Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
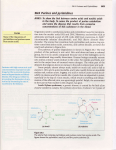
Gout and Hyperuricemia Gout is one of the oldest known and most common forms of arthritis; it is a crystal deposition disease in which crystals of monosodium urate form in joints and other tissues. Gout attacks cause a characteristic painful inflammation of one or more joints of the extremities, or nodules in soft tissues called tophi. An acute attack of gout, although brief and usually subsiding spontaneously, can be temporarily debilitating, and predisposes an individual to subsequent attacks. Once a disease of only the affluent (who could afford the purine-rich foods and drink linked to gout risk), this "disease of kings" has rapidly become a disease of everyman. The prevalence of gout among US adults, according to the National Health and Nutrition Examination Survey (2007-2008) is estimated at 3.9% (8.3 million people), favoring men over women by almost 3:1 (Zhu 2011). This represents a significant 44% increase in gout frequency from previous estimates just a decade earlier (Kramer 2002.) The primary risk factor for gout is elevated levels of a metabolic byproduct called uric acid in the blood; this condition is known as hyperuricemia. Hyperuricemia is estimated to affect over 21% of the US population, and doubles in frequency between ages 20 and 80 years (Zhu 2011.) Hyperuricemia increases the risk of not only gout, but other diseases as well, including hypertension, kidney disease, and metabolic syndrome. Even during the asymptomatic periods between gout attacks, the body is exposed to periods of low-grade, chronic inflammation. The propensity for excessive blood uric acid and gout is also increased by other disease states; therefore, a gout or hyperuricemic patient should consider Life Extension's recommendations and protocols for Inflammation, Cardiovascular Disease, Hypertension, Kidney Health, and Obesity as well. Uric Acid Metabolism Uric acid is the final product of purine metabolism in humans. Purines are components of nucleosides, the building blocks of DNA and RNA. Purine nucleosides (adenosine and guanine) are used in the creation of other metabolically important factors as well, such as adensosine triphosphate (ATP; the energy-carrying molecule), S-adeneosylmethione (SAMe; the methyl donor), and nicotine adenine dinucleotide (NADH; an important cofactor in energy production and antioxidation). Given the importance of purine-containing molecules for survival, vertebrates, including humans, have developed robust systems for synthesizing sufficient purine nucleosides for their metabolism using readily available materials (such as glucose, glycine, and glutamine), as well as recycling purine nucleosides from throughout the body or from the diet. In mammals, excess purine nucleosides are removed from the body by breakdown in the liver and excretion from the kidneys. For most mammals, the purines are first converted into the intermediate uric acid, which is then metabolized by the enzyme uricase into the compound allantoin. Allantoin is a very soluble compound that can easily travel through the bloodstream, become filtered by the kidneys, and be excreted from the body. In contrast to other mammals, humans and other primates lack a functional uricase enzyme, and can only break purines down into uric acid. The levels of uric acid in the blood depend on two factors. The first is the rate of uric acid synthesis in the liver. Since uric acid results from purine degradation, its levels are influenced by both the amount of purines synthesized in the body, as well as the amounts of purines absorbed from the diet (Richette 2010). The second determinant of blood uric acid levels is the rate of uric acid excretion from the kidneys. Excretion has the greatest effect on blood uric acid levels, with about 90% of hyperuricemia cases attributed to impaired renal excretion (Choi 2005). Impaired excretion is most often due to abnormalities in the kidney urate transporter (called URAT1) or organic ion transporter (OAT), both of which control the movement of uric acid out of proximal kidney tubules and into urine (Enomoto 2002.) One of the most intriguing aspects of uric acid is that although it appears to be a "waste product" of purine metabolism, only about 10% of the uric acid that enters a normal human kidney is excreted from the body (Richette 2010). In other words, rather than eliminating uric acid, a healthy kidney returns up to 90% of it to the blood stream. The reason for this is likely due to the role or uric acid as one of the most important antioxidants