Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
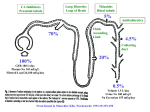
RATIONAL USE OF DIURETICS AND PATHOPHYSIOLOGY OF EDEMA 12 : 1 OP Kalra, Amitesh Aggarwal, Delhi Introduction The use of diuretics for therapeutic purposes is not new. They were used for the treatment of dropsy as early as 16th century. Diuretic drugs increase urine output by the kidney by altering sodium handling. Increased sodium excretion by kidneys leads to increase in water excretion. Most diuretics produce diuresis by inhibiting the reabsorption of sodium at different segments of the renal tubular system. Diuretic use in clinical practice spans conditions like edema, hypertension, metabolic acidosis and hyperkalemia. Patients with nephropathy or heart failure may have a 10 to 30% increase in extracellular and blood volume, even in the absence of overt edema1. Classification Multiple classes of diuretics are available for use including loop diuretics, thiazides and potassiumsparing diuretics. The level of GFR and need and urgency for reduction in ECF volume dictates the choice of diuretic agent. Thiazide diuretics Thiazide diuretics inhibit the apical Na+-Cl- cotransport system in the distal tubule. Metabolism of thiazide diuretics is variable. Bendroflumethiazide and indapamide are primarily metabolized by the liver; while hydrochlorothiazide and metolazone are metabolized by the kidney. They are delivered to their luminal site of action by organic anion transporters in the straight segment of the proximal tubule, consequent of their extensive protein binding. Considerable protein binding makes role of glomerular filtration inconsequential in entry of thiazide diuretic into the urinary space. Loop diuretics Loop diuretics act by inhibiting the Na+-K+-2Cl- cotransporter in the thick ascending limb of the loop of Henle delivered to their luminal site of action by organic anion transporters. By blocking the transporter in the cortical segments, the loop diuretics enhance free water clearance. The bioavailability of loop diuretics is not affected by renal insufficiency. On an average, 50% (range 10-100%) of an orally administered dose of furosemide is absorbed2. In contrast, absorption of bumetanide and torsemide, is nearly complete (80- 100%). Loop diuretics are primarily bound to albumin. Torsemide is approximately 80% cleared by the liver. Bumetanide is approximately 50% metabolized by the liver and its half-life does not appreciably change in kidney failure. Approximately 50% of the dose of furosemide is excreted unchanged; the remainder is conjugated to glucuronic acid in the kidney. Therefore, in patients with kidney failure, the plasma half-life of furosemide is prolonged. Potassium sparing diuretics There are two principal types of potassium-sparing diuretics, those that inhibit epithelial sodium channels (triamterene and amiloride) and those that inhibit mineralocorticoid receptors (aldosterone antagonists). For both types, the site of action is in the collecting tubule. The absorption of potassiumsparing diuretics is quite variable. The total protein binding is low for amiloride and high for spironolactone. Amiloride and triamterene undergo significant excretion by the kidney, both by glomerular filtration and tubular secretion by the organic cation secretory pathway. Spironolactone 601 Medicine Update 2012 Vol. 22 is metabolized by the liver; its pharmacokinetic property is not significantly affected by chronic kidney disease (CKD). Loop Thiazide Potassium sparing Pharmacodynamic effects Increases excretion of Na, K, Ca, Mg Increases excretion of Na, K, Mg, decrease excretion of Ca Increases excretion of Na, decrease excretion of Ca, K, Mg Site of action Thick ascending Distal tubule limb Transporters affected Na+ K+ 2Cl- co transporter Collecting tubule Apical Na+ Cl- co Epithelial Na+ transporter channels or mineralocorticoids receptors % of filtrate 20-30% reabsorbed at site of action 6-11% < 5% Bioavailability 40-90% 30-90% 50-100% (Adapted from K/DOQI clinical practice guidelines on hypertension and antihypertensive agents in chronic kidney disease) Am J Kidney Dis. 2004 May; 43(5 Suppl 1):S1-290) Pathophysiology of edema Cardiac: Fluid retention is a consistent finding in almost all acute and most chronic heart failure patients. It manifests as pulmonary and peripheral edema. The pathophysiology of edema in heart failure involves the activation and interplay of multiple neurohumoral and cellular systems. Pathobiologically important alterations occur in the sympathetic nervous system, the renin-angiotensin-aldosterone system (RAAS), the vasopressin axis, and vasodilatory/ natriuretic pathways. These disturbances are translated at the renal circulatory and tubular level in such a way that avid retention of sodium and water occurs3. The state of the arterial circulation, as governed by cardiac output and peripheral vascular resistance, is the chief determinant of sodium and water retention in heart failure4. In particular, either a primary decrease in cardiac output or arterial vasodilatation brings about arterial underfilling, which activates neurohumoral reflexes that in turn incite sodium and water retention. Sympathetic nervous system activity contributes to peripheral and renal vasoconstriction and to sodium and water retention. Activation of renal sympathetic nerves leads to angiotensin II release, stimulating the reninangiotensin-aldosterone system. Sympathetic stimulation also prompts release of arginine vasopressin, excess levels of which lead to water retention and hyponatremia. Angiotensin II acts as a potent vasoconstrictor, stimulates aldosterone release from the adrenal gland, and promotes renal tubule sodium reabsorption. Aldosterone increases reabsorption of sodium in the collecting duct. free water excretion leads to extracellular volume expansion and total body volume overload manifesting clinically when the GFR falls to less than 10-15 mL/min. As kidney function declines further, peripheral edema and pulmonary edema appears. At a higher GFR, excess sodium and water intake could result in a similar picture if the ingested amounts of sodium and water exceed the available potential for compensatory excretion. The interstitial inflammation of the kidney has a key role in the pathogenesis of nephrotic edema by