Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
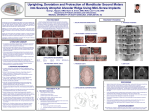
Case Report By Neal D. Kravitz, DMD, MS W hen you are protracting maxillary molars, often anterior dental anchorage or Class III directional elastics are sufficient to consolidate space without affecting incisor position. However, in more challenging cases such as movement through a pneumatized sinus or molar substitution, skeletal anchorage may facilitate efficient molar protraction. This case report presents the treatment of an adolescent patient with early loss of dysplastic maxillary first molars and successful, noncompliant protraction of the second molars using orthodontic miniimplants for anchorage. molars, presence of all third molars, and acceptable condylar head shape bilaterally (Figure 3). Study model analysis revealed a Class II division 1 subdivision right malocclusion, a tapered-maxillary arch, 40% overbite, +4 mm of overjet, and moderate anterior crowding. Treatment Objectives Diagnosis and Etiology A 13-year-old adolescent female was referred by her general dentist for an orthodontic consultation following the recent extraction of severely carious maxillary first molars. The patient presented with a straight soft-tissue profile and good facial symmetry, with the maxillary dental midline left of the facial midline. Intraoral examination revealed missing maxillary first molars, full eruption of the maxillary second molars, 180º malrotation of the maxillary left second premolar, forward position of the maxillary right buccal segment due to the labially displaced maxillary right canine, forward position of the left mandibular buccal segment due to lingually displaced mandibular left lateral incisor, and coinciding dental midlines (Figure 1). As shown in Figure 2, cephalometric analysis confirmed a mild Class II skeletal relationship (SNA: 79º; SNB: 76º). A pretreatment panorex provided by her general dentist revealed large carious lesions with pulpal involvement of the maxillary first Maxillary second molar protraction with mini-implants and a transpalatal arch We identified five treatment objectives: 1)establish functional Class I molar and canine occlusion with normal overbite and overjet; 2)resolve crowding; 3)develop a broader maxillary-arch shape; 4)align the dental midlines with the facial midline; and 5) maintain soft-tissue esthetics. Treatment Alternatives Figure 1: Pretreatment composite. Figure 2: Pretreatment cephalograph. Figure 3: Pretreatment panorex provide by general dentist. Notice the dysplastic first molars (yellow circles). 18 OrthodonticProductsOnline.com February 2011 The patient presented to our office with the maxillary first molars already extracted. Therefore, our treatment options were limited to either holding first-molar spaces for restorative treatment or molar substitution (protracting the second molar into the first molar position). The maxillary left second premolar would not be derotated to avoid prolonging treatment duration and risking pulpal necrosis. In regard to the first treatment option, the maxillary left second premolar would benefit from cuspal coverage; however, no other posterior teeth had carious lesions. Therefore, we did not want to prepare bridgework on healthy teeth. Furthermore, the patient was approximately 4 years from skeletal maturity, and she was not interested in pursuing endosseous dental implants. The second treatment option included protraction of the maxillary second molars into the first molar position. To aid molar protraction, we discussed incorporating orthodontic mini-implants into the palate. Due to the cost savings and the preservation of healthy teeth, this treatment option was chosen by the patient and supported by her referring dentist. Treatment Progress We fitted all teeth, excluding the maxillary first premolars, with fixed, preadjusted edgewise appliances (Rocky Mountain Orthodontics Synergy .018 slot in the anterior and Synergy-R .022 self-ligating slot in the posterior. We ligated .014 NiTi aligning archwires (also from RMO). At 2 months of treatment, we switched to .016 x .022 NiTi archwires for anterior torque and arch development (Figure 4). We placed two RMO Dual-Top mini-implants (6-mm length and 1.6-mm diameter) in the paramedian region of the maxillary palate, in line with the first premolars. We fitted bands on the maxillary first premolars for a pick-up impression to fabricate an AOA Laboratories transpalatal arch spanning premolar-to-premolar. I instructed the laboratory technician to keep the buccal brackets and solder palatal buttons on the bands. After fabrication, we cemented the transpalatal arch with GC Fuji LC, and we added RM Bond flowable composite to secure the mini-implants to the transpalatal bar (Figure 5). After 4 months of treatment, we inserted .017 x 0.025 stainless steel archwires to begin consolidation. We placed buccal and palatal elastic chains (RMO Medium-Energy Chain) for efficient molar protraction. In less than 5 months (December 2007 to April 2008), we achieved complete space closure with minimal crown tipping. After 9 months of treatment, we removed the transpalatal arch and mini-implants, then bracketed the maxillary first premolars. We then performed final arch coordination and minimal occlusal equilibration. Once panoramic evidence confirmed mesial migration of the maxillary third molars into the second molar region, we bonded lingual retainers and took impressions for overlay Hawley retainers. At the debonding appointment, we gave the patient a referral for extraction of the mandibular third molars. The total length of treatment was 16 months. Figure 4: Treatment Montage. A) Upper and lower .014 NiTi wires after bonding. B) Upper and lower .016 x .022 NiTi wires. C) Upper and lower .017 x .025 stainless steel wires. Transpalatal arch has been placed and molar protraction has begun. D) Completion of molar protraction. Figure 5: Treatment Montage, occlusal-view. A) Placement of 1.6- x 6.0-mm mini-implants with a torsional-controlled contra-angled driver. Mini-implants placed in the para-medium region. Two mini-implants were placed to stabilize the transpalatal arch. In critique, the mini-implants should have