in body fluids, responsible for the neutralization of over 50% of the free radicals in the blood stream (Glantzounis 2005.) The ability of humans and primates to preserve blood levels of uric acid (due to slow kidney filtration and lack of a uricase enzyme) was probably advantageous to our evolution, by increasing antioxidant capacity of the blood (Alvarez-Lario and Macarrón-Vicente 2011.) Humans and primates are one of the few mammals that cannot produce their own vitamin C, and may have evolved the ability to preserve uric acid to compensate for this (Hediger 2002). For example, blood uric acid levels in humans are normally about 6 times that of vitamin C, and about ten times the levels in other mammals (Roch-Ramel 1999). Like vitamin C, uric acid has a principle role in protecting high-oxygen tissues (like the brain) from damage, and low blood uric acid levels have been associated with the progression or increased risk of several neurological disorders, including Amyotrophic Lateral Sclerosis (Keizmann 2009), Multiple sclerosis (Rentzos 2006), and Huntington's (Auinger 2010), Parkinson's (Andreadou 2009), and Alzheimer's diseases (Kim 2006.) Hyperuricemia and the Development of Gout Uric acid is a metabolic "waste product" with poor solubility in body fluids, yet its potential role as a primary antioxidant in body fluids suggests that it should be kept at sufficient levels in the blood. Clearly, these diametric properties of uric acid define a range for normal blood uric acid levels. Commonly, the upper limit of this range is taken as 8.6 mg/dl in men and 7.1 mg/dl in women, (although some laboratories and research groups use different limits) (Zhang 2006a; Sclesinger 2009; Sun 2010). Uric acid levels above this limit are considered as hyperuricemia. Hyperuricemia is a primary risk factor for the development of gout, although it is likely that many hyperuricemic individuals will not develop symptoms. (Alvarez-Lario and Macarrón-Vicente 2011). While the risk of a gout attack increases with blood uric acid, the annual occurrence of inflammatory gout is fairly low; persons with blood uric acid levels between 7 and 8.9 mg/dL have a 0.5-3% change of developing the disease, which rises to 4.5% at levels over 9 mg/dL (Campion 1987.) Hyperuricemia without symptoms (asymptomatic hyperuricemia) is also a risk factor for other diseases (see below). Although patients with asymptomatic hyperuricemic may never experience the symptoms of a gout attack, ultrasound studies have revealed that up to one-third may have urate deposits and evidence of inflammation in their joints and surrounding soft tissues (Puig 2008.) As local serum uric acid concentrations rise above their limit of solubility, monosodium urate can begin to precipitate out of the blood, forming needle-like crystals preferentially in cartilage and fibrous tissues. Here, the crystals may reside for years without causing problems (Doherty 2009). Urate crystals within tissues have two fates; they can re-dissolve in body fluids and reenter circulation, or may be "shed" from the tissue. Shed monosodium urate crystals can enter nearby joint spaces or bursa (the fluid-filled sacs that provide cushioning between tendons and bones around a joint), where they are quickly engulfed by immune cells. This activates a localized inflammatory response, leading to the characteristic arthritis of gout (Martinon 2006.) Gout is commonly divided into distinct "phases" of recurrent attacks of acute gout interspersed with symptom free periods, with cumulative crystal deposition gradually contributing to a chronic condition (chronic tophaceous gout.) An attack of acute gout usually appears as a sudden inflammatory arthritis of a single joint in the lower extremities, most often the metatarsophalangeal joint of the big toe (the "ball" of the foot). At this joint, gout is called podagra. Other joints that are frequently affected include the mid-foot, ankle, knee, wrists and finger joints. The skin may be red and shiny above the affected area. Attacks often begin in the early morning reach a peak within 6 to 24 hours. The pain is severe, and patients often cannot wear socks or touch bedsheets during flare-ups (Eggebeen 2007). Even without treatment, the attacks typically subside spontaneously within several days to two weeks. Acute gout attacks can also be accompanied by high fever and leukocytosis (elevated white blood cell count) (Doherty 2009.) Gout attacks can be triggered by a variety of factors, many of which reduce the solubility of urate in the blood; these include infection, trauma to the joint, rapid weight