Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
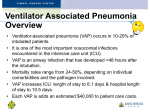
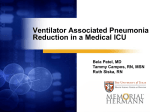
RAJIV GANDHI UNIVERSITY OF HEALTH SCIENCES BANGALORE, KARNATAKA ANNEXURE – 2 PROFORMA FOR REGISTRATION OF SUBJECTS FOR DISSERTATION 1. NAME OF CANDIDATE AND ANGELINE KURIAN ADDRESS 1ST YEAR M. SC NURSING ST. JOHN’S COLLEGE OF NURSING BANGALORE-34 2. NAME OF THE INSTITUTION ST.JOHN’S COLLEGE OF NURSING 3. COURSE OF SYUDY SUBJECT M.SC NURSING CHILD HEALTH NURSING 4. DATE OF ADMISSION TO COURSE MAY 2ND, 2012 5. Title of the Topic IMPACT OF ADHERENCE TO A VENTILATOR ASSOCIATED PNEUMONIA (VAP) BUNDLE ON THE INCIDENCE OF VAP IN PICU. 6. Brief resume of the intended work 6.1 Need for the study Intensive care units have come to represent the most frequently identifiable source of nosocomial infection within hospital, with the infection rates and rate of antimicrobial resistance several fold greater than General hospital settings. Ventilator associated pneumonia (VAP) is defined as nosocomial pneumonia in ventilated patients that develop more than 48 hours after initiation of mechanical ventilation(MV). VAP is the second most common nosocomial infection after urinary tract infection in pediatric intensive care unit patients accounting for 20% of nosocomial infection in this population. VAP can be of two types. Early onset VAP which develops within 5 days of mechanical ventilation and late onset VAP which develops 5 days or more after mechanical ventilation.1 The number of VAP cases per 1000 ventilator days, is the standard measure for surveillance by the CDC and are outlined in CDC guidelines. The incidence of VAP in PICU is 18.7 per 1000 days of mechanical ventilation. Ventilator associated pneumonia occurs in 9 to 27% of all intubated patients and 28 to 40% of brain injury in ventilated patients develops due to this condition.Ventilator Associated - Pneumonia occurs up to 17 times more frequently in developing countries than elsewhere and has a mortality rate as high as 27%, among all other infections. The risk of VAP is higher during early course of hospital stay. It is estimated to be 3% during first 5 days, decreasing to 2% during 5 to 10 days of mechanical ventilation and to 1% afterwards. Among hospital acquired infections VAP is the leading cause of death, exceeding the rate of death due to central line infections, severe sepsis, and respiratory infections in the non-intubated patients. Hospital mortality of ventilated patients who develop VAP is 46%, in comparison with 32% of ventilated patients who do not develop VAP. Patients with VAP have longer stays in the ICU and in the hospital than the uninfected patients, even after adjusting for the underlying severity of their illness.2 VAP has been associated with increased length of ventilator dependence, increased PICU and hospital stay, increased mortality, and increased hospital costs. Patients who developed VAP had a significantly higher overall mortality rate, increased PICU mortality rate and 56 and 43% increase in the length of PICU and hospital stay respectively.3 The primary route of VAP pathogenesis is a combination of two processes; bacterial colonization of the aero-digestive tract and the subsequent aspiration in to the lower airway. Early onset pneumonia is usually caused by Staphylococcus aureus, Haemophilus influenza and Streptococcus pneumonia, and late onset pneumonia is caused by Methicillin Resistant Staphylococcus Aureus, Pseudomonas aeruginosa, and Acinetobacter or enterobacter. Traditional signs and symptoms of VAP are chest X-ray showing new or progressive diffuse infiltrate which is not attributable to any other causes, onset of purulent sputum, fever greater than 38.5 0 C, leukocytosis, and positive sputum or blood cultures. The single largest risk factor for VAP is the presence of endotracheal tube. Patient related risk factors include underlying chronic illness, immunosuppression, depressed consciousness, thoracic or abdominal surgery, previous antibiotic therapy and previous infection. Devise, treatment and personnel related risk factors include nasogastric tube placement, bolus enteral feeding, gastric over distension, stress ulcer treatment, supine patient position, nasal intubation route, instillation of normal saline, understaffing, non-conformance to hand washing protocol, indiscriminate use of antibiotics and lack of training in VAP prevention. 