been placed farther apart for greater stability. Pick-up impression taken after placement of the mini-implants. B) We placed flowable composite to secure the transpalatal arch to the mini-implants, and activated molar protraction with buccal and palatal elastic chains. C) Complete consolidation in less than 5 months. Notice the small space opening distal to the right lateral incisor, indicating a slight loss of anchorage even with the skeletal anchorage system. Treatment Results The results of our treatment were an acceptable Class I relationship and a maintained facial balance (Figure 6). We obtained an appropriate incisal relationship by arch development, distal uprighting of the maxillary anterior teeth, and labial advancement of the mandibular anterior teeth with mild reproximation. Evaluation of Figure 6: Final composite photographs. Notice the second molars fully protracted into a Class I occlusion. Also notice the lingual cusp of the maxillary left second premolar. February 2011 OrthodonticProductsOnline.com 21 pretreatment and posttreatment cephalometric measurements showed significant molar protraction, slight bite opening, and minimal changes in lip position relative to the Esthetic Line (Figure 7). The 6-month posttreatment records showed good retention of the second molars and continued mesial eruption of the maxillary third molars into the second molar position (Figure 8, page 24). odontogenesis. Other environmental factors may include birth-related trauma to the teeth and jaws, trauma during intubation, poor prenatal and postnatal nutrition (specifically, vitamin A and D deficiency), hypoxia, infections, or exposure to toxic chemicals (such as high dosages of fluoride, tetracycline, and lead). Genetic factors include a variety of hereditary conditions such as trisomy 21, cerebral palsy, and metabolic disorders.1 Treatment options of enamel dysDiscussion plasia depend on the severity of the le7: Superimposition. Maxillary second Enamel Dysplasia, sometimes re- Figure sion. Due to the nature of the dysplastic molars and mandibular first molars were traced. ferred to as enamel hypoplasia (EH) or enamel, bonding is often challenging. simply dysplasia, is a defect that results in underdeveloped Conservative treatment may consist of stainless steel crowns, or malformed enamel. Dysplasia can occur on any tooth or composite bonding, or root canal with a full-coverage cast on multiple teeth, though it most commonly presents on the crown. In our patient, due to the large carious lesions with first molars or the central incisors. The enamel defect may pulpal involvement, the general practitioner recommended present itself in a variety of forms, from a small pit-lesion extraction of the dysplastic first molars followed by protracto large orange-brownish mottling of the facial or occlusal tion of the second molars and spontaneous mesial drift of the surface of the tooth. Teeth with enamel dysplasia are often third molars. misshapen, hypersensitive, and may be more susceptible to The literature demonstrates that spontaneous third dental caries.1 molar drift following extraction of second molars is highly The cause of dysplasia may be multifactorial, but the predicable in the maxilla (96.2%) and less predictable in the defect is most commonly associated with infection or fe- mandible (66.2%).2 During eruption, maxillary third molar ver during pregnancy or infancy that may interfere with crowns upright and maintain their angulation as they come 22 OrthodonticProductsOnline.com February 2011 into occlusion. Additional uprighting octreatment overbite, with or without the incurs once molar occlusion is established.2 corporation of a transpalatal arch, would Factors that influence successful thirdhave provided sufficient dental anchorage molar eruption include initial angle of for molar protraction. While placement of eruption, jaw angulation, sex, age, and mini-implants ensured anchorage of the developmental stage of the third molar.3 transpalatal arch, the benefit of this case During the treatment of our patient, the report lies in sharing a method for molar maxillary second molars were protracted protraction that may be more applicable following extraction of the first molars. Figure 8: The final panorex reveals spon- when dental anchorage is insufficient. A post-treatment panoramic radiograph taneous mesial drift of the maxillary third revealed good erupting position and an- molars into the second molar position. The Conclusions patient was referred for extraction of the gulation of the maxillary third molars. Indirect skeletal anchorage with an mandibular third molars. To aid efficient molar protraction, anterior transpalatal arch can provide efwe incorporated indirect skeletal anchorage using an ante- ficient, noncompliant maxillary molar protraction. The prorior transpalatal arch. Indirect skeletal anchorage is often traction of maxillary second molars after early loss of first preferable to direct anchorage when protracting posterior molars, and the subsequent mesial drift of the third molars, teeth for two reasons: allows for the reestablishment of Class I molar occlusion 1) greater biomechanical control, because forces are di- without costly posterior restorative treatment. OP rected along a continuous archwire; and 2) greater patient safety, because the mini-implant can Neal D. Kravitz, DMD, MS, is in private practice in South be placed in a variety of locations. Riding, Va, and White Plains, Md. He is a Diplomate The palate is a preferable location for indirect skeletal of the American Board of Orthodontics, and is on the anchorage due to its dense cortical bone, attached tissue faculty at the University of Maryland and Washington coverage, and low risk probability.4 Hospital Center. He would like to References for this article can With this said, mini-implants were thank the orthodontic residents at arguably not necessary to aid successbe found with the online version the University of Maryland for their ful molar protraction in this particular editorial guidance. He can be reached at OrthodonticProductsOnline.com. case. It is likely that the depth of preat [email protected]. 24 OrthodonticProductsOnline.com February 2011