loss, dehydration, acidosis, and lower body temperature (which explains the timing of gout attacks and why they most frequently occur in the extremities) (Eggebeen 2007.) Following resolution of an acute attack, a patient can enter an "intercritical period", or a period without symptoms. Although the patient may be asymptomatic, monosodium urate crystals and low-grade inflammation can persist in the joint during this period (Pascual 1991). Once an initial acute gout attack has occurred, further attacks are likely to follow. Recurrent attacks of acute gout often lead to chronic tophaceous gout, in which monosodium urate deposits (tophi) form in the soft tissues, usually along the rim of the ear, over the elbow joint, and in the joints of the fingers and toes. Tophi reduce the growth and viability of bone cells (osteoblasts) (Chhana 2011) and if left untreated, tophaceous gout can lead to significant joint erosion and loss of function (Eggebeen 2007.) The Role of Hyperuricemia in Other Conditions Although hyperuricemia is most often associated with gout, elevated blood levels of uric acid have also been associated with other diseases. Hyperuricemia and gout are both risk factors for kidney or bladder stones (urolithiasis). Both conditions increase the risk of forming not only uric acid stones, but also the more common calcium oxalate stones. The presence of calcium oxalate stones is 10-30 times higher in gout patients than those without gout (Pak 2005). Deposits of monosodium urate crystals in kidney tissues can result in kidney damage (nephropathy), either acutely by formation of crystals within the tubules of the kidney, or through a chronic inflammatory response to urate deposits in other tissues of the kidney (Johnson 1999). Prior to the development of uric acid lowering treatments, kidney disease occurred in up to 40% of gout patients; renal failure was the usual cause of death in 18-25% of these patients (Alvarez-Lario 2011.) Hyperuricemia is a risk factor for cardiovascular diseases in high risk groups, and has been associated with small increases in the risk of coronary events (Kim 2009), heart failure (Ekundayo 2010), and stroke (Kim 2010). It is often seen in patients with hypertension; high blood pressure has long been thought to contribute to elevated blood uric acid, possibly due to reduced blood flow to the kidneys and lower urate excretion (Mazzali 2010). However, recent experimental and epidemiological data suggest that the opposite may be true: a comprehensive review of 18 observational studies revealed that for each 1 mg/dl increase in blood uric acid, in risk of hypertension increased by 13% (Grayson 2011). This effect was more pronounced in women and young adults. Lowering of uric acid levels in hyperuricemic, hypertensive adolescents reduced their blood pressure as well (Feig 2008). Ironically, the increased risk of cardiovascular diseases associated with hyperuricemia may be due to increases in oxidative stress: xanthine oxidase, the enzyme that synthesizes uric acid, also produces free radicals in the process (Glantzounis 2005.) Hyperuricemia is an integral part of metabolic syndrome (Doherty 2009), and epidemiological studies have demonstrated that elevated uric acid levels substantially increase metabolic syndrome risk (and vice versa) (Dao 2010 ; Choi 2007a). Data from the Multiple Risk Factor Intervention Trial (MRFIT) showed that hyperuricemia was associated with increased risk of type 2 diabetes, and that male patients with gout had a 41% increased risk for the disease (Choi 2008.) Risk Factors for Gout Hyperuricemia is the primary risk factor for gout, and is required, although not sufficient, for the progression of the disease. The risk of gout increases with age and is more common in men; increased risk is also associated with other medical conditions including hypertension, obesity, renal insufficiency, early menopause (hormone therapy can reduce this risk), hypercholesterolemia, and surgery. Some medications increase gout risk (which is reversible upon discontinuation), particularly loop and thiazide diuretics, but also antituberculous drugs, cyclosporin, and levodopa (Bierer 1982; Scott 1991; Doherty 2009; Singh .)1122Aspirin has a dual effect on uric acid levels; low doses inhibit excretion and increase blood levels, while very high doses (>3000mg/day) reduce levels (Doherty 2009). At 75 mg/day in elderly patients, the increase in blood uric acid is about 6% (Caspi 2000.) Uric acid levels are very sensitive to dietary influences. High-purine foods, particularly red meat, fish, and shellfish, have long been known to