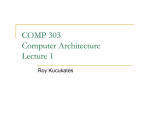
Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
d 2.00 • US $ 2.00 • CAN $ 3.00 Biomedical Therapy J o urnal o f Volume 1, Number 2 ) 2007 Integrating Homeopathy and Conventional Medicine Detoxification and Drainage • Functiotropic and Organotropic Therapy • Are You Getting the Patients You Deserve? ) Contents I n Fo c u s Management of Chronic Toxin Accumulation . . . . . . . . . . . . . 4 W h a t E l s e I s N e w ? . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 8 Practical Protocols Detoxification and Drainage . . . . . . . . . . . . . . . . . . . . . . . . . . 10 Re s e a r c h H i g h l i g h t s Obesity’s Helper in Triggering Diabetes . . . . . . . . . . . . . . . . .13 Around the Globe Spain: Homotoxicology in “Flamenco Country” . . . . . . . . . . .14 Around the Globe New E-learning Course on Homotoxicology . . . . . . . . . . . . . . 15 Re f r e s h Yo u r H o m o t ox i c o l o g y Synergy Between Functiotropic and Organotropic Therapy . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1 6 M a r ke t i n g Yo u r P r a c t i c e Marketing to Target Groups – Are You Getting the Patients You Deserve? . . . . . . . . . . . . . . .18 Specialized Applications Detoxification of Patients in the Dedifferentiation Phase . . . . . . . . . . . . . . . . . . . . . . . .20 Making of ... Manufacturing Liquid Medications: How Do Those Drops Get Into the Bottle? . . . . . . . . . . . . . . .22 Cover photograph © Titus Lacoste/Riser/Getty Images ) 2 C r o s s w o r d P u z z l e . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .24 Published by/Verlegt durch: International Academy for Homotoxicology GmbH, Bahnackerstraße 16, 76532 Baden-Baden, Germany, e-mail: [email protected] Editor in charge/verantwortlicher Redakteur: Dr. Alta A. Smit Print/Druck: Konkordia GmbH, Eisenbahnstraße 31, 77815 Bühl, Germany © 2007 International Academy for Homotoxicology GmbH, Baden-Baden, Germany ) Detoxification Is Finally Getting a Hearing Dr. Alta A. Smit D etoxification and drainage are one of the pillars of antihomotoxic treatment. Detox medications are administered routinely by practitioners of homotoxicology, but in other branches of medicine, toxin accumulation (except in the form of drug overdose) is not always seen as a problem until it becomes lifethreatening. Because chronic intoxication is insidious and damage on the molecular level occurs over years, the role of chronic intoxication has been largely ignored. As the introduction of new substances into the environment increases and as the proponents of global warming theory are finally getting a hearing, we see increasing awareness of the effects human beings may have on the planet and themselves. The picture that nature reflects back at us can be sobering, as we see from the banning of DDT after the publication of Rachel Carson’s Silent Spring.1 Now evidence of the chronic effects of toxins is mounting in reputable journals: Science has published observations of genetic damage that is seen only in the next generation, The New Scientist reported on the effects of persistent organic pesticides (see summary on page 13 of this journal), and many articles have appeared on endocrine disruption and the genetic effects of many toxins.2-4 Data released at a conference in Edinburgh on the 10th of September this year confirmed that both passive and active smokers suffer fewer heart attacks when smoking is banned in public places, confirming that legislation can indeed have an effect on environmental safety.5 However, till we humans can maintain a balance between our industry and our own health, the only thing patients and practitioners can do is to support the elimination of toxins from the body. That is why this issue is devoted to this very important topic. Our focus article examines the effects of chronic intoxication, while practitioners share their experiences with detoxification in various types of patients. In our new column Marketing Your Practice, you will learn about target-group oriented marketing, and the Making of… series will introduce you to the process of manufacturing liquid medications. Last but not least, Around the globe will take you on a journey to Spain. Alta A. Smit, MD References: 1. Carson R. Silent Spring. Boston, MA: Houghton Mifflin, 1962. 2. Anway MD, Cupp AS, Uzumcu M, Skinner MK. Epigenetic transgenera tional actions of endocrine disrup tors and male fertility. Science 2005; 308(5727):1466-1469. 3. Welshons WV, Thayer KA, Judy BM, Taylor JA, Curran EM, vom Saal FS. Large effects from small exposures. I. Mechanisms for endocrine-disrupting chemicals with estrogenic activity. Environ Health Perspect 2003;111(8):994-1006. Journal of Biomedical Therapy 2007 ) Vol. 1, No. 2 4. Hartwig A, Asmuss M, Ehleben I, Herzer U, Kostelac D, Pelzer A, Schwerdtle T, Bürkle A. Interference by toxic metal ions with DNA repair processes and cell cycle control: molecular mechanisms. Environ Health Perspect 2002;110(Suppl 5):797-799. 