inducing primary sodium retention. Both decrease in sodium filtration and increase in net sodium reabsorption occur due to generation of vasoconstrictive substances in the interstitium, driven by the inflammatory cell infiltrate. Reduction in plasma oncotic pressure also plays a key role in the pathogenesis of edema. Thus, hypoalbuminemia effectively buffers the hemodynamic effects of acute increments in blood volume as the fluid overload is sequestered into the tissues5 and is responsible for the fact that while patients with acute glomerulonephritis show a steep relationship between weight gain and the humoral response, indicating plasma expansion, the patients with nephrotic syndrome do not6. Low plasma colloid oncotic pressure and primary sodium retention combine to overwhelm the mechanisms protecting from changes in interstitial volume7-10 and drive the development of edema (Fig. 1). Hepatic: Patients with cirrhosis of liver share a common pathophysiology of arterial underfilling secondary to decreased cardiac output and decreased systemic vascular resistance, respectively, with eventual stimulation of neurohumoral axis and sodium and water retention. The resultant renal vasoconstriction and sodium and water retention lead to ascites and hepatorenal syndrome in advanced cirrhosis. Two key PROTEINURIA Tubulointerstitium Infiltration T cells, MФ ↑ All, ↓ NO Renal: Chronic renal insufficiency (CRI) leads to alteration in salt and water handling by the kidney. Failure of sodium and 602 ↑ Na reabsorption Primary Na retention Glomeruli HYPOALBUMINEMIA ↓ Kf ↓ SNGFR ↓ Filtered Na ↓ UNa V Secondary Na retention Intravascular volume ↑PC Overwhelmed mechanisms of edema removal ↓ PCOP EDEMA Fig. 1: Overview of pathophysiology of edema formation in nephrotic syndrome. (Adapted from Rodríguez-Iturbe B, HerreraAcosta J, Johnson RJ. Interstitial inflammation, sodium retention, and the pathogenesis of nephrotic edema: A unifying hypothesis. Kidney Int 2002; 62: 1379–1384.) Rational Use of Diuretics and Pathophysiology of Edema factors are involved in the pathogenesis of ascites formation— sodium and water retention, and portal hypertension. There is an overlap between CKD and heart failure11, having a complex bidirectional pathophysiologic state12 that worsens the function of both organs known as cardio renal syndrome (CRS). In Chronic CRS (Type 2), longstanding heart failure leads to progressive CKD, possibly via episodes of acute kidney injury (AKI). Optimal management of sodium and extracellular fluid volume through low-sodium diet and diuretics is important in prevention of chronic CRS. Many studies indicate that the lowest doses of loop diuretics necessary to maintain hemodynamics are optimal13. Conversely, those patients requiring the highest doses of loop diuretics have the highest rates of CRS and mortality probably by further activation of neurohumoral pathways14. Another form of chronic CRS (Type 4) may be recognized who have repetitive bouts of cardiac ischemia and injury reflected by chest pain, electrocardiogram changes and elevations in cardiac biomarkers. In this form of CRS, worsening kidney function reduces the effectiveness of diuretics. Rationale for use Cardiac disease: In heart failure, loop diuretics may improve cardiac function by decreasing cardiac filling pressure, functional mitral insufficiency, ventricular wall stress, and endomyocardial ischemia. In some patients, this may also lead to improved renal function. In patients with acute left heart failure, pulmonary edema is the main abnormality and is usually treated with intravenous loop diuretics. The improvement in symptoms and the accompanying reduction in filling pressures occur even before diuresis is initiated and have been attributed to vasodilatation15. Renal diseases: In CKD, they reduce ECF volume, lower blood pressure, potentiate the effects of ACE inhibitors, ARBs, and other antihypertensive agents; and reduce the risk of cardiovascular disease in CKD. The addition of diuretics and calcium channel antagonists to RAS inhibitor therapy is also considered to be a rational strategy to reduce blood pressure and preserve renal function. Extracellular fluid volume overload as a result of sodium retention is one of the major causes of hypertension in renal disease16,17. In principle, the mechanism of decreased sodium excretion in CKD is reduced glomerular filtration of sodium, increased tubular reabsorption of sodium, or both. Diuretics act primarily by decreasing tubular sodium reabsorption, thereby increasing sodium excretion, reversing extracellular fluid volume expansion, and lowering blood pressure. Diuretics potentiate the antihypertensive effects of ACE inhibitors and ARBs by stimulating renin and reducing fluid volume, thus making blood pressure more sensitive to the action of these agents16-19. A randomized study designed specifically to test the effectiveness of a diuretic-based treatment on microalbuminuria in diabetic patients with hypertension found that diuretic-based therapy was equivalent to an ACE inhibitor-based therapy20. It is generally recommended that patients with chronic renal disease receive a diuretic along with an ACE inhibitor or ARB as part of the strategy to reach target blood pressure16,21,22. Increased rate of fluid delivery and reabsorption per nephron in the loop segment and relative preservation of the target transporters is a critical factor in the retained efficacy of loop diuretics even in advanced renal insufficiency. On the other hand, thiazide diuretics when used alone become relatively ineffective in patients with a moderate to severe degree of CRI (creatinine clearance < 35 ml / min), although high doses of thiazide diuretics, such as metolazone, do retain some efficacy in even advanced CRI23. Loop diuretics have been prescribed to patients with endstage renal disease (ESRD) in an attempt to slow the rate of loss of GFR. An observational study of 125 patients with ESRD treated by peritoneal dialysis (PD) showed that total sodium and fluid removal by PD were powerful predictors of longer survival24. In contrast, a controlled clinical trial of the effects of furosemide in patients treated with continuous ambulatory peritoneal dialysis (CAPD) showed no benefit of regular diuretic therapy in delaying the loss of residual renal