increase hyperuricemia and gout risk. Data from the Health Professionals Follow-up Study, which followed over 47,000 health professionals for 12 years, revealed that individuals with the highest intakes of beef, pork, or lamb (>1.9 servings/day) and seafood (>0.6 servings/day) increased their risk of gout by 77% and 53%, respectively (Choi 2004a). There were no associations between total protein intake, total animal protein (including dairy protein, poultry, and eggs) intake, or purine-rich vegetable intake and the incidence of gout. Alcoholic beverages increase blood uric acid and gout risk (Choi 2004b; Choi 2004). In one study, individuals who consumed one beer or one serving of spirits per day had 1.75 and 1.22 times the incidence of gout, respectively, than individuals who consumed less than one drink a month. Drinking over 2 beers/day increased gout risk by 2.5-fold (Choi 2004b). Wine does not appear to affect gout risk. Alcohol metabolism to acetate accelerates the breakdown of purine-containing nucleotides (like ATP) and raises blood uric acid (Puig 1984). Alcohol can also lower body temperature in the extremities which may precipitate an acute attack independent of blood uric acid concentration (gout attacks can occur in alcoholics at lower blood urate levels than in nonalcoholics) (Vandenburg 1994). Beer, despite having less alcohol per serving than the other beverages, is more hyperuricemic due to its high purine content (Gibson 1984.) Fructose has been positively associated with both gout and hyperuricemia risk in some studies, but has had no significant effect in others. In the third National Health and Nutritional Examination Survey of 14,761 individuals over 20 years old, (NHANES III), individuals who consumed one or more sweetened soft drinks per day had levels of blood uric acid that averaged 0.5 mg/dl higher than nondrinkers (Choi 2008b). By comparison, persons who consumed an equivalent amount of orange juice had blood uric acid levels that averaged only about 0.15mg/dl higher than non-juice drinkers. An analysis of more recent NHANES data (Sun 2010), however, failed to find any significant association between total fructose consumption and hyperuricemia risk. These results, in addition to the conflicting results of several metabolic studies of fructose in human volunteers, suggest that the relationship between fructose and hyperuricemia may be sensitive to factors aside from just the amount of ingested sugar (Sun 2010.) Conventional Gout Diagnosis and Treatment Gout usually presents with characteristic inflamed, painful joints in the extremities, but these symptoms are also common to other conditions, particularly pseudogout (a related condition caused by the accumulation of calcium pyrophosphate crystals in the joint) or septic arthritis (caused by joint infection). Blood tests can determine whether the patient is hyperuricemic (typically a serum concentration above 7 mg/dL in males and above 6 mg/dL in females). While hyperuricemia is the most important risk factor for gout its diagnostic power may be limited; as some hyperuricemic patients may never develop the disease, and blood urate levels may be normal during an acute attack (in one study, 14% of patients had blood uric acid levels of <6 mg/dl during their gout attacks) (Schlesinger 2009.) The European League Against Rheumatism (EULAR) recently published guidelines for gout diagnostic criteria, based on accumulated studies of gout diagnoses. According to their analysis, the most definitive feature in the diagnosis of gout is the identification of monosodium urate crystals in synovial (joint) fluid or aspirates of tophi (Zhang 2006a). This involves the insertion of a fine needle into the joint or tophus and withdrawing a fluid sample, which is subsequently examined under a microscope (Kasper 2005). The presence of large needle-shaped crystals confirms the presence of monosodium urate, and can be used to differentiate gout from pseudogout or septic arthritis. The presence of urate crystals in the joints of asymptomatic patients can be used to identify intercritical periods in patients with recurrent gout, or can be used to screen patients who may benefit from urate-lowering therapy prior to their first acute gout attack. Screening of the joints of the extremities using ultrasound is being explored as a non-invasive method to improve the detection of urate crystals in asymptomatic patients. In a pilot study, ultrasound correctly identified urate crystals in the joints of asymptomatic, hyperuricemic volunteers with an accuracy of 81% (De Miguel 2011.) Treatments for acute gout