5. Cramb A. Scottish smoking ban cuts heart attacks. Telegraph. 12 September, 2007. http://www.telegraph.co.uk/ news/main.jhtml?xml=/news/2007/ 09/11/nsmoking111.xml. Accessed November 19, 2007. ) 3 ) I n Fo c u s Management of Chronic Toxin Accumulation ) 4 By Luigi Piroli, MD Introduction in areas where the chemicals were never used. Bioaccumulation of these compounds causes disease in living beings. In humans, the immune, endocrine, and neurological systems are the most affected.3 Xenobiotics and/or individual inability to deal with them seem to be at the root of many modern diseases, including Parkinson’s disease, chro nic fatigue syndrome, and cancer.4-6 Modern medicine is quite successful in diagnosing and treating acute intoxications as medical emergencies (heavy metal accumulation, drug poisoning, etc.) as well as various sub-acute, symptomatic toxicities (chemicals, drugs, and/or other xe nobiotics), but only if laboratory evidence of intoxication is found. In recent years, however, the burden of chronic toxin accumulation has become clearer and more disturbing as the effects of minute doses of toxins over time and effects on subsequent generations become evident.1,2 Individual tolerance of or susceptibility to specific toxins may vary. A biological system’s tolerance of a toxin is partly genetic and partly acquired on the basis of enzymatic induction and/or inhibitions, the degree of functionality of the target organ, and functional reserve capacity of specific organ systems. The clinical manifestations of biological effects of toxins depend not only on the physical and chemical properties of the toxin itself but also on the duration and route of exposure, the toxin’s mechanism of action, and (obviously) on individual susceptibility. Modern laboratories can now test for individual susceptibility. Chemical compounds, which comprise the bulk of environmental toxins, have spread throughout the world via the ground water, rain, and winds, and are now present even Managing chronic toxin accumulation As is clear from the above, in assessing a patient with toxicity, multiple factors need to be taken into account, including not only the total toxin load but also the individual patient’s response. Two patients exposed to the same amount of the same toxin may respond differently. Individual differences are apparent not only in how patients deal with toxins (primarily differences in metabolism or biotransformation) but also in how the toxins are stored and eliminated. Rather than assessing total exposure, therefore, it is more important to assess what each patient is doing with the toxin load. In homotoxicology, this is assessed indirectly on the Disease Evolution Table, where we measure the pa tient’s regulatory ability in terms of disturbance in homeostasis.7 Journal of Biomedical Therapy 2007 ) Vol. 1, No. 2 Biotransformation or metabolization of toxins Substances may undergo processes that make them water-soluble and thus more readily excreted, or they may undergo bioinactivation, which reduces the toxicity of the end product. Biotransformation takes place primarily in the liver and the intestinal tract and to a lesser extent in the skin, kidneys, and other organs. Phase I and II reactions These have been described elsewhere and will not be discussed in depth here.8 Suffice it to say that phase I involves oxygenation; in phase II, conjugation adds a watersoluble group to the reactive site formed in phase I. Thus detoxification is not a single process but a number of processes involved in the biotransfomation of xenobiotics. Every step depends on several cofactors such as vitamins and minerals. Because phase I enzymes are mixed-function oxidases, a number of free radicals are formed during the detoxification process, so it is important to provide adequate nutritional and antioxidant support for the patient. ) I n Fo c u s Phase III – The antiporter system This system is active primarily in the intestines. Paradoxically, the intestinal mucosa functions both as a barrier and as a filter. As the first point of contact with drugs and food as well as environmental xenobiotics, the mucosa has developed a complex set of defense mechanisms, one of which is the so-called antiporter system. In this process, xenobiotics are actively pumped out of the cell to reduce their intracellular concentrations. This phenomenon was first observed in cancer cells, which actively eliminate chemotherapy agents. Antiporter activity in the intestinal wall seems to be co-regulated with the phase I CYP3A4 enzyme.9 It is therefore important to use products such