function25. Thus, optimal dialysis, rather than loop diuretic therapy is the best treatment for these patients. Relevant clinical issues Maximum dose of diuretics Diuretic action relies on an adequate amount of the drug reaching its site of action at the renal tubule. Once present in the circulation, a diuretic must gain entry into the renal tubule in a sufficient concentration to exceed the threshold for response; thereafter, there exists an optimal rate of drug delivery leading to a rate of a maximal response. Additional diuretic delivery does not produce a greater response26,27. High doses of furosemide can increase urine production in patients with chronic renal failure28. The effects in hemodialysis patients are equivocal. Chronic administration of the drug in doses ranging from 250 to 500 mg orally in these patients has been associated with a remarkably long duration of residual urine production. High dose furosemide increases the urinary excretion of sodium, chloride, and water in CAPD patients without affecting GFR, urea clearance, and creatinine clearance29. Combination therapy In patients with nephrotic syndrome, addition of thiazides to furosemide markedly increases natriuresis30,31. But this finding contrasts with repeated recommendations to withhold thiazides in such patients because of their assumed inefficacy32,33. On pharmacokinetic principles, it is usually not 603 Medicine Update 2012 Vol. 22 advisable to combine substances with different half-lives of action. In the particular case of loop diuretics (short half-life) and thiazides (long half-life) this approach may, however, have distinct advantages. First, co-administration of thiazide and loop diuretics may help to overcome “resistance” to the action of conventional therapeutic doses of loop diuretics which is frequently observed in patients with advanced renal failure34,35. Administration of high doses of loop diuretics may cause more frequent and severe side effects36. Coadministration of thiazide diuretics may therefore permit use of smaller doses of loop diuretics and this may reduce the frequency of side effects. Second, because of the long halflives, the duration of action of thiazides outlasts that of loop diuretics and thus prolongs the overall duration of natriuresis. Third, administration of a thiazide may interfere with the socalled “rebound effect” following loop diuretic treatment, that is, with antinatriuresis after the short acting natriuretic effect of the loop diuretic has waned37,38. Continuous vs bolus administration There are potential benefits of continuous infusion when compared with intermittent bolus dosing. Bolus diuretic dosing may be associated with a higher rate of diuretic resistance due to prolonged periods of subtherapeutic drug levels in the kidney. Continuous infusion results in a more constant delivery of diuretic to the tubule, potentially reducing this phenomenon. Additionally, continuous infusion is associated with lower peak plasma concentrations, which may be associated with a lower incidence of other side effects such as ototoxicity, especially at higher doses. A recent meta-analysis from the Cochrane Collaboration comprehensively addresses this question and reviewed studies including a total of 254 patients39-42. Continuous infusion was associated with greater urine output, shorter length of hospital stay, less impairment of renal function, and lower mortality when compared with intermittent bolus dosing. In the Diuretic Optimization Strategies Evaluation (DOSE) study, among patients with acute decompensated heart failure, there were no significant differences in patients’ global assessment of symptoms or in the change in renal function when diuretic therapy was administered by bolus as compared with continuous infusion or at a high dose as compared with a low dose43. In patients who have poor response to intermittent doses of a loop diuretic, a continuous intravenous infusion can be tried. If an effective amount of the diuretic is maintained at the site of action at all times, a small but clinically important increase in the response may occur36. Before administering a continuous infusion of a loop diuretic, the physician should give a loading dose in order to decrease the time needed to achieve therapeutic drug concentrations; otherwise, 6 to 20 hours is required to achieve a steady state, depending on the diuretic used. The frequency of administration of diuretic is determined by its plasma half life. In case of administration of shortacting loop diuretic, sodium reabsorption is increased shortly after the diuretic effect has waned, which may be sufficient to completely nullify the gain from the prior natriuresis. This rebound antinatriuretic effect (braking phenomenon) attenuates the normal dose-response relationship and can last several hours, thus limiting the efficacy of therapy. It can be overcome by administering multiple daily doses of the diuretic44. Predosing for metolazone The recommendation for pre-dosing metolazone is based solely on the pharmacodynamic rationale of delayed onset of action observed following a single orally administered metolazone dose45. Given the lengthy half-life of metolazone, this delayed onset is unlikely to be a concern during ongoing chronic treatment, particularly once steady-state is achieved. However, no published clinical studies have compared predosing to simultaneous dosing. At present, the practice of predosing metolazone prior to a loop diuretic is not supported by the literature. Diuretic resistance Refractoriness to diuretics in heart failure is due to blunting of relationship between urinary sodium excretion and the urinary diuretic excretion rate compared with normal subjects. Typically, heart failure patients with mild to moderate disease have a response that is one fourth to one third of that normally observed with maximally effective doses of loop diuretics. The threshold for effect is noticeably increased. Multiple factors lead to diuretic resistance in CKD. The factors may be increased tubular reabsorption of sodium, use of non-steroidal anti-inflammatory agents, increased plasma levels of organic anions and urate, and metabolic acidosis impairing proximal tubule secretion of diuretics. High dietary intake of sodium may lead to apparent diuretic resistance. The “braking