Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
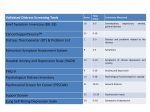
Running head: MEASUREMENT OF STRESS IN THE ONCOLOGY POPULATION Measurement of Stress in the Oncology Population An Integrative Review Merlessa Rosacina Nursing Science II Dr. Mary O’Keefe March 26, 2015 1 MEASUREMENT OF STRESS IN THE ONCOLOGY POPULATION 2 Introduction The purpose of this integrative literature review is to identify the best, consistent measurement method for assessing stress in oncology patients. Stress is an occurrence in everyday life and is a phenomenon spanning across all generations, ages, and genders. According to the American Psychological Association (2012), a healthy stress level is considered a score of 3.6 on a 10 point scale, but Americans report a mean stress level of 4.9 in the Stress in America survey. Thirty-two percent of individuals value the importance of discussing stress management with their healthcare providers, yet only 17% report these conversations actually happening often (The American Psychological Association, 2012). Clinicians and patients have open conversations on physical health complications and the same regard needs to be given to psychological complications. This author works at a cancer facility where patients voice recurrent psychological concerns including fear of death, financial woes, loss of independence, and embarrassment, all of which impact stress levels. Levels of stress vary depending on specific stressors and situation. Consistent assessment and monitoring of stress prevents progression into higher levels and adverse physical symptoms caused by stress, and inhibits extended periods of stress known to cause further health complications. The articles used in this integrative review were guided with the following question: What are current methods used to assess stress in the oncology field? Search Strategy The review was conducted through a Summons search via The University of Texas’ Moody Medical Library website. Boolean operators are used to expand or restrict a search (Polit & Beck, 2014, p. 2). Delimiters used in this review include “psychological”, “distress”, and MEASUREMENT OF STRESS IN THE ONCOLOGY POPULATION 3 “cancer.” Articles are taken from CINAHL, PubMed, PubMed and Psychological Abstracts through the Summons search. CINAHL is a nursing based databases that includes more than 1 million records, and PubMed is considered the premiere source for bibliographic coverage that contains more than 21 million records (Polit & Beck, 2014, p. 122). The original search contained articles no older than 2004 to include the most current studies, but included few older, significant articles. This integrative review relies on primary sources to maintain objectivity and tentativeness. The search was difficult because the majority of the articles resulted were secondary sources, which I excluded to remain unbiased. Nonresearch references that do not show evidence in solving research problems are excluded. The search originally yielded 17,405 results, but due to exclusion criteria, only 13 were used. Summary of Research Findings The table below presents the 13 articles used in tabular format. Each research study was reviewed and broken down to summarize its study purpose, sample size, design, findings, instruments, strengths, and weaknesses. Running head: MEASUREMENT OF STRESS IN THE ONCOLOGY POPULATION Author/ s Title Journal Date (yr/vol/ iss) Kugaya, A., Akechi, T., Okuyama , T., Nakano, T., Mikami, I., Okamura , H., Uchitomi , Y. Prevalen ce, Predictiv e Factors, and Screenin g for Psycholo gic Distress in Patients with Newly Diagnose d Head and Neck Cancer Cancer, Volume 88, Issue 12 11/20/2 000 Researc h Questio n Design & Metho d Does the detection of psycholog ic distress in the pretreatm ent period improve the patient’s adaptatio n to the treatment or rehabilita tion? Crosssectiona l study Population Sample Data Collection/ (Size, Type) Instrumen ts 107 patients diagnosed with head and neck cancer free from cognitive impairment Sociodemog raphic data and medical data obtained from subjects, medical records, and physicians. Interview to assess social support. The Hospital Anxiety and Depression Scale (HADS) for measuring psychologica l distress measured anxiety and depression. Analysis Finding s 4 Strengt hs Limitatio ns Conclusi on Implicati ons (Take home message) Intergrou p comparis on using the chi square test, Fisher exact test, unpaired Student’s t TEST, and variance analysis. Of 107 subjects, 18 had an adjustme nt disorder or major depressio n. Thirtysix, 7, and 35 met criteria for alcohol depende nce, alcohol abuse, and nicotine