Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
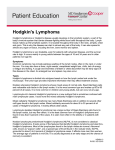
HODGKIN AND NONHODGKIN LYMPHOMA Dr. M. Sofi MD; FRCP (London); FRCPEdin; FRCSEdin Hodgkin’s Lymphoma Hodgkin's lymphoma (HL) is a type of lymphoma, which is generally believed to result from white blood cells of the lymphocyte kind. About half of cases of Hodgkin's lymphoma are due to Epstein–Barr virus (EBV) Most common primary localizations are cervical (60 80%), mediastinal, and inguinal lymph nodes. Hodgkin’s lymphomas disseminate both via lymphatic vessels or per continuitatem into lymphatic organs as well as by blood vessels or per continuitatem into extralymphatic organs. Hodgkin’s Lymphoma Epidemiology • The incidence rate is at 2-3/100,000 per year. The age peak lies at approx. 32 years. • Hodgkin lymphoma is one of the most treatable forms of cancer. • About 75 percent of people diagnosed with Hodgkin lymphoma can be cured with treatment. • Over 90 percent of people live at least 10 years after treatment. Classification WHO classification: There are two main types of lymphoma I. Nodular Lymphocyte-predominant Hodgkin’s lymphoma (NLPHL) • The NLPHL encompasses almost 5% of all Hodgkin’s lymphomas. • As opposed to the classical Hodgkin’s lymphomas the malignant cells are referred to as L&H (lymphocytic and histiocytic) • For therapeutic purposes, nodular lymphocytepredominant HL is managed in the same way as indolent non-Hodgkin lymphoma Classification II. Classical Hodgkin’s Lymphoma (cHL) • Nodular sclerosing (NSHL) • Mixed cellularity (MCHL) • Lymphocyte-rich (LRHL) • Lymphocyte-depleted (LDHL) • Not classified Tumor cells of the classical Hodgkin’s lymphomas are referred to as Hodgkin and Reed-Sternberg cells (H-RS) Stage-adapted therapy allows long term cure in more than 80 percent of all patients. Hodgkin’s lymphoma is one of the oncological diseases with the highest cure rates in adults Features of Hodgkin lymphoma include: may be present (above the diaphragm in 80% of patients) Constitutional symptoms [>10% of total body weight] are present in 40% of patients; collectively, these are known as is observed in about 35% of cases fever is observed (high fever for 1-2 wk, followed by an afebrile period of 1-2 wk) Features of Hodgkin lymphoma include: of those may be present due to a large mediastinal mass or lung involvement; rarely, hemoptysis occurs , precipitated by drinking alcohol, occurs in fewer than 10% of patients but is specific for Hodgkin lymphoma rarely occur • May present with in NSHL has a strong genetic component and has often previously been diagnosed in the family. Physical Examination can be seen in: the (neck) - 60-80% 6-20% (groin) - 6-20% (back of the throat, including the tonsils) or occipital (lower rear of the head) or epitrochlear areas is infrequently observed may be present may develop in patients with mediastinal lymphadenopathy Differential Diagnoses • Cytomegalovirus • Infectious Mononucleosis • Non-Hodgkin Lymphoma • Systemic Lupus Erythematosus • • • • • • Sarcoidosis Serum Sickness Small Cell Lung Cancer Syphilis Toxoplasmosis Tuberculosis Test Laboratory analyses Imaging Bone-marrow puncture Investigations Comments • Complete blood cell count, including leukocyte count with differential • Erythrocyte sedimentation rate • LDH, GOT, GPT, AP, Gamma GT, uric acid, creatinine • Chest X-rays • CT scan of the neck (with contrast medium) • CT scan of the abdomen (with contrast medium) • PET scan: Initial staging of Hodgkin lymphoma • Aspirate (cytology) • Biopsy (histology) Staging according to Ann Arbor Classification Stage I A single lymph node area or single extra-nodal site Stage II 2 or more lymph node areas on the same side of the diaphragm Stage III Lymph node areas on both sides of the diaphragm Stage IV Disseminated or multiple involvement of the extranodal organs Addendum A No B symptoms Addendum B Presence of B symptoms Lymphocyte Hodgkin's lymphoma, mixed-cellularity type Reed – Sternberg Cell H L: Reed-Sternberg cells, Eosinophils , Plasma cells Non-Hodgkin lymphomas: is a group of blood cancers that includes all types of lymphoma except Hodgkin's lymphomas. Non-Hodgkin lymphomas (NHLs) are tumors originating from lymphoid tissues, mainly of lymph nodes. These tumors may result from chromosomal translocations, infections, environmental factors, immunodeficiency states, and chronic inflammation Signs and symptoms • Peripheral adenopathy: Painless and slowly progressive; can spontaneously regress • Primary extranodal involvement and B symptoms: • Uncommon at presentation; however, common with advanced, malignant transformation or end-stage disease • Bone marrow: Frequent involvement; may be associated with cytopenias(s); fatigue weakness more common in advanced-stage disease Non-Hodgkin lymphomas Signs and symptoms : Most patients have a more varied clinical presentation: : More than one third of patients; most common sites are GI/GU tracts (including Waldeyer ring), skin, bone marrow, sinuses, thyroid, CNS : within 6 months; in approximately 30-40% of patients Physical Examination Examination in patients with may demonstrate: lymphomas may result: : Usually in Burkitt lymphoma : Associated with cutaneous T-cell lymphoma Complications: Disease-related complications include: (neutropenia, anemia,thrombocytopenia) secondary to thrombocytopenia, DIC secondary to neutropenia or arrhythmias secondary to cardiac metastases • and/or parenchymal lesions (lymphocytosis) in leukemic phase of disease (SVC) syndrome secondary to a large mediastinal tumor secondary to vertebral metastases , in a patient with GI lymphoma secondary to tumor invasion Testing: Laboratory studies with suspected NHL include: : May show • • • • • Anemia Thrombocytopenia Leukopenia Pancytopenia Thrombocytosis : May show elevated LDH, LFT and calcium levels : Especially in patients with diffuse large cell immunoblastic or small non cleaved histologies serology: Patients with adult T-cell leukemia/lymphoma : In patients in whom rituximab therapy is planned of lymph node, bone marrow, peripheral blood : NHL associated with monoclonal gammopathy Imaging studies for NHL include: with small bowel follow-through: In patients with head and neck involvement and those with a GI primary lesion of the neck, chest, abdomen, and pelvis (CT-CAP) : For opposite testis in male patients with a testicular primary lesion : Only in patients with bone pain, elevated alkaline phosphatase, or both : Procedures: : For staging rather than diagnostic purposes (extra-nodal biopsy): For lymphoma protocol studies for CSF analysis in patients with: Management: The treatment of NHL varies greatly and include: : Most common; usually combination regimens : Possible role in relapsed high-risk disease • Transfusions of blood products • Antibiotic Pharmacotherapy • Medications include: