Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
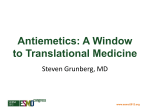
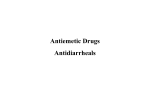
CHEMOTHERAPY INDUCED NAUSEA AND VOMITING Dr. Rotich Julius (BPharm) Pharmacist, MTRH 1/11/2016 OUTLINE Definitions General overview of N/V Pathophysiology of CINV Types of CINV Drugs used in management of CINV Summary DEFINITIONS Nausea is usually defined as the inclination to vomit or as a feeling in the throat or epigastric region alerting an individual that vomiting is imminent ( subjective ). Nausea ---Autonomic symptoms Vomiting is defined as the ejection or expulsion of gastric contents through the mouth, often requiring a forceful event (reflexive ) Vomiting. Contraction + forced expel of GI content Retching is the contraction of the abdominal wall,diaphragm &thoracic muscles without expulsion. Retching---- Contractions of muscles CAUSES OF NAUSEA/ VOMITING Early pregnancy Psychogenic vomiting Bulemia Pyloric channel ulcer Acute gastritis Gastric retention Viral gastroenteritis Acute gastroenteritis Myocardial infarction Peritonitis Acute obstruction Neurologic emergency Drug toxicity Cancer therapy Drug withdrawal HISTORY AND PE Timing of symptoms Relation to meals Associated symptoms Last menstrual period Comorbid conditions Epidemiologic data Drug history Physical Examination LABORATORY Rule out obstruction and peritonitis HCG Urinalysis Electrolytes, BUN, creatinine, glucose Transaminases, amylase EKG, head CT, upper GI &/or endoscopy GENERAL MANAGEMENT Phenothiazines Centrally acting non-phenothiazines Dramamine & Scopolamine Pregnancy Antivert Motion sickness Tigan Vestibular disturbances Compazine & Phenergan No approved Others Marinol, Zofran, Kytril PATHOPHYSIOLOGY • Two sites in the brainstem— --the vomiting center and the chemoreceptor trigger zone—are important to emesis control. The vomiting center(VC) consists of an intertwined neural network in the nucleus tractus solitarius that controls patterns of motor activity. The chemoreceptor trigger zone (CTZ), located in the area postrema, is the entry point for emetogenic stimuli. • Enterochromaffin cells in the gastrointestinal tract respond to chemotherapy by releasing serotonin. Serotonin binds to 5-HT3 receptors, which are located not only in the gastrointestinal tract, but also on vagal afferent neurons and in the nucleus tractus solitarius and the area postrema. Grunberg SM, Hesketh PJ. Control of chemotherapy-induced emesis. N Engl J Med. 1993;329: 1790-1796. PATHOPHYSIOLOGY CTD’ • The activated 5-HT3 receptors signal the chemoreceptor trigger zone via pathways that may include the afferent fibers of the vagus nerve. • Serotonin also may bind with 5-HT3 receptors in the brainstem. • Other neurotransmitters, including dopamine and substance P, also influence the chemoreceptor trigger zone. • Afferent impulses from the chemoreceptor trigger zone stimulate the vomiting center, which initiates emesis.1 Grunberg SM, Hesketh PJ. Control of chemotherapy-induced emesis. N Engl J Med. 1993;329: 1790-1796. PATHOPHYSIOLOGY CTD’ Nausea & vomiting are complex interaction from different systems Central vomiting center (medulla) CTZ (5-HT3 ,D2,NK1 ) Gastrointestinal(visceral afferents(5HT3,D2,NK1 ) Cerebral cortex (sensory) Vestibular system (H!, muscarinic ) PATHOPHYSIOLOGY OF CHEMOTHERAPY-INDUCED EMESIS CHEMOTHERAPY-INDUCED NAUSEA AND VOMITING AN UNMET MEDICAL NEED Over one million cancer patients receive chemotherapy each year 20% highly emetogenic chemotherapy (HEC) Chemotherapy-induced nausea and vomiting (CINV) Among the most distressing side effects of chemotherapy Disrupt patients’ daily lives Patients may even delay scheduled chemotherapy J Clin Oncol 1997;15(1):103-9 American Cancer Society. Cancer Facts & Figures 2001 EMETOGENIC POTENTIAL OF SINGLE ANTINEOPLASTIC AGENTS HIGH Risk in nearly all patients (> 90%) MODERATE Risk in 30% to 90% of patients LOW Risk in 10% to 30% of patients MINIMAL Fewer than 10% at risk PATIENT-SPECIFIC RISK FACTORS FOR CINV Age <50 years Women > men History of light alcohol use History of vomiting with prior exposure to chemotherapeutic agents Other risks History of motion sickness History of nausea or vomiting during pregnancy History of anxiety ASHP. Am J Health Syst Pharm. 1999:56:729-764; Balfour and Goa. Drugs. 