4 Risk factors for development of VAP can be classified in to modifiable and non modifiable conditions. Risk factors can be patient related or treatment related. Modifiable risk factors are obvious targets for improved management and prophylaxis in the comprehensive Guidelines for preventing Health care associated pneumonia, published by centre for disease control. Effective strategies include strict infection control, alcohol based hand disinfection, monitoring and early removal of invasive devices and programs to reduce or alter antibiotic prescribing practices.6 Interventions to prevent VAP begin at the time of intubation and should be continued until extubation. Nurses need to understand the pathophysiology of VAP, risk factors and strategies that may prevent VAP. Use of study education modules on nursing care of patients at risk of VAP and use of ventilator pathways or protocols with pre-printed order sets and monitoring tools can lead to improved outcome for patients.5 A pre test post test study was conducted to assess effectiveness of a multidimensional approach to reduce ventilator associated pneumonia in a paediatric intensive care units, of 5 developing countries (Colombia, Salvador, India, Philippines and Turkey). During study period VAP rate was 11.7 per 1000 ventilator days and 8.1 per 1000 ventilator days during intervention period, demonstrating 31% reduction in VAP rates.5 A cross sectional observational study was conducted to determine frequency of ventilator associated pneumonia and to identify the associated factors, causative organisms and outcome of VAP in children admitted to ICU of Children’s hospital and Institute of Child Health, Lahore, for 15 months. Out of 93 patients receiving ventilator support during study period 16 developed VAP (17%). Factors significantly associated with were age less than one year, unplanned emergency intubation and use of continuous intravenous sedation. Overall mortality was 23% among ventilated cohort. Average length of stay in ICU among all ventilated cases were 8.77 days and for the children who developed VAP mean duration of stay was 13.7 days compared to 7.7 days of those who did not develop VAP.14 St. John’s Medical College Hospital (SJMCH) is a tertiary care centre with bed strength of 1200. Average of 80 to 90 children is admitted per month .Out of which 25 to 30 patients need ventilator support. Incidence of VAP in PICU is 16%, which means out of 25 ventilated patients 4 develop VAP. VAP can develop easily in ventilated children, leading to increased hospital stay, high cost and higher mortality rate. At the same time VAP can be prevented with implementation of a practice guideline with principles of prevention of iatrogenic spread of infection (hand hygiene, universal precaution and isolation technique), prevention of aspiration (head end elevation 30-45 degree and monitoring gastric residual volume ), oral hygiene(chlorhexidine oral care 6 hourly), avoiding contamination of respiratory equipment (change ventilator circuit when contaminated, empty respiratory circuit condensate 6 hourly and disinfect nebulizer unit between each use and using proper suction technique(do suction only when indicated, thorough suctioning of oropharynx, following asceptic technique for open tracheal suctioning, avoid instillation of normal saline or sterile water during tracheal suctioning, use clean glove during closed suctioning and changing inline suction catheter according to manufacturer’s recommendations or when it is soiled). Therefore researcher felt a strong need to assess the practice regarding prevention of VAP in PICU setting. This is planned in order to implement a ventilator associated pneumonia bundle , which will provide staff nurses with a base of scientific knowledge and thereby to reduce the VAP incidences in PIU 6.2 Review of Literature Review of literature provides base for future investigations, gives an insight in to the problem, intensifies need for data collection and relates finding of study to another which would facilitate to establish a comprehensive body of scientific knowledge. Literature is grouped under 3 headings : 1. Studies related to ventilator associated pneumonia. 2. Studies related to effectiveness of guidelines to prevent ventilator associated pneumonia. 3. Studies related to health care providers knowledge on ventilator associated pneumonia. 