phenomenon” (post diuretic sodium retention) describes avid sodium retention that can develop in response to a rapid diuresis due to hemodynamic and neurohumoral changes produced, thereby limiting response to further doses of diuretics. The braking phenomenon may occur during either short-term or long-term therapy. In CKD, the tubular secretory capacity for a diuretic is lowered in parallel with the reduction in GFR warranting requirement of higher blood levels to affect tubular delivery sufficient to prompt a diuresis. Several mechanisms may contribute to diuretic resistance in nephrotic syndrome, including intratubular binding of loop diuretic by filtered albumin, decreased GFR, excessive tubular reabsorption of sodium at site proximal to the loop of Henle, or a disease state-related resistance to diuretic action at the cellular level. These patients have an impaired response 604 Rational Use of Diuretics and Pathophysiology of Edema to loop diuretics and there is reduced tubular sensitivity and responsiveness to diuretics. Many patients with advanced nephrotic syndrome have a marked stimulation of plasma renin activity, especially during diuretic therapy. The ensuing hyperaldosteronism further reinforces NaCl reabsorption in the distal nephron and collecting ducts. Four pharmacokinetic mechanisms that could impair the responsiveness to loop diuretics in patients with the nephrotic syndrome are decreased renal diuretic delivery, decreased peritubular diuretic uptake, enhanced renal metabolism of furosemide to the inactive glucuronide and decreased free diuretic levels in tubular fluid. Treatment of nephrotic syndrome may require high doses of loop diuretics, a combination of loop and thiazide diuretics, or loop diuretics with albumin infusions. With long-term administration of a loop diuretic, the solute that escapes from the loop of Henle floods more distal regions of the nephron. By unknown mechanisms, increased exposure to solute causes hypertrophy of distal nephron segments, with concomitant increases in the reabsorption of sodium38,46,47. Sodium that escapes from the loop of Henle is therefore reabsorbed at more distal sites, decreasing overall diuresis resulting in longterm tolerance to loop diuretics. Thiazide diuretics block the nephron sites at which hypertrophy occurs, accounting for the synergistic response to the combination of a thiazide and a loop diuretic44,48. Newer methods of delivery In nephrotic syndrome, the efficacy of diuretic therapy may be increased by administering a mixture of albumin and a loop diuretic; in several patients with severe hypoalbuminemia, an infusion of 30 mg of furosemide mixed with 25 g of albumin enhanced diuresis49. However, in most patients with the nephrotic syndrome50,51, renal tubular secretion of furosemide is normal (unless the patient also has renal insufficiency), and combined infusions are therefore unnecessary. This conclusion may not be applicable to patients with serum albumin concentrations of less than 2 g per deciliter. In such patients, it may be reasonable to try combined infusions. Diuretic therapy in diverse clinical settings Acute kidney injury In the acute care setting, loop diuretics are often prescribed to maintain or increase urine output. Furosemide and other loop diuretics reduce oxygen demand in the medullary thick ascending limb and attenuate the severity of acute kidney injury in animal models52. They may protect the human kidney from ischemic injury. There have been several small, randomized, controlled trials of diuretics for the treatment or prevention of AKI in various clinical settings. Some studies showed a reduction in dialysis requirement53, reduced urinary albumin and N-acetyl glucosaminidase concentration54, or improved dialysis free survival in oliguric patients56. Others, however, showed either worsened renal function56-58 or no difference in various measured outcomes59-62. Mehta et al.63 published an observational study of diuretic use in patients with AKI in the setting of critical illness and showed that, using multivariate analysis and propensity scores, the use of diuretics was associated with an increased risk of death. However, another analysis by Uchino et al refuted this claim and found that diuretic use in critically ill patients with acute kidney injury is not associated with higher mortality64. Hypertension Many physicians consider thiazides the diuretics of choice for long-term therapy. On average, after adjustment for reductions seen with the use of placebo, thiazides induce a reduction in the systolic and diastolic blood pressures of 10 to 15 mm Hg and 5 to 10 mm Hg, respectively. Hypertension responding preferentially to thiazides is considered to be low-renin or salt-sensitive hypertension. The elderly, blacks, and patients with characteristics associated with high cardiac output (e.g., obesity) tend to have this type of hypertension. Thiazides potentiate the action of other antihypertensive agents when they are used in combination, often producing an additive decrease in blood pressure. For many hypertensive patients, several agents will be needed to achieve desired blood-pressure targets. Combination regimens that include a thiazide can achieve therapeutic synergy while minimizing adverse effects65. Combined meta-analyses and systematic reviews report that, as compared with placebo, thiazide-based therapy reduces relative rates of heart failure (by 41 to 49%), stroke (by 29 to 38%), coronary heart disease (by 14 to 21%), and death from any cause (by 10 to 11%)66-68. Despite a long, well-established record of efficacy, the role of thiazides in hypertension therapy continues to provoke debate69. Based on the benefits observed in studies in which thiazides were used as initial therapy in a stepped-care approach, with agents added sequentially, guidelines for hypertension therapy in the United States have advocated thiazides as initial treatment65. In contrast, British guidelines recommend diuretics more selectively, such as for use in the elderly and blacks70. European guidelines endorse several antihypertensive agents, including diuretics, as initial therapy71. An update from the Joint National Committee is anticipated in the near future. Heart failure Loop diuretics are recommended as the first line of therapy as per the updated