Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
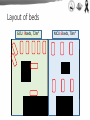
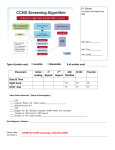
OUTBREAK OF CARBAPENEM-RESISTANT ENTEROBACTERIACEAE (CRE) IN A NEONATAL INTENSIVE CARE UNIT (NICU) Soichiro Kawata1, Manami Ishibashi1, Kaori Ishikawa1, Fumiko Kinoshita1, Katsunori Yanagihara2, Koichi Izumikawa3, Hiroyuki Moriuchi1 1: Department of Pediatrics, Nagasaki University Hospital, Nagasaki, Japan 2: Department of Laboratory Medicine, Nagasaki University Hospital, Nagasaki, Japan 3: Infection Control and Education Center, Nagasaki University Hospital, Nagasaki, Japan Disclosure of Conflict of Interest Name of the speaker: Soichiro Kawata We have no COI with regard to our presentation. Introduction • Neonates, especially those born by C-section, are born sterile. • Neonates in NICU receive antibiotic treatment and undergo various manipulations and procedures. ∴Neonates are vulnerable to colonization and infection with multidrug-resistant bacteria. • Carbapenem-resistant Enterobacteriaceae (CRE), one of the most topical drug-resistant organisms recently, is a great threat especially for children with underlying disease. Dr. Frieden, director of the CDC, said… CRE is “Nightmare bacteria.” CRE outbreak at the NICU in Nagasaki Univ. Hospital CRE outbreak at the NICU in Nagasaki Univ. Hospital Press Reporting Background of our NICU 6 beds in NICU, 9 beds in GCU. Our patients are • Infants who undergo surgical procedure (excluding heart surgeries) or have some underlying disease. • low-birth-weight infants (excluding very-low-birthweight infants) born in-hospital. Layout of beds GCU: 9beds, 72m2 NICU:6beds, 70m2 Onset of Outbreak Oct. 28 29 30 Nov. 31 1 2 3 1 On 3rd November, 2014… CRE colonization was detected in the index case. MIC MIC Ampicillin ≧32 R Cefoperazone/Sulbactam ≧64 R Ampicillin/Sulbactam ≧32 R Latamoxef ≧64 R 4 S Cefmetazole ≧64 R ≦4 S Imipenem/Cilastatin 2 I Cefazolin ≧32 R Meropenem 2 I Cefotiam ≧32 R Aztreonam ≦0.5 S Cefotaxime ≧64 R Gentamicin 8 I Ceftriaxone ≧64 R Amikacin ≦4 S Cefditoren-Pivoxil ≧4 R Minocycline 1 I Cefpodoxime ≧8 R Ciprofloxacin ≦0.5 S Ceftazidime ≧64 R Levofloxacin ≦0.5 S Cefpirome 16 R ST ≦19 S Cefepime 16 R Piperacillin Piperacillin/Tazobactam Enterobacter Cloacae complex (IMP type) CRE was isolated from 16 patients through active surveillance culture. Oct. Nov. Dec. Jan. Feb. Mar. 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 = negative = Enterobacter spp. = Enterobacter spp. (CRE, metallo) = Klebsiella oxytoca (CRE, metallo) Cooperation with Infection Control and Education Center • Active surveillance culture once a week • Behavior monitoring and re-education of staffs • Strict management of medical devices (ex: ultrasound, bronchoscope) • Cleaning of the NICU/GCU, by the NICU/GCU staffs • Consultation to the external expert institutions Infection Control Committee of National and Public University Hospital Field Epidemiology Training Program of National Institute of Infections Disease Major Interventions Hand hygiene practice per 1 patient-day at NICU/GCU (National University Hospitals in Kyushu area in 2014) Total: 145.9 cycles 66% Efficacy of alcohol-based hand rubs on hydrophilic GNR, such as Enterobacter spp. No MRSA hand hygiene strategy →Changed colonization from hand washing to hand rubbing 34% Changing Layout of the NICU/GCU before Started recording of bed positions AFTER “Zoning of patient areas” Each zone includes all tools for daily patient care, such as a hazardous waste box and personal protective equipment (PPE) →stopped sharing tools and using a dirt disposing room. “Cohorting” GCU: 9 beds CRE carriers NICU: 6 beds CRE colonized patients were cared by nurses exclusively in charge of them. 19 Assessment of risk factors significant Risk Factors Cases n=16 Controls (%) n=24 Total (%) n=40 Odds Ratio P value 95%CI upper lower Birth Weight <2,500g 12 80 7 28 40 10.29 <0.005 1.85 Inborn 14 93 11 44 40 17.82 <0.005 1.96 805.86 stayed at only NICU 9 56 3 13 12 9 <0.01 1.55 62.5 Born with C-section 14 88 9 38 23 11.7 <0.01 1.86 121 Tube Feeding 16 100 16 67 32 0.01 1.89 - 6 85.7 1 12.5 7 42 <0.01 2.1 