depende nce. Older adults living alone showed significan tly higher score of psycholo gic distress. Good sample size. Appropr iate methods . No other group or population to compare results with. HADS is a good measurem ent to track psychologi cal distress in cancer patients. Head and neck cancer patients who have advanced disease or live alone should be assessed so that psychologi cal distress can be detected and interventio n made. MEASUREMENT OF STRESS IN THE ONCOLOGY POPULATION Author/ s Title Journal Date (yr/vol/ iss) de Haes, J., van Knippen berg, F., Neijt, J.P. Measuri ng psycholo gical and physical distress in cancer patients: structure and applicati on of the Rotterda m Sympto m Checklist British Journal of Cancer Volume 62 1990 Researc h Questio n Design & Metho d Is the Rotterda m Symptom Checklist a reliable method in measurin g psycholog ical and physical distress in cancer patients? Crosssectiona l study Random ised control trial Population Sample Data Collection/ (Size, Type) Instrumen ts RSCL stability investigated in 3 studies: The Rotterdam Symptom Checklist 95 female cancer patients visiting an outpatient clinic 56 patients participating in a randomised control trial comparing two chemotherap y regimens for the treatment of advanced ovarian cancer 20 cancer patients compared the quality of life with 611 patients of ‘normal’ controls. 5 Analysis Finding s Strengt hs Limitatio ns Conclusi on Implicati ons (Take home message) Principal compone nt analysis in all 3 studies. Subscales in the RSCL were developed on the factors identified. Good sample size. Allows 3 groups of compari son. Lack of prior studies related to the RSCL. Reliability of the scale constructe d on the basis of the results was consistentl y high, and can be used as a basis for future studies. The RSCL shows promising potential in measuring psychologi cal distress in oncology patients. MEASUREMENT OF STRESS IN THE ONCOLOGY POPULATION Author/ s Title Journal Date (yr/vol/ iss) Jacobsen , P.B., Donovan , K.A., Trask, P.C., Fleishma n, S.B., Zabora, J., Baker, F., Holland, J.C. Screenin g for Psycholo gic Distress in Ambulat ory Cancer Patients Cancer, Volume 103, Issue 7 02/22/2 005 Researc h Questio n Design & Metho d Determin e whether the singleitem Distress Thermom eter (DT) compared favourabl y with longer measures currently used to screen for distress. Crosssectiona l study Population Sample Data Collection/ (Size, Type) Instrumen ts 380 cancer patients recruited from 5 different cancer hospitals, 18 years or older, diagnosed with cancer, scheduled for an outpatient appointment, able to understand English and informed consent Self-report questionnair e The Distress Thermomete r The Hospital Anxiety & Depression Scale 6 Analysis Strengt hs Limitatio ns Conclusi on Implicati ons (Take home message) Receiver operating characteri stic Curve analyses Chi square analyses t tests Brief Symptom Inventory Finding s DT scores yielded good overall accuracy in comparis on to the HADS and BSI cutoff score. Patients had a DT scores of greater than or equal or 4 are more likely to be women, poorer performa nce status, report practical, family, emotiona l, and physical problem, compare Good sample size. Appropr iate method of data collectio n. Limited previous research on the effectivene ss of DT. Limited racial diversity Crosscultural differences, a previous study was done in Japan that yielded different results The singleitem DT compares favourably with longer measures used to screen for distress. Further research is needed to support this considerin g the limited studies regarding the DT tool. The DT tool helps identify patients with a range of problem that were likely to reflect psychologi c distress. MEASUREMENT OF STRESS IN THE ONCOLOGY POPULATION Author/ s Title Journal Date (yr/vol/ iss) Researc h Questio n Design & Metho d Population Sample Data Collection/ (Size, Type) Instrumen ts 7 Analysis Finding s Strengt hs Limitatio ns Conclusi on Implicati ons (Take home message) d with patients who have DT scores <4. Bleiker, E., Pouwer, F., van der Ploeg, H., Leer J., Ader, H. Psycholo gical distress two years after diagnosis of breast cancer: frequenc y and predictio n Patient and Educatio n Counsell ing, Volume 40, Issue 3 06/200 0 Investigat e the frequency of high stress levels of psycholog ical distress in women with early stage breast cancer almost two years after diagnosis and identify characteri stics associate with longterm distress. Crosssectiona l study 244 women with a histological diagnosis of breast cancer treated with a mastectomy or breast conserving surgery, no previous neoplasms, younger than 75 years