guidelines by Heart Failure Society of America72. The use of loop diuretics in heart failure may be a double-edged sword. There is, however, a meta-analysis of 3 small randomized trials that concludes a benefit of diuretics on mortality73. The use of diuretics in some cardiac failure patients 605 Medicine Update 2012 Vol. 22 occasionally may lead to deterioration of renal function. In general, compared with normal individuals, patients with heart failure need higher doses of loop diuretics to achieve a similar sodium excretion, and the magnitude of the “maximal” response is attenuated74. A low sodium diet (less than 2.4 g sodium) and fluid restriction (less than 1.5 l fluid) can reduce the need to use higher doses in advanced heart failure. Non-steroidal anti-inflammatory drugs blunt the effects of diuretics and should be avoided. Diuretics are the mainstay of therapy for symptomatic chronic heart failure but are now rarely used as monotherapy. Together with angiotensin converting enzyme inhibitors they improve patients’ symptoms and in most cases also improve their effort tolerance75. Thiazide diuretics can be used in milder cases, particularly if there is no renal impairment. However, in more symptomatic patients (NYHA III–IV) and in patients with renal impairment, loop diuretics are more useful owing to their relatively strong diuretic action and fewer side effects76. Consistent with pathophysiological process, evidence for pleiotropic benefits of mineralocorticoid blockade is rapidly emerging. The analysis of SOLVD revealed a significantly lower risk for hospitalization and/or death from heart failure, cardiovascular mortality, and all-cause mortality when a potassium-sparing diuretic was used alone or in combination with a non–potassium-sparing diuretic77. Eplerenone is a novel agent that selectively blocks the mineralocorticoid receptor and not those for glucocorticoids, progesterone, or androgens78. It has also been shown to reduce morbidity and mortality in patients with acute myocardial infarction complicated by left ventricular dysfunction and heart failure79. Ascites Loop and distal diuretics are the basic drugs for the treatment of ascites. Management of ascites is based on improving the renal sodium excretion with diuretics and dietary sodium restriction. Despite the natriuretic potency of loop diuretics being greater than other diuretics, only half of the nonazotemic cirrhotic patients have satisfactory natriuresis76,80. Reasons for this poor diuretic effect include reduced tubular secretion of furosemide into the lumen, decreased delivery of fluid to the loop of Henle secondary to enhanced proximal sodium reabsorption, and hyperaldosteronism. In a comparative trial in patients with cirrhosis, spironolactone was found to be more effective than furosemide. Thus, patients with marked hyperaldosteronism did not respond to furosemide and required high doses of spironolactone (400 to 600 mg/day)76. Generally, a ‘‘stepped care’’ approach is used in the management of ascites starting with modest dietary salt restriction, together with an increasing dose of spironolactone. Frusemide is only added when 400 mg of spironolactone alone has proved ineffective81-83. Chronic kidney disease The choice of diuretics is guided by both the status of ECF volume in the patient and the stage of CKD. Thiazide diuretics can be used in CKD Stages 1-3. In the recommended doses, thiazides are effective in generating diuresis in patients with GFR > 30 mL/min/1.73 m2 84. They may lower blood pressure and reduce cardiovascular risk by mechanisms in addition to reduction in ECF volume. Chlorthalidone is longer-acting than hydrochlorthiazide, resulting in better blood pressure control, but causing higher incidence of hypokalemia. Chlorthalidone may be effective at a lower GFR than hydrochlorthiazide. If blood pressure control worsens or if volume expansion occurs as CKD progresses from Stages 1-3 to Stages 4-5 during treatment with a thiazide diuretic, a loop diuretic should be substituted for the thiazide diuretic. Unlike other thiazide diuretics, metolazone retains effectiveness at GFR below 30 mL/min/1.73 m2. Once metolazone has effected a diuresis, it can typically be dosed as infrequently as two to three times a week because of its very long half-life44. Loop diuretics can be used in all stages of CKD and hence are the most commonly used diuretics. The maximal natriuretic response occurs with intravenous bolus doses of 160 to 200 mg of furosemide, or the equivalent doses of bumetanide and torsemide. Larger doses have little incremental value85. Loop diuretics are not as effective as thiazide diuretics in lowering blood pressure in CKD Stages 1-3. In CKD Stages 4-5, loop diuretic therapy is a useful adjunct therapy in the treatment of hypertension. One may use the most bioavailable drug, torsemide, when using the oral route and the drug with the least hepatic elimination, furosemide, when using the intravenous route. Potassium-sparing diuretics must be used with caution in CKD consequent to risk of hyperkalemia. The risk is especially high in patients with GFR < 30 mL/min/1.73 m2 receiving concomitant therapy with ACE inhibitors or ARBs or other conditions that raise serum potassium. Indications for potassium-sparing diuretics in CKD are persistent hypokalemia or resistant hypertension86. The presence of hyporeninemic hypoaldosteronism is a contraindication to their use. Adverse effects Loop diuretics may have detrimental effects in patients with heart failure. Administration of loop diuretics may result in a significant decrease in glomerular filtration rate in some patients with heart failure, presumably due to reninangiotensin-aldosterone system and sympathetic nervous system activation with related changes in renal blood flow and glomerular filtration pressure11,87,88. New-onset diabetes has been reported in patients receiving 606 Rational Use of Diuretics and Pathophysiology of Edema thiazides; however, newly diagnosed diabetes occurs over time in many hypertensive patients, regardless of which class of antihypertensive agent is used. Use of thiazides over several years may lead to an excess of 3 - 4% of new cases of diabetes as compared with other antihypertensive agents 82 . But no analyses of ALLHAT data have indicated that the development