1. Studies related to ventilator associated pneumonia A prospective study was performed to detect the various etiological factors of VAP and the prevalence of multidrug resistant pathogens (MDR), over a period of 15 months, in Jawaharlal Institute of Postgraduate Medical Education and Research in Pondicherry, India. Enterobacteriaceae, Hemophilus influenza, Staphylococcus aureus Streptococcus pnumoniae, Candida were more common in early onset VAP, while fermenters were significantly associated with late onset VAP (p value 0.0267, chi-square value 4.9). This study found that VAP is increasingly associated with MDR pathogens and appropriate broad spectrum antibiotics should be used to treat them.8 A prospective observational study was conducted in NICU of CSM Medical University, Lucknow (UP) India to assess aetiology and risk factors of VAP in neonates over a period of one year. Neonates admitted to NICU who required mechanical ventilation for more than 48 hours were enrolled in to the study. The study group comprised of 98 neonates out of which, 30 neonates developed VAP (30.6%). VAP rates were 37.2 per 1000 days of mechanical ventilation. Most common bacterial organisms isolated from endotracheal aspirate of VAP patients were Klebsiella spp(32.8%) , E coli (23.2%), and Acinobacter (17.8%). Very low birth weight, prematurity, duration of mechanical ventilation, number of reintubations, and length of ICU stay were significantly associated with VAP in bivariate analysis. Multiple regression analysis revealed that duration of mechanical ventilation (OR 1.10, 95% CI 1.02, 1.21; p=0.021) and very low birth weight (OR 3.88, 95% CI 1.05, 14.34; p= 0.042) were two statistically significant risk factors in predicting VAP.1 A prospective observational study was conducted for one year in the PICU of Postgraduate Institute of Medical Education and Research, Chandigarh, India, to determine the incidence, aetiology and risk factors for nosocomial pneumonia (NP). Patients who needed ventilator support, were included and diagnosis of nosocomial pneumonia was made with regard to CDC guideline. Out of total sample 30.5% developed nosocomial pneumonia. Re intubation prolonged duration of ventilation. Mechanical ventilation was the significant risk factor for development of NP. On multiple regression analysis re-intubation was the single risk factor for NP. Overall mortality rate was 21%, and 7% of these deaths were due to Nosocomial Pneumonia.12 2. Studies related to effectiveness of ventilator associated pneumonia bundle A double blind randomized placebo controlled trial was conducted in Pediatric intensive care unit of All India Institute of Medical Sciences, New Delhi, to study the efficacy of oral mucosal decontamination with chlorhexidine gel for the prevention of ventilator associated pneumonia in children between 3 months and 15 yrs. Either 1% chlorhexidine or placebo gel was applied on the buccal mucosa at 8-hr intervals for the entire duration of ventilation, subject to a maximum of 21 days. Patients were followed up for the development of ventilator-associated pneumonia, diagnosed using the Centers for Disease Control and Prevention criteria. 41 children received 1% chlorhexidine, whereas 45 received placebo application. Incidence of ventilator-associated pneumonia was 39.6/1,000 ventilator days with 1% chlorhexidine and 38.1/1,000 ventilator days with placebo (relative risk 1.03, confidence interval 0.44-2.42, p = .46). The duration of intensive care unit stay and hospital stay was a mean of 8.4 ± 5.8 vs. 9.6 ± 11.days (p = .58) and 16.1 ± 10.2 days vs. 15.1 ± 14.3 days (p = .19) with chlorhexidine and placebo, respectively. The mortality rates were similar in the two groups (p = .81). All but two isolates causing ventilator-associated pneumonia were gram-negative, with Acinetobacter species being the most common (14 of 26). No side effects of the applied gel were seen in either group.7 A survey was conducted on current practices of intensivists practicing in Indian subcontinent to assess how VAP is managed. Three hundred, 10 point questionnaires were distributed and majority (96.8%) reported using VAP bundles with head of bed elevation (98.4%), Chlorhexidine mouth care (83.3%), stress ulcer prophylaxis (96.8%), heat and moisture exchangers (92.9%), early weaning(94.4%) and hand washing (97.6%) as part of their bundle. Majority reported, that they are using (39.7%) proton pump inhibitors for stress ulcer prophylaxis. 84.1% believed that VAP contributed to increased mortality.9 Another before and after structured study was conducted in an 18 bedded mixed medical surgical ICU of a hospital in Edinburg, United States of America to determine the effect of implementing VAP bundle of care. Main results showed that, compliance with head of bed elevation and chlorhexidine gel were 95-100%; compliance with wake and wean element was 70% and overall bundle compliance was 70%.Compared to pre intervention period, there was a significant reduction in VAP in post intervention period (32 cases per 1000 ventilator days to 12; p< 0.001). Statistical process control charts showed the decrease was more marked after VAP bundle implementation. Patient cohorts staying > 6 and >14 days had greater reduction in VAP acquisition and also had reduced antibiotic use (reduced by 1 and 3 days; p= 0.008/ 0.001).10 A pre- test post- test design study was conducted over a period of 05 months, in the University District Hospital in Atlanta, United States of America, to assess compliance to ventilator bundle strategies. Compliance was evaluated daily in random shifts after conducting lectures, bed pamphlets and card reminders. Pre educational compliance was 6%. Individual component compliance was head of bed elevation 14%, withdrawal of sedation 67%, peptic ulcer prophylaxis 93%, deep venous thrombosis prophylaxis 87%. Post educational compliance was 59% with individual compliance of 74%, 72%, 95%, and 92% respectively. A statistically significant increase in compliance was observed in ventilator bundle compliance and HOB elevation (p< 0.01).2 Another prospective study was conducted to assess impact of adherence to a ventilator associated pneumonia bundle on the incidence of VAP in surgical intensive care unit of Boston Medical Centre in Boston over a 38 month period. A daily checklist was considered compliant if all the items were performed for all patients. Prior to initiation of bundle VAP was seen at a rate of 10.2 cases per 1000 ventilator days. Compliance with bundle increased over the study period from 53% and 63% to 91% and 81% in each respective SICU. The rate of VAP decreased to 3.4 cases per 1000 ventilator days. 11 3. Studies related to health care providers knowledge on ventilator associated pneumonia A single group pre test post test study was conducted to assess nurse’s knowledge on evidence based guideline for prevention of ventilator associated pneumonia in critical care area, in a private tertiary care hospital in Karachi, Pakistan. Knowledge of nurses was assessed before, immediately after and after 4 weeks of intervention. The demographic data sheet was used to collect relevant information about participants. Knowledge scores of participants increased significantly, immediately after educational intervention.15 A descriptive study was conducted to detect knowledge of nurses working in ICU with respect to evidence based guideline for prevention of ventilator associated pneumonia in Johannesburg, South Africa. The nurses performed poorly in the test, with only 21.9% of participants obtaining a mark at or above competency level. 16 6.3 Statement of the problem A study to assess the impact of adherence to ventilator associated pneumonia (VAP) bundle on the incidence of ventilator associated pneumonia (VAP) in PICU of a selected hospital in Bangalore. 6.4 Objectives of the study 1. To assess the practice before and after implementation of ventilator associated pneumonia bundle. 2. To compare the incidence of ventilator associated pneumonia before and after implementation of VAP bundle. 3. To find association between incidence of ventilator associated pneumonia and patient’s baseline variables. 6.5 Operational definition 1. Impact Dictionary meaning of impact is a noticeable effect or influence. (Oxford dictionary 2011) In this study impact refers to extent to which adherence to VAP bundle in practice have occurred and decrease in the incidence of VAP after implementation of VAP bundle, assessed and scored by observation and record analysis. 2. Adherence Dictionary meaning of adherence is to stick firmly or follow. In this study meaning of adherence is following all aspects of ventilator associated pneumonia bundle assessed and scored by observation and record analysis. 3. Ventilator associated pneumonia (VAP) bundle. ventilator associated pneumonia (VAP) bundle is grouping of best practices supported by evidence strategies, with respect to ventilator associated pneumonia prevention (IHI 2011) In this study meaning of ventilator associated pneumonia (VAP) bundle is comprehensive recommendations for prevention of ventilator associated pneumonia which include prevention of iatrogenic spread of infection (hand hygiene, universal precaution), prevention of aspiration (head end elevation 30-45 degree and monitoring gastric residual volume), oral hygiene(chlorhexidine oral care 6 hourly), avoiding contamination of respiratory equipment (change ventilator circuit when contaminated, empty respiratory circuit condensate 6 hourly), using proper suction technique (do suction only when indicated, thorough suctioning of oropharynx, following asceptic technique for open tracheal suctioning, avoid instillation of normal saline or sterile water during tracheal suctioning and use clean glove during closed suctioning ) and peptic ulcer disease prophylaxis (administration of Sucralfate) 4. Incidences Dictionary meaning of incidence is rate or frequency of occurrence of something. In this study incidence meaning is number of VAP cases per 1000 ventilator days. Incidence of VAP =Patients with VAP/Patients on ventilator*1000. 