Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
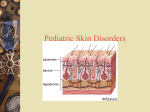
LECTURE DELIVERED AT THE NPMCN, FACULTY OF FAMILY MEDICINE WORKSHOP ON COMMON SKIN DISORDERS , AT FMC, BIDA,NIGER STATE. BY; DR. M D. PEMI(MB.,BS., FWACP). CONSULTANT FAMILY PHYSICIAN, Learning Objectives Introduction Epidemiology Pathogenesis/Predisposing factors Symptoms and Signs Clinical/Laboratory diagnosis Differential diagnosis Management, Conclusion,Bibliography To let us know that bacteria skin diseases are common. We should be able to recognize and discuss differential diagnosis of each. To highlight predisposing factors for each. To highlight treatment modalities for each To highlight prevention/complication The skin has normal flora just like any other part of the body The flora is composed of aerobic cocci, aerobic and anaerobic coryneform bacteria etc Major function of skin flora is to prevent skin infections by Providing ecological competition for pathogenic microorganism By hydrolizing lipids of sebum to produce free fatty acids which are toxic to many bacteria The ecology of particular areas of the skin is determined by the availability of moisture, presence of sebaceous lipids, and gaseous environment The process of infection involves the interaction between two organisms-the host and the invader The clinical changes depends on the organisms, its virulence, and patient’s immunity Acute bacteria infections generally produce some or all of the classical features of acute inflammation These cardinal signs includes; erythema(redness), swelling/oedema, heat/warmth, pain/discomfort Bacteria skin infections are very common in Family Medicine Practice settings Cellulitis, impetigo and folliculitis are the most common bacteria skin infections seen by the Family Physicians. The percentage office visits for cellulitis was 3.2percent in a cohort of 320,000 health plan member. The skin has normal flora whose function is to provide Introduction- folliculitis is infection of the hair follicles. Classification is by the depth of involvement of the hair follicles which could be superficial or deep folliculitis. Hair follicle can become inflamed by physical injury, chemical irritation or infection that leads to folliculitis. A furuncle develops when the entire follicle and surrounding tissues are involved. The most common form is superficial folliculitis It could be multiple or single lesion and can appear on any skin bearing hair including head, neck, trunk,buttocks and extremities S. aureus is the most common infectious cause of folliculitis. However,commensal organisms like yeast can be seen in immunocompromised. Occasionally, gram negative folliculitis can be seen in acne vulgaris patients treated with long courses of antibiotics. The use of hot tubs and whirl pools has been classically associated with Pseudomonas folliculitis. Patients with atopic dermatitis are at increased risk because of higher rate of colonization with S. aureus. Shaving, plucking or waxing hair, use of topical corticosteroids, hot and humid weather, and diabetes mellitus are all predisposing factors The appearance of the lesions depends on the depth of follicular involvement. Lesions of superficial folliculitis(Bockhart’s impetigo) are small, 1-4mm pustules or crusted papules on an erythematous base Lesions of superficial folliculitis is usually tender or painless pustules that heals without scarring. Associated systemic symptoms is rare A deep folliculitis appears as large, tender, erythematous papules, often with a central pustule. The lesions may be pruritic and slighly tender. The lesions are painful and may scar. The diagnosis of bacterial folliculitis is usually based on clinical inspection. Gram stain and bacterial cultures can help to identify the causative organisms, especially in recurrent or treatment-resistant cases. The differential diagnosis includes other forms of folliculitis as well as acne vulgaris, rosacea, ,pseudofolliculitis barbae , and keratosis pilaris Superficial bacterial folliculitis can be treated with antibacterial washes that contain chlorhexidine or triclosan. Antibacterial ointments (bacitracin or mupirocin 2%) may also be used for 7–10 days for localized lesions. When staphylococcal folliculitis is widespread or recurrent, appropriate oral blactamase inhibitor antibiotics, macrolides and lincosamides (e.g clindamycin), flouroquinolones can be used. Despite emerging resistance patterns, treatment failure of bacterial folliculitis is uncommon. Chronic S. aureus carriage can be treated with mupirocin 2% ointment applied twice daily to the nares, axillae/groin and/or submammary area for 5 days. Pseudomonal folliculitis is associated with the use of whirlpools, hot tubs and, rarely, swimming pools. P. aeruginosa gains entry via hair follicles or breaks in the skin. The lesions arise 8–48 hours after exposure and resolve in 7–14 days. There are erythematous, papules