1997:54:273-298. TYPES OF CINV: DEFINITIONS Acute (post-treatment) Delayed Learned or conditioned response from poorly controlled nausea and vomiting associated with previous chemotherapy Breakthrough CINV that begins after first 24 hours May last for 120 hours Anticipatory Occurs within first 24 hours after administration of cancer chemotherapy CINV that occurs despite prophylaxis and requires rescue Refractory Occurs during subsequent treatment cycles when prophylaxis and/or rescue has failed in previous cycles CHEMOTHERAPY-INDUCED EMESIS: KEY TREATMENT MILESTONES Aprepitant, March 2003 Palonosetron July, 2003 PHARMACOLOGIC AGENTS Corticosteroids Dopamine antagonists Serotonin (5-HT3) antagonists NK-1 receptor antagonists Cannabinoids STEROIDS Corticosteroids are an integral part of antiemetic therapy for acute and delayed CINV. When used in combination with other antiemetics, corticosteroids exert a booster effect, raising the emetic threshold. Dexamethasone is the most frequently used corticosteriod. Steroids are sometimes underutilised, owing to concerns regarding potential adverse events . Usually, when used in the short term as antiemetic therapy, corticosteroids are well tolerated. Adverse events include moderate-to-severe insomnia (45%), indigestion/epigastric discomfort (27%), agitation (27%), increased appetite (19%), weight gain (16%) and acne (15%) DOPAMINE ANTAGONISTS These agents include phenothiazines, butyrophenones and substituted benzamides. One of the most frequently used benzamides is metoclopramide. However, in patients receiving cisplatin-based chemotherapy,the effects of conventional doses of metoclopramide are not significantly different from placebo. Although not effective in the acute phase, metoclopramide in combination with corticosteroids has proven efficacy in the prevention of delayed CINV SEROTONIN ANTAGONISTS Generation 1/2 Ondansetron, granisetron, tropisetron, dolasetron and,more recently, palonosetron. When given at equivalent doses for the prevention of acute emesis, 5-HT3-RAs have equivalent efficacy and safety and can be used interchangeably . Single-dose daily schedules have similar efficacy to multiple dose daily schedules, and oral forms have been shown to be as effective as I.V. forms . As a class, 5-HT3-RAs are well tolerated; common adverse events include mild headache,transient elevation of hepatic enzymes and constipation BENZODIAZEPINES Benzodiazepines can be useful additions to antiemetic regimens in certain circumstances. They are often used to treat anxiety and reduce the risk of anticipatory CINV. Benzodiazepines are also used in patients with refractory and breakthrough emesis Olanzapine, an atypical antipsychotic drug, has potential antiemetic properties due to its ability to bind at several receptors involved in the CINV pathways. NK-1 RECEPTOR ANTAGONISTS They exert their antiemetic action through the inhibition of substance P in the emetic pathways in both the central and peripheral nervous systems. Aprepitant , casopitant,, netupitant and rolapitant, are agents in this class. Aprepitant is available for oral and as fosaprepitant in the i.v. administration form. It is recommended for use in the acute phase in combination with a 5-HT3-RA plus dexamethasone . CANNABINOIDS Cannabinoids (e.g. dronabinol and nabilone) possess weak combined antiemetic efficacy with potentially beneficial sideeffects, including sedation and euphoria. This makes them a useful adjunctive therapy in selected patients; in the ASCO and NCCN guidelines, cannabinoids are recommended for patients intolerant of or refractory to 5-HT3-RA or steroids andaprepitant. In a systematic review of the efficacy of oral cannabinoids in the prevention of nausea and vomiting, cannabinoids were found to be slightly better than dopamine receptor antagonists,including phenothiazines, haloperidol and metoclopramide. Despite this, their clinical utility was found to be generally limited by the high incidence of adverse events, such as dizziness, dysphoria and hallucinations. META-ANALYSIS OF EFFICACY OF 5-HT3RA IN PREVENTION OF DELAYED EMESIS FROM CHEMOTHERAPY Reviewed 5 studies, 1,716 pts comparing 5-HT3 RA to placebo, 5 studies, 2,240 pts comparing 5-HT3 RA + dexamethasone to dexamethasone alone 5-HT3 RA as monotherapy Absolute RR (95% CI) 8.2% (3.0-13.4) NNT 12.2 Number of doses per protected pt: 74.4 5-HT3 RA as adjunct to dexamethasone Absolute RR (95% CI) 2.6% (-0.6-5.8) NNT 38.8 Number of doses per protected pt: 423 Geling and Eichler, JCO 23:1289-1294 ASCO 2006/NCCN 2009 RECOMMENDATIONS BY RISK CATEGORY High (>90% emetic risk) Three-drug combination of a HT3 Including AC containing regimens serotonin receptor antagonist, dexamethasone, and aprepitant Moderate (>30% to 90% emetic risk) Two-drug combination of a HT3 serotonin receptor antagonist and dexamethasone (+/aprepitant for selected patients) Low (10% to 30% emetic risk) Dexamethasone 8-12 mg Minimal (<10% emetic risk No antiemetic routinely HOW CAN WE IMPROVE THE VALUE OF CARE IN CINV? Cost Value = Quality Cure Rate Nausea or Emesis Functioning Side Effects Compliance or Patient Inconvenience • Direct • Indirect SUMMARY 5HT3 RA’s are therapeutically good & major advance in supportive care for control of acute emesis Treatment guidelines have changed over time Degree of nausea incurred has been refined for many agents Delayed CINV recommendations are updated Prevention of CINV has improved, but challenges remain Improving detection of CINV, especially after 24 hours Educating patients and oncology healthcare givers The development and evaluation of clinically useful assessment tools Further development of regimens to treat delayed CINV