of age, and knowledge of the Dutch language Questionnai re during the period of radiotherapy , and again after 1 and a ½ years after the first assessment. Holmes and Rahe Readjustme nt Rating Scale Social Experience Checklist SelfAssessment Questionnai re-Nijmegen Impact of Event Scale Descriptiv e statistics Explorati ve analyses Pearson’s and Spearman ’s correlatio nal methods Confirmat ive multiple regressio n analysis Sixteen percent of the women reported a high level of psycholo gical distress. Large sample size. No compariso n group. Two part analyses method Cultural barrier. This is a good, thorough study. It was done in a Dutch setting, and may need cross cultural studies in the future for further support. Patients with early diagnosis and good prognosis still experience high levels of stress and need active screening. MEASUREMENT OF STRESS IN THE ONCOLOGY POPULATION Author/ s Title Journal Date (yr/vol/ iss) Hoffman , B., Zevon, M., D’Arrigo, M., Cecchini, T. Screenin g for Distress in Cancer Patients: The NCCN RapidScreenin g Measure PscyhoOncolog y, Issue 13 03/03/2 004 Researc h Questio n Design & Metho d Population Sample Data Collection/ (Size, Type) Instrumen ts The goal of this study is to examine the psychome tric properties of the NCCN DMSM and explore its psychome tric relationsh ip to a widely used and validated measure of stress. Crosssectiona l study 68 outpatient cancer patients Distress Managemen t Measure 27 males, 41 females Distress Thermomete r 60 White, 3 Hispanic, 3 AfricanAmerican, 1 Asian, 1 other 44 married, 10 single, 11 divorced/sep arated, 3 widowed Mean age 53.7 years of age, age range 17 to 90 Diagnosed an average of 15.1 months prior to participation 14 breast cancer, 11 lymphoma, 9 colon cancer, 10 leukemia, 20 other cancers, 4 Distress domain checklists Brief Symptom Inventory Global Severity Index 8 Analysis Finding s Strengt hs Limitatio ns Conclusi on Implicati ons (Take home message) Receiveroperating characteri stic curves Internal consisten cy coefficien t Alphas The DMSM has moderate ability to detect distress identified by the BSI and BSI-18. Good sample size. Mostly Caucasian – limits the generizabil ity. There’s no single cutoff score maximizes sensitivity and specificity for DMSM. Lower cutoff scores risk overidentifying distressed individuals , while higher score cutoffs risk missing truly distressed individuals . The NCCN Distress Managem ent Screening Measure is an efficient, nonthreat ening method for the rapid screening and identificati on of distress experience d by cancer patients. Further research is needed with this tool. MEASUREMENT OF STRESS IN THE ONCOLOGY POPULATION Author/ s Title Journal Date (yr/vol/ iss) Researc h Questio n Design & Metho d Population Sample Data Collection/ (Size, Type) Instrumen ts 9 Analysis Finding s Strengt hs Limitatio ns Conclusi on Implicati ons (Take home message) with uncertain diagnosis Strong, V., Waters, R., Hibberd, C., Rush, R., Cargill, A., Storey, D., Walker, J., Wall, L., Fallon, M., Sharpe, M. Emotion al Distress in Cancer Patients: The Edinburg h Cancer Centre Sympto m Study British Journal of Cancer, Volume 96 02/20/2 007 Measure the prevalenc e of clinically significan t emotional distress and to determine its demograp hic and clinical associatio ns in a large sample of outpatien ts with a variety of cancer types attending a regional cancer centre. Crosssectiona l study 3071 outpatient cancer patients above the age of 18 Hospital Anxiety and Depression Scale Confident ial Interval Cutoff measure ments Nearly a quarter of the sample had clinically significan t emotiona l distress. Large sample size. All outpatient clinics were not measured, underestim ating the prevalence of emotional distress. Definition of clinically significant emotional distress is based on a self-rated questionna ire and excludes patients experienci ng transient distress. The study has a great sample size, but has a lot of missing informatio n and needs to be more developed. The population with the highest distress score include being female, having active disease, and an age of less than 65. Knowing this, special attention is needed for this population . MEASUREMENT OF STRESS IN THE ONCOLOGY POPULATION Author/ s Title Journal Date (yr/vol/ iss) Keller, M., Sommerf eldt, S., Fischer, C., Knight, L., Riesbeck, M., Lowe, B., Herfarth, C., Lehnert, T. Ozalp, E., Cankurta ran, E., Soygur, H., Geyik, P., Jacobsen , P. Recognit ion of distress and psychiatr ic morbidit y in cancer patients: a multimethod approach Screenin g for psycholo gical distress in Turkish cancer patients Annals of Oncolog y, Volume 15, Issues 8 