and pustules that rarely scar, but may result in post inflammatory Hyperpigmentation . The lesions frequently occur in sites covered by bathing suits, and the face and neck are usually spared. Associated symptoms do not imply systemic spread of P. aeruginosa, These symptoms includes ; painful eyes, malaise, fever The diagnosis can be confirmed by isolation of P. aeruginosa, especially serotype O-11, from lesions. The differential diagnosis includes S. aureus folliculitis, insect bites, papular urticaria, Majocchi’s granuloma, eosinophilic folliculitis, miliaria and acne vulgaris. Treatment is generally not indicated in immunocompetent hosts as it is usually a self-limited process. Lesions usually resolves spontaneously within seven to ten days In the case of widespread eruptions, recurrences, immunosuppression or associated systemic symptoms, an oral fluoroquinolone and topical gentamicin can be used. By appropriate cleaning of whirlpool or hot tub. By maintaining appropriate chlorine levels Bromine/copper solutions are less common alternatives used. Hand washing is an important behaviour modification in the prevention of spread. Sports participants should shower regularly and all personal clothing should not be shared Daily application of 6.25% aluminium chloride hexahydrate in completely anhydrous ethyl alcohol was reported to be very effective in treatment for chronic folliculitis of unspecified type, except for scalp lesions. A furuncle is a tender, erythematous, firm or fluctuant mass of walled-off purulent material arising from the hair follicles. It is commonly known as boil or abscess. Carbuncles are an aggregate of infected hair follicles that form broad swollen, erythematous, deep and painful masses that usually open and drain through multiple tracts. Furuncles tend to occur in adolescents and young adults. S. aureus is the most common causative organism, though recurrent furuncles in the anogenital region can be secondary to anaerobic bacteria. Five percent of cutaneous abscesses are sterile, caused by a foreign body reaction (e.g. ruptured cyst Predisposing factors include chronic S. aureus carriage, Diabetes mellitus, obesity, poor hygiene, Immunodeficiency states, such as in chronic granulomatous disease and Job syndrome. The most common locations are the face, neck, axillae, buttocks, thighs and perineum. Sites prone to friction or minor trauma, such as the area under a belt, are distinctly susceptible. Furuncles usually begin as a hard, tender, red nodule that enlarges and becomes painful and fluctuant; rupture results in decreased pain. Abscesses are localized collections of pus that are usually inflamed. They can arise in any organ or structure, as well as at any cutaneous site. Furuncles (boils) are acute, inflammatory abscesses of hair follicles and surrounding tissue, and, as such, occur only in hairbearing skin. Systemic symptoms are usually absent in furunculosis Carbuncles are slow to heal and scar formation is inevitable Carbuncles usually occur in area of thicker skin eg nape of neck, back and thigh Biopsy specimens reveal a dense neutrophilic infiltrate in the subcutaneous tissue. Furuncles are characterized by an acute, suppurative reaction involving the follicle below the infundibulum, as well as perifollicular necrosis with fibrinoid debris Diagnosis is based primarily on clinical appearance. Gram stains and cultures from the lesion support the diagnosis. Extensive furuncles and carbuncles can be associated with an increased leukocyte count. A ruptured epidermoid or pilar cyst, hidradenitis suppurativa (‘acne inversa’) and cystic acne should be considered in the differential diagnosis. For simple furuncles oral antibiotics such as cloxacillin, first generation cephalosporins are indicated. Warm compress may promote maturation ,drainage and resolution of symptoms Fluctuant lesions require incision and drainage . Systemic antibiotics should be used in four instances: (1) furuncles around the nose, within the nares or in the external auditory canal; (2) large and recurrent lesions; (3) lesions with surrounding cellulitis; and (4) lesions not responding to local care . INTRODUCTION Erysipelas is primarily an infection of the dermis with significant lymphatic involvement. It has a distinctive clinical presentation and is most often caused by Str. pyogenes (group A streptococci). Erysipelas can be traced back to the Middle Ages. It was thought to be caused by ingestion of the fungus Claviceps purpurea, which produces ergot alkaloids and is found in contaminated rye. The eponymous distinction refers to St Anthony, an Egyptian monk and healer, who was believed to be the only person able to provide relief from the symptoms of erysipelas Erysipelas is a disease of the very young, the aged, the debilitated, and those with lymphedema or chronic cutaneous ulcers. Women outnumber men, except for very young patients, where boys are