of diabetes obviates the benefit of the thiazide89. Depending upon the site and mode of action, some diuretics increase excretion of potassium, chloride, calcium, bicarbonate, or magnesium. Some can reduce renal excretion of electrolyte-free water, calcium, potassium, or protons. Consequently, electrolyte and acid-base disorders commonly accompany diuretic use. Except for the mildly natriuretic collecting duct agents, which are used mainly to limit potassium excretion, all diuretics can cause volume depletion with prerenal azotemia. Loop agents and thiazides, produce hypokalemic and hypochloremic metabolic alkalosis. Carbonic anhydrase inhibitors produce less hypokalemia and volume depletion but at the cost of inducing metabolic acidosis that is often symptomatic. The potassium-sparing agents like spironolactone may also produce metabolic acidosis. Hyperkalemia is a leading complication of the potassium-sparing agents, especially in patients with an underlying tendency. Whether diuretic-induced hypokalemia increases cardiovascular risk is controversial. All diuretics promote excretion of sodium. Hyponatremia, a frequent accompaniment of use of loop agents and thiazides may cause permanent neurologic damage, especially with thiazides use. Loop agents may cause dose-related reversible or irreversible ototoxicity. Some diuretic agents have the potential to cause nephrocalcinosis, nephrolithiasis, hypomagnesemia, and hyperuricemia. Reported idiosyncratic reactions to diuretics include interstitial nephritis, noncardiogenic pulmonary edema, pancreatitis, and myalgias90. Conclusion Multiple classes of diuretics are available for use including loop diuretics, thiazides and potassium-sparing diuretics with use primarily focused in edema of various causes. The pathophysiology of edema involves the activation and interplay of multiple neurohumoral and cellular systems with alterations in the sympathetic nervous system, the reninangiotensin-aldosterone system, the vasopressin axis, and vasodilatory/ natriuretic pathways. These disturbances are translated at the renal circulatory and tubular level in such a way that avid retention of sodium and water occurs resulting in edema. High doses of loop diuretics can increase urine production in patients with chronic renal failure. Loop diuretics combined with thiazides have distinct advantages especially in resistant cases. Continuous infusion of loop diuretics offer potential benefits compared with intermittent bolus dosing. Treatment of diuretic resistance may require high doses of loop diuretics, a combination of loop and thiazide diuretics, or loop diuretics with albumin infusions. The level of GFR and need for reduction in ECF volume dictates the choice of diuretic agent. Electrolyte and acid-base disorders commonly accompany diuretic use and thus their use should be prudent and in tune with the clinical profile of the patient. References 1. Mitch WE, Wilcox CS: Disorders of body fluids, sodium and potassium in chronic renal failure. Am J Med 1982; 72: 536–550. 2. Murray MD, Haag KM, Black PK, Hall SD, Brater DC. Variable furosemide absorption and poor predictability of response in elderly patients. Pharmacotherapy 1997; 17:98-106. 3. Peters JP. The role of sodium in the production of edema. N Engl J Med 1948; 239:353–362. 4. Wiemer G, Fink E, Linz W, et al. Furosemide enhances the release of endothelial kinins, nitric oxide and prostacyclin. J Pharmacol Exp Ther 1994; 271:1611–1615. 5. Koomans HA, Braam B, Geers AB, et al. The importance of plasma proteins for blood volume and blood pressure homeostasis. Kidney Int 1986; 30:730–735. 6. Rodriguez-Iturbe B, Colic D, Parra G, et al. Atrial natriuretic factor in the acute nephritic and nephrotic syndromes: Contrasting patterns of response. Kidney Int 1990; 38:512–517. 7. Koomans HA, Geers AB, Dorhout Mees EJ, et al. Lowered tissue fluid oncotic pressure protects the blood volume in the nephrotic syndrome. Nephron 1986; 42:317–322. 8. Oqvist BW, Rippe A, Tencer J, Rippe B. In vivo microvascular clearance of albumin in renal and extrarenal tissues in puromycin aminonucleoside (PAN) nephrotic syndrome. Nephrol Dial Transplant 1999; 14:1898–1903. 9. Rostoker G, Behar A, Lagrue G. Vascular permeability in nephrotic edema. Nephron 2000; 85:194–200. 10. Schrier RW, Abraham WT. Hormones and hemodynamics in heart failure. N Engl J Med 1999; 341:577–585. 11. Ronco C, McCullough PA, Anker SD, et al. Cardio-renal syndromes: report from the consensus conference of the acute dialysis quality initiative. Eur Heart J 2009; 31: 703–711. 12. McCullough PA. Cardiorenal risk: an important clinical intersection. Rev Cardiovasc Med 2002; 3: 71–76. 13. Hasselblad V, Gattis Stough W, Shah MR et al. Relation between dose of loop diuretics and outcomes in a heart failure population: results of the ESCAPE trial. Eur J Heart Fail 2007; 9: 1064–1069. 14. Metra M, Nodari S, Parrinello G et al. Worsening renal function in patients hospitalised for acute heart failure: clinical implications and prognostic significance. Eur J Heart Fail 2008; 10: 188–195. 15. Packer M, Cohn JN. Consensus recommendations for the management of chronic heart failure. Am J Cardiol 1999; 83(2A):1–38A. 16. Kidney Disease Outcomes Quality Initiative (K/DOQI). Clinical practice guidelines on hypertension and antihypertensive agents in chronic kidney disease. Am J Kidney Dis 2004; 43(5 Suppl 1):S1290. 17. Bidani AK, Griffin KA. Pathophysiology of hypertensive renal 607 Medicine Update 2012 Vol. 22 damage: implications for therapy. Hypertension 2004; 44: 595601. 18. Abbott K, Basta E, Bakris GL. Blood pressure control and nephroprotection in diabetes. J Clin Pharmacol 2004; 44: 431-438. 19. Bakris GL, Williams M, Dworkin L, et al. Preserving renal function in adults with hypertension and diabetes: a consensus approach. National Kidney Foundation Hypertension and Diabetes Executive Committees Working Group. Am J Kidney Dis 2000; 36: 646-661. 20. Marre M, Puig JG, Kokot F, et al. Equivalence of indapamide SR and enalapril on microalbuminuria reduction in hypertensive patients with type 2 diabetes: the NESTOR Study. J Hypertens 2004; 22: 1613-1622. 21. Chobanian AV, Bakris GL, Black HR, et al. Seventh report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure. Hypertension 2003; 42: 1206-1252. 