PsychoOncolog y, Volume 16, Issue 4 04/08/2 004 08/16/2 006 Researc h Questio n Design & Metho d Explore how distressed patients can be identified in a specific setting in order to provide appropria te support. Crosssectiona l study Aim is to investigat e distress impact on oncology patients in Turkey and determine optimal cut-off score on the Distress Crosssectiona l study Population Sample Data Collection/ (Size, Type) Instrumen ts 189 consecutively recruited cancer patients upon admission to surgical oncology wards Diagnostic psychiatric interview 182 cancer patient in Ankara Oncology Education And Research Hospital 10 Analysis Distress Thermomete r The Problem List The European Organizatio n for Strengt hs Limitatio ns Conclusi on Implicati ons (Take home message) Multilevel approach Hospital Anxiety and Depression Scale Questionnai re Finding s Descriptiv e Statistics Seventyseven percent of patients with a psychiatr ic disorder were properly identified by physician s. Nurse identified 75% correctly. Good sample size. Scores on DT were moderate ly correlate d to the HADS and EORTC concludi ng its acceptabi lity Allows quantita tive predicti ons to be made. Quick process. Limited sensitivity and specifity to psychologi cal morbidity Limited resource, unable to conduct a diagnostic interview with all patients A good study, but needs more informatio n regarding morbidity. The study did not effectively support that aspect. Further training is needed to improve communic ation and diagnostic skills of nurses and doctors. The study needs further research since it is the first step for quick distress screening in Turkey. More informatio n needs to Statisticall y effective studies still need further process for real-life results. No other group tested for compariso n. Not generalizab le to outpatients . Majority is of low socioecono mic status and education level. Questionna MEASUREMENT OF STRESS IN THE ONCOLOGY POPULATION Author/ s Title Journal Date (yr/vol/ iss) Researc h Questio n Design & Metho d Population Sample Data Collection/ (Size, Type) Instrumen ts Thermom eter for identifyin g clinically significan t distress by comparin g DT’S performa nce with existing screening methods. Grassi, L., Johansen , C., Annunzi ata, M., Capovilla , E., Constant ini, A., Gritti, P., Torta, R., Bellani, M. Screenin g for distress in cancer patients Cancer, Volume 119, Issue 9 05/1/20 13 The objective of this study is to examine the validity and acceptanc e of the DT in a large saple of Italian patients with cancer. 11 Analysis Finding s Strengt hs Limitatio ns Conclusi on Implicati ons (Take home message) Research and Treatment of Cancer Quality of Life Questionnai re criterion validity. ires may have been manipulate d. Sample size needs to be greater for the test to be valid. be obtained about the patients’ psychosoci al activities. Not cross validated in different sample of patients. Crosssectiona l study 1108 outpatients with cancer were recruited from 38 representativ e oncology center in Italy Distress Thermomete r, The Problem List, The Hospital Anxiety and Depression Scale, Brief Symptom Inventory, Visual Analog Scale Descriptiv e Analysis, Pearson r correlatio n tests, chisquare test, Student t tests, analyses of variance DT cutoff scores greater than or equal to 4 and greater than or equal to 5 had optimal sensitivit y and specificit y relative to HADS and BSI cutoff scores for Good sample size. Quick data collectio n. Precise, quantita tive, and numeric al data. Generaliza bility to cancer patients with poor outlook should be examined. Restricted research on effectivene ss of DT. The majority of cancer sites test included The study needs further developme nt of the DT tools, but shows promising trends on identifying patients with risk of psychologi cal distress. The DT thermome ter is commonly used to assess psychologi cal distress in cancer patients, but needs further developme nt for reliability especially for such a MEASUREMENT OF STRESS IN THE ONCOLOGY POPULATION Author/ s Title Journal (yr/vol/ iss) Date Researc h Questio n Design & Metho d Population Sample Data Collection/ (Size, Type) Instrumen ts 12 Analysis Finding s Strengt hs Limitatio ns Conclusi on Implicati ons (Take home message) general caseness and more severe psycholo gical distress. Patients with greater than or equal to 4 on the DT are more likely to be women, a history of psycholo gical problem, report more stressful events in the last year, and currently have more family, emotiona l, and physical problem related to GI and breast cancer, and did not compare to other cancer sites. Methodolo gy could be improved. Further history