attacks typically manage pain and inflammation, and include NSAIDS, corticosteroids, and colchicine. While treatments for acute gout are typically short term, there are risks of significant gastrointestinal side effects for NSAIDs and colchicine in some individuals. Moreover, though colchicine is FDA approved to treat acute gout flares, it has a low therapeutic index, meaning that the dose required to exert a beneficial effect is near that which is potentially toxic. Aspiration of affected joints to relieve pressure, and injection of long-acting steroids are commonly used treatments in practice, although they have not been investigated in controlled trials (Zhang 2006b.) After the initial attack has subsided, patients are usually encouraged to adopt lifestyle changes that may reduce hyperuricemia and gout risk (such as lower purine diets, weight loss, or exercise). Many will be placed on longer-term uric acid-reduction therapy. Recall that uric acid levels are controlled by the rate of uric acid production and the rate of uric acid excretion; current therapies address either of these two aspects. Xanthine oxidase inhibitors reduce the activity of xanthine oxidase, the final step in uric acid synthesis. This has the effect of lowering uric acid production. Allopurinol (Zyloprim) has a long history of usage as a xanthine oxidase inhibitor; recently febuxostat (Uloric) has been approved for treatment of hyperuricemia in the US. Febuxostat exhibits greater uric acid-lowering effects than allopurinol, although the incidence of gout flares is similar between the two drugs (Becker 2005.) Uricosuric drugs increase the excretion of uric acid from the kidneys, primarily by reducing the absorption of uric acid from the kidneys back into the blood. Probenecid (Benemid) and sulfinpyrazone (Anturane) are two examples. These drugs tend to increase urinary uric acid levels, which can cause kidney stones. The tophi of chronic gout, if severe enough to cause joint dysfunction or deformity, can also be treated by surgical removal (Larmon 1970; Ford 1992.) Innovative New Drugs for the Management of Chronic Gout As mentioned earlier in this protocol, in most mammals uric acid is converted into the more soluble compound allantoin by an enzyme called uricase. This conversion allows for the urinary excretion of allantoin, thereby reducing uric acid blood levels. However, humans are unable to facilitate this conversion due to an evolutionary loss of the uricase enzyme. Recently, scientists have recreated the mammalian uricase enzyme in the laboratory and generated injectable medications that deliver the recombinant enzyme it into the blood. Once in the blood stream, the recombinant uricase enzyme breaks down uric acid into allantoin, which is then easily excreted through the human kidneys. By injecting this enzyme otherwise not present in higher primates, the rate of uric acid excretion can be expedited. Two such medications are available – rasburicase (Elitek®), and a chemically modified version of this same drug, called pegloticase (Krystexxa®). Pegloticase is FDA approved to lower uric acid levels in patients with chronic gout (FDA 2010.) In two concurrent randomized, double-blind, placebo-controlled trials, pegloticase, administered at a dose of 8 mg either every two weeks or every four weeks, efficiently lowered uric acid levels (Sundy 2011). The participants in these studies consisted of patients with chronic gout, which had not been relieved by allopurinol, and blood uric acid levels above 8.0 mg/dl at baseline. Reduction of uric acid levels to <= 6.0 mg/dl was the primary endpoint, and was achieved in 38% of patients receiving biweekly injections, and in 49% of those receiving monthly injections. However, pegloticase may cause some side effects. In the studies mentioned above, between a quarter and a half of subjects experienced an injection site reaction, of which 6.5% were considered to be anaphylaxis. This means that physicians may opt to administer corticosteroids before pegloticase in order to suppress the immune system in hopes of avoiding an inflammatory response. The long-term effects of corticosteroids in combination with pegloticase have not been studied as of yet, so the side effects in gout patients remain unknown (Ea 2011.) Many physicians may not be aware of the availability of pegloticase for lowering uric acid levels in gout patients due to its recent FDA approval. Individuals with chronic gout that has not improved after the use of conventional gout medications should consider asking their healthcare professional if pegloticase is right for them.