more commonly affected. There is an increased frequency during the summer months and most cases are isolated. Most cases of erysipelas are caused by infection with group A streptococci and less often by group G, B, C or D. S. aureus, Pneumococcus species, Klebsiella pneumoniae, Yersinia enterocolitica, and Haemophilus influenzae type b have been known to cause an erysipelas-like infection The classic lesion of erysipelas, with its welldefined margins, involves the face. Nowadays, however, the lower extremity is the most common location. After an incubation period of 2 to 5 days, there is an abrupt onset of fever, chills, malaise and nausea. A few hours to a day later, a small plaque of erythema develops that progressively spreads The area is clearly demarcated from uninvolved tissue, hot, tense and indurated with non-pitting edema. The affected area is painful to palpation and may burn. Regional lymphadenopathy is normally present, with or without lymphatic streaking. Pustules, vesicles, bullae and small areas of hemorrhagic necrosis may also form. Complications of erysipelas are rare and usually occur in patients with underlying disease. When the infection resolves,desquamation and postinflammatory pigmentary changes may occur. Biopsy specimens reveal diffuse edema of the dermis and a dermal neutrophilic infiltrate. Involvement of the lymph vessels (dilation), dermal foci of suppurative necrosis, And a dermal–epidermal separation are commonly seen. There is no primary necrotizing vasculitis, thrombosis or leukocytoclasis Diagnosis is based primarily on clinical findings. Routine laboratory evaluation will show an elevated leukocyte count with a left shift. Blood cultures are positive in only about 5% of cases. Swabs from local ports of entry, pustules or bullae, the throat, and the nares may be helpful. Culture of skin biopsy specimens and the injection-re-aspiration method yield poor results, especially in immunocompetent hosts . Anti- DNase B and ASO titers are good indicators of streptococcal infections. Direct immunofluorescence and latex agglutination tests can be used to detect streptococci within skin specimens. . cellulitis and other soft tissue infections (e.g. erysipeloid, necrotizing fasciitis) as well as inflammatory causes of ‘pseudocellulitis’ (e.g. Sweet’s syndrome, contact dermatitis) A 10–14-day course of penicillin is the treatment of choice for erysipelas caused by streptococci. Although macrolides such as erythromycin may be used in penicillin-allergic patients, there has been an increase in macrolide resistance among certain strains of Str. pyogenes. Hospital admission and intravenous or intramuscular antibiotics should be reserved for children and debilitated patients. INTRODUCTION Cellulitis is an infection of the deep dermis and subcutaneous tissue caused most commonly by Str. pyogenes and S. aureus Cellulitis in immunocompetent adults is most often caused by Str. pyogenes or S. aureus. The majority of cellulitis in childhood is caused by S. aureus, and less commonly by H. influenzae (even less so since the introduction of the vaccine). A mixture of Gram-positive cocci and Gramnegative aerobes and anaerobes is associated with cellulitis surrounding diabetic ulcers and decubitus ulcers. Bacteria may gain access to the dermis via an external or a hematogenous route. Usually, in immunocompetent patients, a break in the skin barrier is responsible In immunocompromised patients, a blood borne route is most common. Lymphedema, alcoholism, diabetes mellitus, intravenous drug abuse, and peripheral vascular disease all predispose to cellulitis. Recurrent bouts of cellulitis may be caused by damage to the lymphatic system (e.g. previous lymph node dissection, saphenous vein harvest or prior episode of acute cellulitis) Cellulitis is often preceded by systemic symptoms, such as fever, chills and malaise. The affected area displays all four of the cardinal signs of inflammation: rubor (erythema), calor (warmth), dolor (pain), and tumor (swelling). The lesion usually has ill-defined, nonpalpable borders. In severe infections, vesicles, bullae, pustules or necrotic tissue may be present. . Ascending lymphangitis and regional lymph node involvement may occur. Children usually have cellulitis of the head and neck region, whereas in adults the extremities are most often affected In intravenous drug abusers, the upper extremities are often involved. Complications are rare, but include acute glomerulonephritis (if caused by a nephritogenic strain of streptococci), lymphadenitis and subacute bacterial endocarditis. Damage to lymphatic vessels can lead to recurrent cellulitis. A mild or moderate inflammatory infiltrate composed mostly of lymphocytes and neutrophils can be seen throughout the dermis, occasionally extending into the subcutaneous fat. There is also edema and dilation of lymphatics and small blood vessels. With special stains, the causative organism may be identified. Subepidermal bullae may be seen in cases of severe dermal edema The diagnosis of cellulitis is usually clinical . The leukocyte count is usually normal or only slightly elevated. Blood cultures are almost always negative in immunocompetent hosts. An important exception is H. influenzae cellulitis, where there is usually an increased leukocyte count with a left shift and positive blood cultures. In children and immunocompromised patients, atypical organisms are more common, and needle aspiration and skin biopsy may be appropriate The differential diagnosis of lower extremity cellulitis includes deep vein thrombosis and other inflammatory diseases, such as stasis dermatitis, superficial thrombophlebitis, and panniculitis (especially lipodermatosclerosis). While superficial thrombophlebitis often presents with redness and tenderness, the absence of a fever and the presence of a palpable cord aid in the diagnosis. Lipodermatosclerosis, misdiagnosed as cellulitis, often leads to unnecessary hospitalizations. In most cases of cellulitis, treatment should be targeted against Str. pyogenes and S. aureus. Mild cases require a 10-day course of an oral antibiotic that has good Gram-positive coverage. Hospitalization and parenteral antibiotics should be reserved for patients who are seriously ill and those who have facial cellulitis. Diabetic or decubitus ulcers complicated by cellulitis require broad-spectrum coverage (e.g. piperacillin/tazobactam or, in penicillin-allergic patients, metronidazole plus ciprofloxacin). Immobilization and elevation, as well as the application of wet dressings to areas with bullae or exudate, are recommended. If signs and symptoms do not improve after 24–36 hours of treatment, cultures and sensitivities should be obtained and antibiotics adjusted accordingly. NSAIDs may mask the signs and symptoms of deeper necrotizing infections and should be avoided when treating cellulitis. INTRODUCTION: Impetigo is a common, highly contagious, superficial skin infection that primarily affects children. The condition presents in both non-bullous and bullous forms . The primary pathogens in non-bullous and bullous impetigo are Staphylococcus aureus and, less commonly, group A b-hemolytic Streptococcus (Streptococcus pyogenes). Worldwide, impetigo is the most common bacterial skin infection in children. It is extremely contagious, spreading rapidly via direct person to - person contact, though contact with fomites has also been implicated in spread of the disease. Peak incidence is in summer and fall months. Often, adult acquire the infection through close contact with infected children. . Predisposing factors include warm temperature, high humidity, poor hygiene, an atopic diathesis and skin trauma. Nasal, axillary, pharyngeal and/or perineal S. aureus colonization imparts an increased risk for developing impetigo Non-bullous impetigo Non-bullous impetigo (or crusted impetigo) is usually caused by S. aureus and, on occasion, Str. pyogenes. Infection occurs at minor sites of trauma (e.g. chickenpox, insect bite, abrasion, laceration, burn). Trauma exposes cutaneous proteins which allow the bacteria to adhere, invade and establish infection Bullous impetigo The etiologic agent of bullous impetigo, S. aureus, elaborates several exfoliative toxins and bullous impetigo is considered a localized form of staphylococcal scalded skin syndrome . In both diseases, blister formation is mediated by exfoliative toxin binding to the desmosomal protein desmoglein 1 and cleaving its extracellular domain, thus leading to acantholysis within the epidermal granular layer. In contrast to non-bullous impetigo, lesions can occur on intact skin . Although the differential diagnosis for nonbullous and bullous impetigo is extensive, the history , physical examination and ancillary tests can often establish the diagnosis. Primary treatment involves local wound care, including cleansing , removal of crusts, and application of wet dressings. For healthy patients with a few, isolated superficial lesions and no systemic symptoms , either mupirocin 2% ointment or fusidic acid cream or ointment can be prescribed. For patients with limited disease, there is evidence that these topical medications are at least equally (if not more) effective than oral antibiotics Although exotoxin-producing S. aureus is more sensitive to penicillin, meta-analysis of treatment trials found that traditional penicillin was inferior to erythromycin and penicillinase-resistant penicillins for the treatment of impetigo. In non-complex cases and in communities with low levels of resistance, macrolides are usually effective. Intravenous therapy should be considered for more severe or widespread infections, as well as infections in compromised hosts Acne Keloidalis (Folliculitis keloidalis) is a chronic, inflammatory process involving the hair follicles of the nape of the neck and leading to hypertrophic scarring in papules and plaques. It occurs in males after puberty and is most frequent between the ages of 14 and 25 years, especially in black males Acne keloidalis occurs when hairs on the back of the head and neck grow into the skin, become inflamed, and cause scar tissue. It is more common in people with stiff or curly hair and those with darker skin. • It is associated with papules and nodules on the nape of the neck. A study from Nigeria reported that 9.4% of all patients attending dermatology outpatients had acne keloidalis . Many patients have, or have had, significant acne, and a patient with previous hidradenitis has been reported . No specific organism can be isolated in most cases , although S. aureus is occassionaly isolated Although friction from the collar is often incriminated, the evidence is unconvincing . An association between frequent haircuts (<4 weeks) in high school boys has been documented Associated keloids in other sites seem not to have been reported, and the process is regarded as hypertrophic scarring rather than true keloid. The most frequent histological findings include chronic perifollicular inflammation, disappearance of sebaceous glands, destroyed follicles, lamellar fibroplasia and acute inflammation around degenerating follicular components. Serial sections may show a foreign-body reaction to hair and follicular remnants. The pathological findings seen in early lesions, perilesional skin and clinically normal skin, suggest that follicular antigens such as Demodex, bacteria or other skin flora, stimulate an inflammatory reaction which then destroys the sebaceous glands and follicles. The end result is scarring . Follicular papules or pustules, often in irregularly linear groups, develop on the nape of the neck just below the hair line. Less often, they extend upwards into the scalp, and the name acne keloidalis is thus preferred to acne keloidalis nuchae The early inflammatory stage may be inconspicuous, and the patient may first be aware of the hard, keloidal papules that follow the folliculitis. The papules may remain discrete, or may fuse into horizontal bands or irregular plaques. In other cases, the inflammatory changes are persistent and troublesome, with undermined abscesses and discharging sinuses The condition is extremely chronic and new lesions may continue to form at intervals for years. Bacterial infection should be treated if present, and antiseptics may help to reduce further or secondary infection. No evidence-based reviews of therapy options are available. Avoidance of closely shaven hair on the back of the scalp may be advised. Intralesional or topical potent steroids may reduce scarring and inflammation. Oral steroids prescribed for another condition helped, but long-term treatment is unlikely to be justified In general, medical treatment is disappointing, and in troublesome cases the affected area may be excised and grafted, or excised and allowed to heal by secondary intention. Laser therapy followed by secondary intention healing has been helpful. Surgery followed by radiotherapy has also been advocated previously. PFB is a Chronic Inflammatory disorder of the hair-bearing skin. PFB occurs as a consequence of hair removal when tightly coiled hair shafts, after being shaved or plucked, reenter the epidermis or penetrate the hair follicle wall causing inflammation Sometimes when men shave, the hair pierces the epidermis causing irritation and sensitivity to the hair follicle whose wall is inflamed after the piercing. Beard hair, when shaved closely, causes inflammation, papules and nodules Keratosis pilaris Perioral dermatitis Angiofibromas Acne keloidalis nuchae Folliculitis Hidradentis suppurativa Basic skin care No washing, scrubbing or picking Cleanse with a gentle soap, may contain salicylic acid, glycolic acid or benzoyl peroxide If moisturize use noncomedogenic agent Based on skin type, choose appropriate vehicle for topical treatments Oily (solutions, gels, pledgets) Combination (lotions) Dry (cream, ointment) Tretinoin (Retin A), Adapalene (Differin), Tazarotene (Tazorac) Excellent choice for comedomal acne Improves follicular desquamation and dyschromia Anti-inflammatory action (Differin best) Use at night over entire face, exposure to the sun increases irritation Results in six to eight weeks. May increase concentration over time Degraded by prolonged exposure to the sun and when used with benzoyl peroxide (Differin most photostable) Adverse affects Irritant potential (Tazorac most irritating, Differin least) Sun sensitivity Pustular eruption after 3-4 weeks Potential hyper/hypopigmentation in black and Asian patients Contraindicated in pregnancy Erythromycin, Clindamycin, Decrease P.acnes and percentage of free fatty acids Slow to act Resistance often develops over time Best used in combination with topical retinoids/benzoyl peroxide Rare cases of pseudomembranous