5. Ventilator associated pneumonia Pneumonia in patients who have been on mechanical ventilation for greater than 48 hours (CDC guideline 2012) In this study ventilator associated pneumonia is a nosocomial lower respiratory tract infection occurring in mechanically ventilated patients 48 hours or more after initiation of ventilator support as diagnosed by physician. 6. Pediatric intensive care unit A special area in the hospital where critically ill pediatric patients who need close observation and frequent ministrations can be cared for by qualified, trained staff working under the best possible conditions. 7.Baseline variable In this study patient’s baseline variables are age, sex, diagnosis, number of days of mechanical ventilation and number of intubations. 6.6 Assumption 1. There will be some practice measures followed in PICU regarding ventilator associated pneumonia prevention. 2. VAP bundle may reduce the incidence of ventilator associated pneumonia in PICU.11 6.7 Delimitations This study is limited to, mechanically ventilated pediatric patients in PICU of St. John’s Medical College Hospital, Bangalore. 6.8 Projected outcome The result of the study will help to identify the effectiveness of VAP bundle in reducing ventilator associated pneumonia and this will provide guideline for nurses in preventing VAP in PICU. 6.9 Hypothesis H1. There will be a significant difference in the mean practice score before and after implementation of VAP prevention guideline at 0.05 level of significance. H2. There will be significant association between incidence of VAP and baseline variables of patients (age, sex, diagnosis, number of days on mechanical ventilation and number of intubations) 7. Material and method 7.1 Source of data Interventions carried out for mechanically ventilated pediatric patients. 7.1.1 Research design Research design selected for this study is quasi experimental design, in order to assess practice before and after implementation of ventilator associated pneumonia bundle. 7.1.2 Study setting This study is planned to conduct in St. John’s Medical College hospital, Bangalore. It is 1200 bedded, tertiary care hospital, with pediatric services. The study setting is Pediatric Intensive Care Unit. The PICU consists of 12 beds and there are 18 staff nurses and 7 doctors. On an average there are 25 to 30 patients who require ventilator support per month. 7.1.3 Population Population in this study comprise of all patients who are on ventilator support at the time of study, in SJMCH, Bangalore. 7.2 Method of data collection 7.2.1 Sampling procedure Sampling procedure refers to process of selecting a portion of population to select the entire population. Purposive sampling is the sampling technique planned for the study. 7.2.2 Sampling size 23 pediatric patients on ventilator support who meet inclusion and exclusion criteria in PICU of SJMCH should be assessed before and after implementation of VAP bundle to observe the difference in compliance with 20% precision and 95% confidence interval. 7.2.3 Inclusion criteria for sampling Patients who are on ventilator support at the time of study. 7.2.4 Exclusion criteria for sampling 1. Patients who require ventilator support for less than 48 hours. 2 .Patients on ventilator with cervical injury 3. Known hypersensitivity to chlorhexidine. 7.2.5 Instrument used 1. Baseline performa 2. Record analysis to assess clinical pulmonary infection score. 3. Observations performed to assess the practice in PICU regarding prevention of ventilator associated pneumonia. 7.2.6 Data collection method After getting a formal administrative permission samples will be identified as per inclusion and exclusion criteria using purposive sampling technique. Practice will be assessed using observation checklist and record analysis for 5 weeks.23 patients will be assessed and 2 observations each lasting for 2 hours will be made on each patient before implementation of bundle. Incidence of VAP will be assessed as per physician’s diagnosis. VAP bundle will be implemented through structured teaching and will be displayed in the PICU. A time period of 1 week is planned before assessing post implementation practice. The post implementation practice will be assessed using observation checklist and record analysis for 5 weeks. 