22. Guidelines Committee, 2003 European Society of Hypertension. European Society of Cardiology guidelines for the management of arterial hypertension. J Hypertens 2003; 21: 1011-1053. 23. Dargie HJ, Allison ME, Kennedy AC, Gray MJ: High dosage metolazone in chronic renal failure. Br Med J 1972; 4: 196–198. 24. Ates K, Nergizoglu G, Keven K, et al. Effect of fluid and sodium removal on mortality in peritoneal dialysis patients. Kidney Int 2001; 60: 767–776. 25. Medcalf JF, Harris KP, Walls J. Role of diuretics in the preservation of residual renal function in patients on continuous ambulatory peritoneal dialysis. Kidney Int 2001; 59: 1128–1133. 26. von Vigier RO, Zberg PM, Teuffel O, Bianchetti MG. Preliminary experience with the angiotensin II receptor antagonist irbesartan in chronic kidney disease. Eur J Pediatr 2000; 159:590-593. 27. Weber M: Clinical safety and tolerability of losartan. Clin Therapeutics 1997; 19: 604-616. 28. Brater DC, Anderson SA, Brown–Cartwight DPA. Response to furosemide in chronic renal insufficiency: rationale for limited dosages. Clin Pharmacol Ther 1986; 40:134–9. 29. Faller B, Lameire N. Evolution of clinical parameters and peritoneal function in a cohort of CAPD patients followed over 7 years. Nephrol Dial Transplant 1994; 9:280–6. 30. Nakajiama H, Orita Y, Yamazaki M, et al. Pharmacokinetic and pharmacodynamic interactions between furosemide and hydrochlorthiazide in nephrotic patients. Nephron 1998; 49:223-227. 31. Olesen KH, Dupont B, Flensted-Jensen E. The combined diuretic action of quinetazone and furosemide in congestive heart failure. Acta Med Scand 1970; 187:33-40. 32. Wilcox CS: Diuretics, in The Kidney, edited by Brenner BM, Rector FC, Philadelphia, WB Saunders, 1991; pp. 2123-2147. 33. Rose BD. Diuretics. Kidney Int 1991; 39:336-352. 34. Oster JR. Epstein M, Smoller S. Combined therapy with thiazide type and loop diuretic agents for resistant sodium retention. Ann Intern Med 1983; 99:405-406. 35. Brater DC. Resistance to loop diuretics: Why it happens and what to do about it. Drugs 1985; 35:27-43. 36. Rudy DW, Voelker JR, Green PK, Esparza FA, Brater DC. Loop diuretics for chronic renal insufficiency: A continuous infusion is more potent than bolus therapy. Ann Intern Med 1991; 115:360366. 37. Nowack R, Fliser D, Richter J, Horne C, Mutschler E, Ritz E. Effects of angiotensin converting enzyme inhibition on renal sodium handling after furosemide injection. Clin Investig 1993; 71:622627. 38. Loon NR, Wilcox CS, Unwin RJ. Mechanism of impaired natriuretic response to furosemide during prolonged therapy. Kidney Int 1989; 36:682-689. 39. Salvator DR, Rey NR, Ramos GC, Punzalan FE. Continuous infusion versus bolus injection of loop diuretics in congestive heart failure. Cochrane Database Syst Rev 2005; 3: CD003178. 40. Pivac N, Rumboldt Z, Sardelic S, et al. Diuretic effects of furosemide infusion versus bolus injection in congestive heart failure. Int J Clin Pharmacol Res 1998; 18:121–128. 41. Schuller D, Lynch JP, Fine D. Protocol-guided diuretic management: comparison of furosemide by continuous infusion and intermittent bolus. Crit Care Med 1997; 25:1969 -1975. 42. Licata G, Di Pasquale P, Parrinello G, et al. Effects of high-dose furosemide and small-volume hypertonic saline solution infusion in comparison with a high dose of furosemide as bolus in refractory congestive heart failure: long-term effects. Am Heart J 2003; 145:459–466. 43. Felker GM, Lee KL, Bull DA, et al; NHLBI Heart Failure Clinical Research Network. Diuretic strategies in patients with acute decompensated heart failure. N Engl J Med 2011; 364:797-805. 44. Sica DA, Gehr TW. Diuretic combinations in refractory oedema states: Pharmacokinetic-pharmacodynamic relationships. Clin Pharmacokinet 1996; 30:229-249. 45. Steinmuller ST, Puschett JB. Effects of metolazone in man: comparison with chlorothiazide. Kidney Int 1972; 1:169-181. 46. Ellison DH, Velázquez H, Wright FS. Adaptation of the distal convoluted tubule of the rat: structural and functional effects of dietary salt intake and chronic diuretic infusion. J Clin Invest 1989; 83:113-126. 47. Kobayashi S, Clemmons DR, Nogami H, Roy AK, Venkatachalam MA. Tubular hypertrophy due to work load induced by furosemide is associated with increases of IGF-1 and IGFBP-1. Kidney Int 1995; 47:818-828. 48. Ellison DH. The physiologic basis of diuretic synergism: its role in treating diuretic resistance. Ann Intern Med 1991; 114:886-894. 49. Inoue M, Okajima K, Itoh K, et al. Mechanism of furosemide resistance in analbuminemic rats and hypoalbuminemic patients. Kidney Int 1987; 32:198-203. 50. Rane A, Villeneuve JP, Stone WJ, Nies AS, Wilkinson GR, Branch RA. Plasma binding and disposition of furosemide in the nephrotic syndrome and in uremia. Clin Pharmacol Ther 1978; 24:199207. 51. Keller E, Hoppe-Seyler G, Schollmeyer P. Disposition and diuretic effect of furosemide in the nephrotic syndrome. Clin Pharmacol Ther 1982; 32:442-449. 52. Kramer HJ, Schuurman J, Wasserman C, et al: Prostaglandin-independent protection by furosemide from oliguric ischemic renal failure in conscious rats. Kidney Int 1980; 17:455-464. 608 Rational Use of Diuretics and Pathophysiology of Edema 53. Sirivella S, Gielchinsky I, Parsonnet V: Mannitol, furosemide, and dopamine infusion in postoperative renal failure complicating cardiac surgery. Ann Thorac Surg 2000; 69:501-506. 69. Messerli FH, Bangalore S, Julius S. Risk/benefit assessment of beta-blockers and diuretics precludes their use for first-line therapy in hypertension. Circulation 2008; 117:2706-2715. 54. Nicholson ML, Baker DM, Hopkinson BR, et al: Randomized controlled trial of the effect of mannitol on renal reperfusion injury during aortic aneurysm surgery. Br J Surg 1996; 83:1230-1233. 70. National Collaborating Centre for Chronic Conditions. Hypertension: management in adults in primary care: pharmacological update. London: Royal College of Physicians, 2006. 55. Allgren RL, Marbury TC, Rahman SN, et al: Anaritide in acute tubular necrosis. Auriculin Anaritide Acute Renal Failure Study Group. N Engl J Med 1997; 336:828-834. 71. Mancia G, De Backer G, Dominiczak A, et al. 2007 ESH-ESC practice guidelines for the management of arterial hypertension. J Hypertens 2007; 25:1751-1762. 