colitis w/ topical clindamycin Bactericidal effect on P.acnes No evidence of resistance BP combined with a topical antibiotic may help decrease the presence of antibiotic resistant P. acnes Mild comedolytic action, decreases free fatty acids Adverse effects Irritation Bleaches clothing and hair Allergic contact dermatitis Dicarboxylic acid that is bacteriostatic against P.acnes and normalizes keratinization Most effective when used with other agents Side affects uncommon Use in caution in teens w/ dark complexions due to potential risk of hypopigmentation Primarily used for moderate to severe inflammatory acne Decreases P.acnes Reduces amount of free fatty acids Preferred agents: Tetracyclin, Doxycyclin, Minocyclin High rates of resistance to Erythromycin Oral contraceptive pills in females Increases production of sex hormone binding globulin leading to a decrease of circulating androgens Decreases ovarian androgen production Ortho tri-cyclen, Estrostep FDA approved for the treatment of acne Oral antiandrogens (spironolactone) can be useful Oral corticosteroids, short course for patients with severe inflammatory disease Systemic retinoid used for nodulo-cystic acne Most effective treatment with remission in 60% after single course (15-24 weeks) Reduces sebum production Normalizes follicular keratinization Decreases inflammation Baseline CBC, LFT’s, cholesterol, triglycerides, urinalysis, pregnancy test. Repeat monthly Post pubertal females must be on contraception and have two sequential negative pregnancy tests before starting Adverse effects Teratogenic (facial dysmorphism, abnormalities of brain, eye, ear, CV system, thymus) and retinoid embryopathy can occur with single exposure during gestation Drying/chapping of skin and mucous membranes Myalgias/arthralgias Photosensitivity GI effect: transaminitis, lipid abnormalities, pancreatitis Hematological: leucopenia, elevated platelets and ESR Neurological: pseudo tumor cerebri Renal: proteinuria, hematuria Mood disorders, depression, suicidal ideations and suicides Comedome May be helpful if comedomes are resistant to other treatments Chemical removal peels Little evidence supporting efficacy Intralesional Used for large inflammatory nodules/cysts Can be associated with local atrophy Topical steroids tree oil One clinical trial documented effectiveness Majority of bacterial skin infection are caused by Staphylococcus and Streptococcus species. Antibiotics are used emperically with consideration for resistance pattern Gram negative coverage is indicated in children under 3yrs and patient with diabetes or immunocompromised Stulberg DL, Penrod MA, Blatiny RA. Common bacterial skin conditions. Am Fam Phy 2002: 66(1);119-125. Salami T, Omeife H, Samuel S. Prevalence of acne keloidalis nuchae in Nigerians. Int J Dermatol 2007; 46: 482. George AO, Akanji AO, Nduka EU et al. Clinical, biochemical and morphologic features of acne keloidalis in a black population. Int J Dermatol 1993; 32: 714–6. Khumalo NP, Jessop S, Gumedze J et al. Hairdressing is associated with scalp disease in African schoolchildren. Br J Dermatol 2007; 157: 106–10. Sperling L, Homoky C, Pratt L et al. Acne keloidalis is a form of primary scarring alopecia. Arch Dermatol 2000; 136: 479–84. Shah GK. Efficacy of diode laser for treating acne keloidalis nuchae. Indian J Dermatol Vernereol Leprol 2005; 71: 31–4. Daum RS. Skin and soft-tissue infections caused by methicillin-resistant Staphylococcus aureus. N Engl J Med. 2007;357:380–90. Zetola N, Francis JS, Nuermberger EL, Bishai WR. Community-acquired meticillin-resistant Staphylococcus aureus: an emerging threat. Lancet Infect Dis. 2005;5:275–86. Lyon M, Doehring MC. Blistering distal dactylitis: a case series in children under nine months of age. J Emerg Med. 2004;26:421–3 Ladhani S, Evans R. Staphylococcal scalded skin syndrome. Arch Dis Child. 1996;78:85– 8Agerson AN, Wilkins EG. Streptococcal toxic shock syndrome after breast reconstruction. Ann Plast Surg. 2005;54:553–6 •O’Loughlin RE, Roberson A, Cieslak PR, et al.;Active Bacterial Core Surveillance Team. The epidemiology of invasive group A streptococcal infection and potential vaccine implications: United States, 2000–2004. Clin Infect Dis. 2007;45:853–62.. Pappas G, Akritidis N, Bosilkovski M, Tsianos E. Brucellosis. N Engl J Med. 2005;352:2325– 36. Staquet P, Lemee L, Verdier E, et al. Detection of Neisseria meningitidis DNA from skin lesion biopsy using real-time PCR: usefulness in the aetiological diagnosis of purpura fulminans. Intensive Care Med. 2007;33:1168–72. Vignes S, Dupuy A. Recurrence of lymphoedema-associated cellulitis (erysipelas) under prophylactic antibiotherapy: a retrospective cohort study. J Eur Acad Dermatol Venereol 2006; 20: 818– 22. Koster JB, Kullberg BJ, van der Meer JWM. Recurrent erysipelas despite antibiotic prophylaxis: an analysis from case studies. Neth J Med 2007; 65: 89–94. THANK YOU FOR YOUR ATTENTION