regarding previous psychiatric issues need to be studied. Treatment algorithms need developme nt. common tool in use. MEASUREMENT OF STRESS IN THE ONCOLOGY POPULATION Author/ s Title Journal Date (yr/vol/ iss) Researc h Questio n Design & Metho d Population Sample Data Collection/ (Size, Type) Instrumen ts 13 Analysis Finding s Strengt hs Limitatio ns Conclusi on Implicati ons (Take home message) cancer or treatmen t. Knobf, M., MajorCampos, M., Chagpar, A., Seigerma n, A., Mccorkle , R. Promoti ng quality breast cancer care: Psychoso cial distress screenin g Palliative and Supporti ve Care, Volume 12, Issue 1 02/2014 The purpose is to evaluate the feasibility of implemen ting psychosoc ial distress screening in the Breast Center at Smilow Cancer Hospital at Yale New Haven. Crosssectiona l study 88 breast oncology patients NCCN Distress Thermomete r The Problem List Descriptiv e analysis The new patients screened in surgical oncology reported higher average distress scores compare d to patients in medical oncology. A greater number of patients in medical oncology reported scores greater than 4 compare d to the new patients Theory based study. Appropr iate method. Quick data collectio n. Able to translate to other studies. Limited to the surgical breast oncology patients. This is a good, thorough study predicting psychologi cal distress. Nurse led psychosoci al screening is feasible. Proper psychosoci al screening is an important quality indicator of patientcentred care. MEASUREMENT OF STRESS IN THE ONCOLOGY POPULATION Author/ s Title Journal Date (yr/vol/ iss) Researc h Questio n Design & Metho d Population Sample Data Collection/ (Size, Type) Instrumen ts 14 Analysis Finding s Strengt hs Limitatio ns Conclusi on Implicati ons (Take home message) screen in surgery. Denters, M., Deuteko m, M., EssinkBot, M., Bossuyt, P., Fockens, P., Dekker, E. FIT falsepositives in colorecta l cancer screenin g experien ce psycholo gical distress up to 6 weeks after colonosc opy Supporti ve Care in Cancer, Volume 21, Issue 10 06/01/2 013 Explore the difference s in psycholog ical effects crosssectionall y after receipt of the invitation in all invites and longitudi nally in participan ts with a positive FIT result. Crosssectiona l study 3828 of average risk persons between the ages of 50 to 74 The Psychologica l Consequenc es Questionnai re Data was analysed by point and time. The primary analysis focused on the PCQ total score; additional analyses were done for the PCQ emotional , physical, and social subscores . Mean total, physical, and social PCQ scores had decrease d significan tly between the first question naire and the precolonosc opy one, but scores on the emotiona l subscale did not. In falsepositives, mean total, physical, and emotiona l PCQ Large sample size. Relatively low response rate among nonpartici pants, making it difficult to generalize scores. Bias cannot be excluded – people experienci ng high levels of stress were more likely to return the questionna ire. No other group for compariso n. A good study that reveals how testing can induce psychologi cal stress. There is difficulty in using questionn aires where participan ts do not readily answer if they feel the study does not apply to them. Studies that invite participan ts for test screening can cause psychologi cal distress in invitees. MEASUREMENT OF STRESS IN THE ONCOLOGY POPULATION Author/ s Title Journal (yr/vol/ iss) Date Researc h Questio n Design & Metho d Population Sample Data Collection/ (Size, Type) Instrumen ts 15 Analysis Finding s Strengt hs Limitatio ns Conclusi on Implicati ons (Take home message) scores decrease d significan tly, while in truepositives, a significan t decrease in mean emotiona l PCQ score was observed. Running head: MEASUREMENT OF STRESS IN THE ONCOLOGY POPULATION 16 Research Synthesis Operationally, the Distress Thermometer categorizes stress in 3 different levels. A level from 0 to 4 indicates stress being controlled, a 5 to 7 indicates experiencing stress levels that effect daily living, and a score of 8 to 10 indicates a high level of stress that requires medical attention. The Brief Symptom Inventory Scale is an 18-item questionnaire designed to examine distress in the last week through 3 subscales— somatization, anxiety, and depression (Grassi et al., 2013). Each item is rated on a Likert scale ranging from 0 (not at all) to 4 (extreme stress). A total distress score is derived by summing all items. Other tools used to measure stress include the Hospital Anxiety and Depression, Global Inventory Scale, etc. Regardless of the tool used, stress proves to be a subjective phenomenon and quantitatively