Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
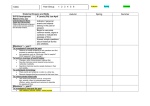
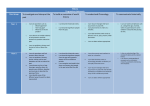
Guidance for Implementation and Completion of the Chronology of Significant Events form in School Nurse and Health Visitor records Aim The chronology of significant events will provide health professionals with an overview of significant events, which may impact on the child’s health and wellbeing. This enables health professionals to undertake a continuous assessment of the child’s needs within the wider family Implementation The long-term aim is for each child’s health visitor and school health record to include a chronology of significant events Implementation of the chronology will be a phased process A chronology of significant events form should be commenced in all new records i.e. all new births and transfers into Trafford A chronology of significant events should be commenced in all records where the children are brought to safeguarding supervision A chronology of significant events will be commenced when the child attends for a routine developmental check or health screening appointment A chronology of significant events will be commenced by school nurses at school entry and transition to year 7 The chronology will be completed from current date and only completed retrospectively when safeguarding or other health concerns identify a need for a chronology to be commenced. Advice and support re this aspect of record keeping can be accessed from the Named Nurses for Safeguarding Children. The chronology of significant events is discussed at Level 3 safeguarding children training Completion of chronology 1. The first entry of the Health Visitor/ School Nurses chronology of significant events will be the Health Visitor’s/ School Nurses first assessment of level of need of the child and family (i.e. antenatal contact, birth visit, transfer in contact) unless other information i.e. 2. 3. 4. 5. 6. 7. 8. child protection information precedes the initial contact and assessment The chronology should include information from assessments and documentation including observations at contacts Chronology should include information received from other sources i.e. A&E discharge information Chronology should include information about referrals to other services Chronologies should include information about the parenting capacity, family and environmental factors and child’s developmental needs Guidance on what information may be included in the chronology of significant events is attached to the chronology of significant events form see appendix A Entries into chronology should be a brief statement of information and not duplication of information recorded in records (therefore significant events not all contacts need to be recorded). Chronologies should be filed at front of health professionals records and be immediately accessible Review date of guidelines May 2011 Appendix A Page Number: TRAFFORD HEALTH RECORDS CHRONOLOGY OF SIGNIFICANT EVENTS Name: Date of Birth: Address: Date & Time Event Signature/ Professional Status This form is to be used to record a brief chronology of events that could (singly or collectively) have an adverse effect on health, safety or wellbeing of the children This is a two page document – as indicated overleaf SIGNIFICANT EVENTS Address Changes Record all changes of address and also other contact addresses where child can be found. Level of Need Identified Universal Services Common Assessment Form Completed Record and file common assessment documentation. Child In Need Meetings Child Protection Strategy Meeting/Case Conference Record the outcome – to include conference recommendations. Court Orders / Children in Care Eg, Private law proceedings or care / supervision orders. Death/Significant Illness of a Child/Parent Carer To include incidents that may impact (directly or indirectly) on the safety or direct care of the child. Drug and Alcohol Related Incidents To include other agency involvement (if applicable). Changes of GP or School (including not registered with GP or School) A pattern of frequent changes may emerge. Housing Problems To include house repossession; family living in bed and breakfast accommodation; damp and squalid conditions. Hospital Attendance Any attendance at A&E, Walk in Centre or GP Out of Hours of child. Attendance of a parent or main carer, when it may impact on the direct care. Inpatient Episodes Such as injuries, accident or non-accidental – eg, RTA, ingestion, and safety/neglect issues. Non-Compliance of a Parent/Main Carer with Health Services Non-attendance/compliance with health care or prescribed treatment, that could adversely affect the parent’s/carer’s ability to adequately care for/protect the child, eg, drug service; mental health services etc. Non-Compliance with Health Care / Paediatric/Health Related Services This may indicate a pattern of repeated no access with planned visits; and failing to attend for immunisation; health screening. Non-attendance for appointments that could result in the child’s health being compromised, eg, cardiology, Audiology etc. treatment plan. Concerns/Disclosure To include concerns from health professional; friends; family or anonymous allegations. Child accommodated by the local authority – record the reason for the child to be out of the family home. Domestic Abuse Domestic abuse incident received/MARAC referral. Social Services Referrals Record reason for contact.