56. Solomon R, Werner C, Mann D, et al: Effects of saline, mannitol, and furosemide to prevent acute decreases in renal function induced by radiocontrast agents. N Engl J Med 1994; 331:1416-1420. 72. Adams KF, Lindenfeld J, Arnold JMO, et al. Heart Failure Society of America. HFSA 2006 Comprehensive Heart Failure Guideline. J Card Fail 2006; 12: e1–e122. 57. Cotter G, Weissgarten J, Metzkor E, et al. Increased toxicity of high-dose furosemide versus low-dose dopamine in the treatment of refractory congestive heart failure. Clin Pharmacol Ther 1997; 62:187-193. 73. Faris R, Flather M, Purcell H, Henein M, Poole-Wilson P, Coats A. Current evidence supporting the role of diuretics in heart failure: a meta-analysis of randomised controlled trials. Int J Cardiol. 2002; 82: 149–158. 58. Lassnigg A, Donner E, Grubhofer G, et al. Lack of renoprotective effects of dopamine and furosemide during cardiac surgery. J Am Soc Nephrol 2000; 11:97-104. 74. Ellison DH. Diuretic therapy and resistance in congestive heart failure. Cardiology 2001; 96:132–143. 59. Shilliday IR, Quinn KJ, Allison ME. Loop diuretics in the management of acute renal failure: A prospective, double-blind, placebo-controlled, randomized study. Nephrol Dial Transplant 1997; 12:2592-2596. 60. Stevens MA, McCullough PA, Tobin KJ, et al. A prospective randomized trial of prevention measures in patients at high risk for contrast nephropathy: Results of the PRINCE Study Prevention of Radiocontrast Induced Nephropathy Clinical Evaluation. J Am Coll Cardiol 1999; 33:403-411. 61. Lewis J, Salem MM, Chertow GM, et al. Atrial natriuretic factor in oliguric acute renal failure. Anaritide Acute Renal Failure Study Group. Am J Kidney Dis 2000; 36:767-774. 62. Bellomo R, Chapman M, Finfer S, et al. Low-dose dopamine in patients with early renal dysfunction: A placebo-controlled randomised trial. Australian and New Zealand Intensive Care Society (ANZICS) Clinical Trials Group. Lancet 2000; 356:2139- 2143. 75. Shah SU, Anjum S, Littler WA. Use of diuretics in cardiovascular diseases: (1) heart failure Postgrad Med J 2004; 80: 201–205. 76. Perez-Ayuso RM, Arroyo V, Planas R, et al. Randomized comparative study of efficacy of furosemide versus spironolactone in nonazotemic cirrhosis with ascites: relationship between the diuretic response and the activity of the renin-aldosterone system. Gastroenterology 1983; 84:961–968. 77. Domanski M, Norman J, Pitt B, Haigney M, Hanlon S, Peyster E. Studies of Left Ventricular Dysfunction. Diuretic use, progressive heart failure, and death in patients in the Studies of Left Ventricular Dysfunction (SOLVD). J Am Coll Cardiol 2003; 42:705–708. 78. de Gasparo, Joss U, Ramjoue HP, Whitebread SE, Haenni H, Schenkel L, Kraehenbuehl C, Biollaz M, Grob J, Schmidlin J. Three new epoxyspirolactone derivatives: characterization in vivo and in vitro. J Pharmacol Exp Ther 1987; 240:650–656. 63. Mehta RL, Pascual MT, Soroko S, et al. Diuretics, mortality, and nonrecovery of renal function in acute renal failure. JAMA 2002; 288:2547-2553. 79. Pitt B, Remme W, Zannad F, et al. Eplerenone Post-Acute Myocardial Infarction Heart Failure Efficacy and Survival Study Investigators. Eplerenone: a selective aldosterone blocker, in patients with left ventricular dysfunction after myocardial infarction. N Engl J Med 2003; 348: 1309–1321. 64. Uchino S, Doig GS, Bellomo R, et al. Beginning and Ending Supportive Therapy for the Kidney (BEST Kidney) Investigators. Diuretics and mortality in acute renal failure. Crit Care Med 2004; 32:1669-1677. 80. Pinzani M, Daskalopoulos G, Laffi G, Gentilini P, Zipser RD. Altered furosemide pharmacokinetics in chronic alcoholic liver disease with ascites contributes to diuretic resistance. Gastroenterology 1987; 92: 294–298. 65. Chobanian AV, Bakris GL, Black HR, et al. The Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure: the JNC 7 report. JAMA 2003; 289:2560-2572. 81. Gatta A, Angeli P, Caregaro L, et al. A pathophysiological interpretation of unresponsiveness to spironolactone in a stepped-care approach to the diuretic treatment of ascites in non-azotemic cirrhotic patients. Hepatology 1991; 14:231–236. 66. Psaty BM, Lumley T, Furberg CD, et al. Health outcomes associated with various antihypertensive therapies used as first-line agents: a network meta-analysis. JAMA 2003; 289:2534-2544. 82. Carter BL, Einhorn PT, Brands M, et al; Working Group from the National Heart, Lung, and Blood Institute. Thiazide-induced dysglycemia: call for research from a working group from the national heart, lung, and blood institute. Hypertension 2008; 52:30-36. 67. Law MR, Morris JK, Wald NJ. Use of blood pressure lowering drugs in the prevention of cardiovascular disease: meta-analysis of 147 randomised trials in the context of expectations from prospective epidemiological studies. BMJ 2009; 338:b1665-b1665. 68. Wright JM, Musini VM. First-line drugs for hypertension. Cochrane Database Syst Rev 2009; 3:CD001841-CD001841. 83. Takaya A, Fukui H, Matsumura M, et al. Stepped care medical treatment for cirrhotic ascites: analysis of factors influencing the response to treatment. J Gastroenterol Hepatol 1995; 10:30–35. 84. Wilcox CS, Mitch WE, Kelly RA, et al. Response of the kidney to 609 Medicine Update 2012 Vol. 22 furosemide. I. Effects of salt intake and renal compensation. J Lab Clin Med 1983; 102:450-458. 85. Voelker Jr, Cartwright-Brown D, Anderson S, et al. Comparison of loop diuretics in patients with chronic renal insufficiency. Kidney Int 1987; 32:572-578. 86. Ouzan J, Perault C, Lincoff AM, Carre E, Mertes M. The role of spironolactone in the treatment of patients with refractory hypertension. Am J Hypertens 2002; 15: 333-339. 87. Gottlieb SS, Brater DC, Thomas I, et al. BG9719 (CVT-124), an A(1) adenosine receptor antagonist, protects against the decline in renal function observed with diuretic therapy. Circulation 2002; 105:1348 –1353. 88. Francis GS, Siegel RM, Goldsmith SR, Olivari MT, Levine TB, Cohn JN. Acute vasoconstrictor response to intravenous furosemide in patients with chronic congestive heart-failure - activation of the neurohumoral axis. Ann Intern Med 1985; 103:1– 6. 89. Wright JT Jr, Probstfield JL, Cushman WC, et al. ALLHAT findings revisited in the context of subsequent analyses, other trials, and meta-analyses. Arch Intern Med 2009; 169:832-842. 90. Greenberg A. Diuretic complications. Am J Med Sci 2000; 319:1024. 610