825.7 Mechanical Ventilation 9 56 6 25 15 3.86 0.05 0.83 18.5 CV catheter 16 0.14 0.75 - Surgical Procedure 1 1 0.06 5.86 Antibiotics Usage 12 0.05 0.88 22.6 - 69.57 2014/1/20~3/9 Tube Feeding not significant 20 83 36 Tube feeding 6 4 17 6 0.71 Odds 42.0 4.2 75 10 ratio 42 22 100 • The source of outbreak thought to be based on daily medical procedures. About milk formulae Milk preparation room Dissolving breast milk by warm water • Both new and used feeding bottles are collected to here. • washing, sterilizing and forming of bottles are performed at same place. • formed by nurse during caring patients. Requested nutritionists for milk preparation Major Interventions • Hand hygiene “Washing Rubbing” • Zoning Completion of patient care within each zone • Cohorting Isolation of colonized patients • Counterapproaches based on risk assessment Outsourcing of milk formulae New colonization : 0 Major Interventions • Hand hygiene “Washing Rubbing” • Zoning Completion of patient care within each zone • Cohorting Isolation of colonized patients • Counterapproaches based on risk assessment Outsourcing of milk formulae At the beginning of Feb., Recurrence New colonization : 0 th ―From 14 , Feb. : Ward Closure― After ward closure… Emptying the NICU/GCU • Discharge or Transfer to other institutes • Moved to a Room at Pediatric ward: “Satellite NICU” →on 28th March : No patients in the NICU/GCU • Further interventions 130 points of Environmental Surveillance CRE genes Positive Incubators Patient monitors Dirt disposing room Requested their management to Medical Equipment Center Negative after cleaning th “Cleaning” of NICU/GCU on 7 April 2015 26 130 points of Environmental Surveillance Culture Positive faucets All 4 faucets were renewed. Culture turned to be negative. Re-opened the NICU/GCU • All CRE positive points were confirmed to be negative after the major cleaning. • Restarted partial NICU activity with 2 patients • Had attained full operation on May, 2015 • No relapse of CRE colonization until today. Discussion Looking back at this outbreak • CRE-positive culture of the wash stand: cause or effect? → Whichever the case, thoroughgoing hand rubbing practice decreased the exposure to water in wash stands and improved decontamination of hydrophilic bacteria. • Two patients developed CRE-associated diseases that were successfully treated with tazobactam/piperacillin. →It is noteworthy that beta-lactam antibiotics can induce AmpC, making Enterobacter more powerful resistant bacteria. • Fortunately, spreading of CRE to the other wards was successfully prevented. About interventions • Zoning and Cohorting : It is important to visualize the respective patient zone in an unpartitioned room like our NICU/GCU. • Outsourcing : Understaffing is a risk of outbreak (Andersen et al, 2002). Involvement of other professionals will improve the management. On the other hand, efficacy of the following remains unclear: • Cleaning : Efficacy has been proven for Streptococci and Staphylococci (Bokulich, et al. 2013), but not for GNRs. • Surveillance culture and environmental screening : Efficacy is evident, but cost-effectiveness remains unclear (Williams, el at. 2014). No studies have demonstrated what will be the most effective approach. Conclusion • Once the outbreak has occurred, we cannot help trying all possible interventions. • Apart from cost-effectiveness, the following procedures should be beneficial for early and successful control of the outbreak. Take home message Risk Assessments, Hand Hygiene, Zoning and Active Surveillance Culture must be effective for control. Economically… calculated by Infection Control and Education Center * $ 1 = \ 1 2 0 .8 0 at M ay, 2 0 1 5 Fall in income (Mar.-May, 2015 : compared with 1year before) Replacing faucets $497,004 $8,238 Drain cleaning with high pressure $932 creating "satellite NICU" $287 the other constructions $13,518 Purchasing goods (Defrosting instruments for breast milk etc.) $17,897 PPEs for colonized patients Surveillance culture, cost for LAMP etc. total $8,300 ? $546,175+α The costs for outsourcing (cleaning incubator and washing bottles) $12,550/month from now on!!