measuring continues to be difficult. Studies in the review used different cutoff scores according to previous studies using the same tool. This makes standardizing significance of stress levels challenging. Using a standardized cutoff score for future studies can further support clinical significance and make it easier to compare scores. Most studies in the integrative review used a crosssectional study design. Populations include patients during hospital admissions and outpatient visits. The integrative review focused on cancer patient’s level of stress. The studies framework are appropriate. Further Research There are implications for further research associated with the integrative review. A potential research area include exploring how distal, cognitive, behavioral, and genetic risk factors affect stress levels during development. Can the incidence of stress be predicted by identifying biological predictors and markers? According to Strong et al. MEASUREMENT OF STRESS IN THE ONCOLOGY POPULATION 17 (2007), the population with the highest distress score within their study are female, having active disease, and younger than 65. Comparing stress levels with populations falling in different categories can highlight whether risk factors are significant in predicting high levels of stress. Another area of potential research include investigating the reliability of stress measurement tools. Most studies in the integrative literature review noted the need for reliability and validity testing of the established instruments. Comparing established stress measurement tools with full narratives can be a means of testing data. Summary The integrative review yielded common measurement tools such as the Distress Thermometer, Brief Symptom Inventory, HADS and GSI. The integrative review highlights the need for further research to support validity and reliability of established measurement tools. This brings up the question which tool is best for assessing stress. Properly determining the presence and level of stress, and the best frequency of assessment, is what these studies aimed to show. Regardless of the differing scores and tools, the all agree with the importance of psychological stress screening and its integration to a practice standard. MEASUREMENT OF STRESS IN THE ONCOLOGY POPULATION 18 References Bleiker, E., Pouwer, F., Ploeg, H., Leer, J., & Adèr, H. (2000). Psychological distress two years after diagnosis of breast cancer: Frequency and prediction. Patient Education and Counseling, 40(3), 209-217. De Haes, J., Van Knippenberg, F., & Nejit, J. (1990). Measuring psychological and physical distress in cancer patients: Structure and application of the Rotterdam Symptom Checklist.British Journal of Cancer, (62), 1034-1038. Denters, M., Deutekom, M., Essink-Bot, M., Bossuyt, P., Fockens, P., & Dekker, E. (2013). FIT false-positives in colorectal cancer screening experience psychological distress up to 6 weeks after colonoscopy. Supportive Care in Cancer, 21(10), 2809-2815. Grassi, L., Johansen, C., Annunziata, M., Capovilla, E., Costantini, A., Gritti, P., ... Bellani, M. (2013). Screening for distress in cancer patients. Cancer, 119(9), 1714-1721. Hoffman, B., Zevon, M., D'arrigo, M., & Cecchini, T. (2004). Screening for distress in cancer patients: The NCCN rapid-screening measure. Psycho-Oncology, (13), 792-799. Jacobsen, P., Donovan, K., Trask, P., Fleishman, S., Zabora, J., Baker, F., & Holland, J. (2005). Screening for psychologic distress in ambulatory cancer patients. Cancer, 103(7), 14941502. Keller, M., Sommerfeldt, S., Fischer, C., Knight, L., Riesbeck, M., Lowe, B., ... Lehnert, T. (2004). Recognition of distress and psychiatric morbidity in cancer patients: A multimethod approach. Annals of Oncology, 15(8), 1243-1249. MEASUREMENT OF STRESS IN THE ONCOLOGY POPULATION 19 Knobf, M., Major-Campos, M., Chagpar, A., Seigerman, A., & Mccorkle, R. (2014). Promoting quality breast cancer care: Psychosocial distress screening. Palliative and Supportive Care,12(1), 75-80. Kugaya, A., Akechi, T., Okuyama, T., Nakano, T., Mikami, I., Okamura, H., & Uchitomi, Y. (2000). Prevalence, predictive factors, and screening for psychologic distress in patients with newly diagnosed head and neck cancer. Cancer, 88(12), 2817-2823. Özalp, E., Cankurtaran, E., Soygür, H., Geyik, P., & Jacobsen, P. (2006). Screening for psychological distress in Turkish cancer patients. Psycho-Oncology, 16(4), 304-311. Strong, V., Waters, R., Hibberd, C., Rush, R., Cargill, A., Storey, D., ... Sharpe, M. (2007). Emotional distress in cancer patients: The Edinburgh Cancer Centre symptom study. British Journal of Cancer, 96, 868-874.