Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
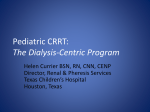
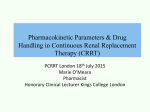
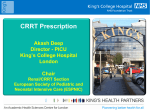
Drug Kinetics and CRRT: Parameters and Principles Morgan R. Cole, Pharm.D., BCPS Manager, HDVCH Pharmacy Services Clinical Pharmacy Specialist, Pediatric Critical Care Objectives Describe CRRT principles Understand basic pharmacokinetic (Pk) parameters Describe CRRT principles and effects on Pk Describe variances in Pk parameters Critically ill Pediatrics & Neonates Understand assumptions to estimate dosing regimens in pediatric CRRT CRRT Principles CRRT Principles Heparin Anticoagulation Citrate Anticoagulation Calcium Chloride Replacement Convective Clearance Acid Citrate Dextrose – Anticoagulation (ACD-A) Hemofiltration ~ Ultrafiltration Filter Replacement Fluid (FRF) Diffusive Clearance Hemodialysis Dialysate CRRT Principles Usual circuit priming volume ~ 100-150mL Blood, Saline, & Albumin Usual Blood Flow Rate ~ 3-5mL/kg/min Tubing and Membrane Filter impact Adsorption Adapted with permission from: Gambro Training Manual 1 and 2 Slides from Gambro Training package Last Update: February, 2008 Ultrafiltration Movement of fluid through a semipermeable membrane caused by a pressure gradient Positive, negative and osmotic pressure from non-permeable solutes Adapted with permission from: Gambro Training Manual 1 and 2 Slides from Gambro Training package Last Update: February, 2008 Convective Clearance Movement of solutes with water flow, “solvent drag”. The more fluid moved through a semipermeable membrane, the more solutes that are removed. Replacement Fluid is used to create convection Adapted with permission from: Gambro Training Manual 1 and 2 Slides from Gambro Training package Last Update: February, 2008 Diffusive Clearance Movement of solutes from an area of higher concentration to an area of lower concentration. Dialysate is used to create a concentration gradient across a semi-permeable membrane. Adapted with permission from: Gambro Training Manual 1 and 2 Slides from Gambro Training package Last Update: February, 2008 Pharmacokinetic Parameters CRRT Impact on Kinetic Parameters Usual circuit priming volume ~ 100-150mL Tubing binds drug Increases Volume of Distribution (Vd) Usual adult blood volume ~5000mL (0.07L/kg or 70mL/kg) Usual pediatric blood volume ~80mL/kg Increases Vd Adsorption Membrane Filter binds drug by “Gibbs-Donnan Effect” Increases Vd Adsorption CRRT Impact on Kinetic Parameters Usual Blood Flow Rate ~ 3-5mL/kg/min Ultrafiltrate Rate ~ Filter Replacement Fluid (FRF) Rate if the patient is kept in even fluid balance ~ 35-40mL/kg/hr (2.5L/m2/hr) Higher the rate leads to increased Clearance (Cl) Higher the rate leads to increased Cl Dialysate Rate ~ 35-40mL/kg/hr (2.5L/m2/hr) Higher the rate leads to increased Cl Sample sieving coefficients (S) Medication Gentamicin Tobramycin Amikacin S ~0.8 ~0.8 ~0.9 Medication Levofloxacin Moxifloxacin Ciprofloxacin S ~0.8 ~0.85 ~0.75 Ceftazidime Cefepime Imipenem ~0.85 ~0.85 ~0.8 Pip / Tazo Linezolid Daptomycin ~>1 ~0.8 ~0.15 Meropenem ~0.8 Vancomycin ~0.7 Valtonen, Journal of Antimicrobial Chemotherapy 2001;48,881-885 Adapted from Golper, Dialysis Transpl 1993;22:185-188 Valtonen, Journal of Antimicrobial Chemotherapy 2000;45,701-704 DelDot, Br J Clin Pharmacol 2004;58:3,259-268 Kraft, Pharmacotherapy 2003;23(8):1071-1075 Malone, Antimicrobial Agents and Chemotherapy 2001;3148-3155 Churchwell, Blood Purif 2006;24(5-6):548-554 Mariat, Crit Care 2006;10:1,R26 Fuhrmann, Journal of Antimicrobial Chemotherapy 2004;54,780-784 Guenter, Pharmacotherapy 2002;2:175-83 Tegeder, Antimicrobial Agents and Chemotherapy 1997;41(12):2640-2645 CRRT Impact on Kinetic Parameters Combined hemofiltration plus dialysis (Cldf) Convective Clearance (Filter Replacement Fluid (FRF)) Diffusive Clearance (Dialysate) Cldf = Qf * S + Qd * Sd Native clearance must be taken into account if the patient maintains renal function despite CRRT support Convective + Diffusive Clearance Ultrafiltrate Rate ~ Filter Replacement Fluid (FRF) Rate ~ 35-40mL/kg/hr (2.5L/m2/hr) Dialysate Rate ~ 35-40mL/kg/hr (2.5L/m2/hr) Clinical Pearls Medications unaffected by CRRT Ceftriaxone Metronidazole Clindamycin Lansoprazole Pantoprazole Cyclosporin Phenytoin Clinical Pearls Due to extracorporeal clearance provided by CRRT remember to hold the following if CRRT circuit goes down and consult the primary service /nephrology service Total Parenteral Nutrition / Enteral Nutrition Antibiotics except ceftriaxone, clindamycin, metronidazole Potassium, and Phosphorus supplementation H2 receptor antagonists Clinical Pearls Due to extracorporeal clearance provided by CRRT remember to monitor closely for toxicity + reduce the dose for the following if CRRT circuit goes down and consult the primary service /nephrology service Sedation (Midazolam, Lorazepam, Fentanyl, & Morphine) Pressors (Norepinephrine, Epinephrine, & Dopamine) Inotropes (Milrinone, Dobutamine, & Epinephrine) If a new circuit is initiated, a reloading phase will occur until complete adsorption occurs and a new steady state with the circuit is reached. Summary Understand CRRT principles Understand basic pharmacokinetic (Pk) parameters Critically ill Pediatrics & Neonates Understand CRRT principles and effects on Pk Vd / Pb / Cl / t1/2 Describe variances in Pk parameters Ultrafiltration / Convective vs Diffusive Clearance Adsorption / Vd / Cl Understand assumptions to estimate dosing regimens in pediatric CRRT Pb / MW / S / Sd / Clf / Cld / Cldf References Gambro Renal Products, Intensive Care Division, 14143 Denver West Parkway Lakewood, Co. 80401 Golper, Dialysis Transpl 1993;22:185-188 DelDot, Br J Clin Pharmacol 2004;58:3,259-268 Malone, Antimicrobial Agents and Chemotherapy 2001;3148-3155 Mariat, Crit Care 2006;10:1,R26 Fuhrmann, Journal of Antimicrobial Chemotherapy 2004;54,780784 Guenter, Pharmacotherapy 2002;2:175-83 Tegeder, Antimicrobial Agents and Chemotherapy 1997;41(12):2640-2645 Valtonen, Journal of Antimicrobial Chemotherapy 2001;48,881-885 Valtonen, Journal of Antimicrobial Chemotherapy 2000;45,701-704 Kraft, Pharmacotherapy 2003;23(8):1071-1075 Churchwell, Blood Purif 2006;24(5-6):548-554