23 patients will be assessed and 2 observations will be made on each patient. The incidence of VAP will be assessed as per doctor’s diagnosis. 7.2.7 Data analysis plan Organize data in a master sheet. Data will be analyzed using descriptive and inferential statistics. Frequency and percentages to show the distribution of subjects according to baseline variables. Paired t test for comparing pre and post practice score. Chi square for association. 7.3 Does the study require any investigation or intervention to be conducted on patients or other humans or animals? If so please describe briefly. No. 7.4. Has ethical clearance been obtained from your institution in case of 7.3? Not applicable List of references 1.Tripathi S, Malik GK, Jain A, Kohli N. A study of ventilator associated pneumonia in Neonatal Intensive Care Unit characteristics, risk factors and outcome. Internet journal of medical update 2010 Jan (cited on 2012Aug 2) ; 5(1) : Available from : URL: http://www.akspublication.com/ijmu 2. Jimenez L, Pastrana EA, Rodriguez GV, Vega GR, Rolston JD. Ventilator bundle compliance report from a neurosurgical intensive care unit. Critical care and shock 2009; 12:109-116 3. Morrow BM, Argent AC, Jeena PM, Green RJ. Guideline for the diagnosis prevention and treatment of pediatric ventilator associated pneumonia. S Afr Med 2009; 99: 1-13 4. Hoosre DTV. Ventilator associated pneumonia best practice strategies for care givers. Protection for life Kimberly Cark Health Care; 2002: 1-19 5. Augustyn B. Ventilator associated pneumonia risk factors and prevention. Critical care nurse 2007; 27 (4): 32-40 6. Michael S, Niederman MD, Donald E, Craven MD. Guideline for the management of adults with hospital acquired ventilator associated and health care associated pneumonia. American journal of respiratory critical care medicine 2005; 171: 388-416 7. Sebastian M, Lodha R, Kapil A, Kabra SK. Oral mucosal decontamination with Chlorhexidine for the prevention of ventilator associated pneumonia in children a randomized control. Pediatric critical care medicine 2012 8. Joseph NM, Sistla S, Dutta TK, Badhe AS, Rashitha D, Parija SC. Ventilator associated pneumonia in a tertiary care hospital in India role of multidrug resistant pathogens J Infect Dev Ctries 2010; 4(4):218-225 9. Juneja D, Singh O, Javeri Y, Arora V, Dang R, Kaushal A. Prevention and management of ventilator associated pneumonia. A survey on current practices by intensivists practicing in Indian subcontinent. Indian journal of anaesthesia 2011 Mar-Apr; 55(2): 122-128 10. Morris AC, Hay AW, Swann DG, Everinham K,MucCulloch C, McNutty J et al. Reducing ventilator associated pneumonia in intensive care impact of implementing a care bundle . Crit care med 2011; 3a (10): 1-7 11. Bird D, Zambuto A, Donnel CO, Silva J, Korn C, Burke R, Burke P et al. Adherance to ventilator associated pneumonia bundle and incidence of ventilator associated pneumonia in the surgical intensive care unit. Arch Surg 2010; 145(5): 465- 470 12. Patra PK, Jayashree M, Singhi S, Ray P, Saxena AK. Nosocomial pneumonia in pediatric intensive care unit. Indian pediatrics 2007 July ; (44): 511-518 13. Victor D, Rosenthal MD, Moreno CA, Gomes WV, Singh S, Ramachandran B. Effectiveness of multi dimensional approach to reduce ventilator associated pneumonia in pediatric intensive care unit of 5 developing countries: International nosocomial infection control consortium findings. American journal of infection control 2011 Oct (cited 2012, Aug 2). Available from: URL: http: // www.ajicjournal.org 14. Hamid M H, Malik M A, Masood J, Zia A, Ahmad T M. Ventilator associated pneumonia in children. Journal of the college of the college of physicians and surgeons Pakistan 2012; 22(3): 155-158. 15. Meherali S M, Parpio Y, Ali T S, Javed F. Nurses knowledge on evidence based guideline for prevention of ventilation associated pneumonia in critical care areas: a pre test post test design,http://www.ayubmed.edu.pk 2011 23 (1) 146-149. 16. Gomes V P R. Knowledge of intensive care nurses on evidence based guideline for prevention of ventilator associated pneumonia. Johannesburg. 2010: 1-176 8. SIGNATURE OF CANDIDATE 9. REMARKS OF GUIDE 10. NAME & DESIGNATION OF: MRS. SHINY MATHEW 10.1: GUIDE ASST. PROFESSOR ST.JOHN’S COLLEGE OF NURSING BANGALORE 10.2: SIGNATURE DR. LALITHA A. V 10.3: CO- GUIDE ASST. PROFESSOR ST. JOHN’S MEDICAL COLLEGE HOSPITAL BANGALORE 10.4: SIGNATURE MRS. SHEEJA P. P 11. 11.1: HEAD OF THE DEPARTMENT ASSO PROFESSOR ST. JOHN’S COLLEGE OF NURSING BANGALORE 11.2: SIGNATURE 12. 12.1: REMARKS OF THE CHAIRMAN AND THE PRINCIPAL 12.2: SIGNATURE