as Mucosa compositum to support the intestinal wall during any detoxification and drainage treatment. Storage and elimination of toxins Release of toxins from their reservoirs depends on toxicokinetics (to xins are cleared “upstream” first, i.e., out of the blood stream), on whether the reservoir is a rapid or slow exchange system, and on whether the chronobiology of the tissue (e.g., the matrix) is intact.8 Adipose tissue, a major reservoir of fat-soluble toxins, is a slow exchange system, as is bone. Consequently, obese patients may have a higher toxic load. When one or more factors will affect the release of toxins, drainage should be stimulated long enough to ensure clearance of the tissue in question (see below). A patient’s total toxic load thus depends on the exposure and storage on the one hand and on biotransformation and elimination on the other. Measurement of toxin accumulation and the ability to biotransform toxins One of the major obstacles facing a physician is how to assess each patient’s current toxic load and exposure risk. It is well known in biological medicine that individuals respond differently to the same exposure – a fact that makes the physician’s task even more daunting. Since intoxication may produce no symptoms, researchers are now hunting for biomarkers to aid in assessing toxin accumulation and the effect of the toxin on individuals and especially in identifying individuals at risk for the effects of certain exposures.10 For practical purposes, testing methods can be divided into four groups: 1. Testing for the presence of toxins 2. Assessing the body’s ability to biotransform toxins and to protect itself from their effects 3. Assessing individualized risk 4. Assessing toxicity indirectly, through symptoms 1. Testing for the presence of toxins In recent years, more sophisticated biomarkers have supplanted the commonly used fat aspiration biopsy. Fat biopsy is an invasive procedure that ultimately provides information only on the accumulation of fat-soluble toxins; it says nothing about how the toxin interacts with and impacts the tissue. Biomarkers of toxin exposure may be either exogenous substances or their metabolites or products of the interaction of the xenobiotics with target molecules or cells within a compartment of the body, e.g., adducts with DNA Journal of Biomedical Therapy 2007 ) Vol. 1, No. 2 or red blood cells. Many of the assays are highly sophisticated and beyond the scope of this article, since they are not routinely used in practice but rather for research purposes and epidemiological studies of exposures.10 Testing for toxic metals can also be done via hair analysis or urinary testing after provocation with DMSA, as these compounds are largely undetected by normal laboratory analyses. Serum testing, however, may be used for lead, mercury, aluminum, and cadmium.9 2. Assessing the body’s ability to biotransform toxins and to protect itself from their effects 2.1 Urinary metabolic profile Biomarkers commonly used in practice include the so-called urinary organic acids. Originally used to detect inborn errors of metabolism, these tests now are a useful tool in the assessment of chronic diseases. Organic profiling can be used not only to detect biomarkers of toxicity but also to assess central energy pathway intermediates, carbohydrate metabolism, specific vitamin deficiency indicators, neurotransmitter metabolism, and the products of the intestinal flora. Where available, it offers a comprehensive way to assess the patient’s individual response from a genetic and environmental perspective and indicates which cofactors should be replaced to ensure optimum detoxification.11 Direct markers of toxicity include glucarate, a by-product of phase II detoxification. Decreased glucarate indicates reduced overall hepatic function, whereas elevated glucarate indicates enzyme induction. For example, glucarate is elevated in pa tients exposed to pesticides. Elevat ed orotate is a sensitive test of both ammonia build-up and arginine ) 5 ) I n Fo c u s availability. 2-methylhippurate, a metabolite of the common solvent xylene, is used to monitor xylene exposure; pyroglutamate measures glutathione metabolism and sulfate measures sulfatation pathways. When the sulfate-creatinine ratio is low, the sulfur containing phase II pathways need replenishment (glutathione, cysteine, taurine). 2.2 Challenge testing Standard liver and kidney function tests reveal only pathologies, not metabolic integrity. In contrast, challenge tests may measure not merely liver integrity, for example, but the function of all organs involved in metabolizing the substance in question, such as the kidneys and P450 in the skin as well. The most common of these probe tests is the caffeine clearance test, which assesses the integrity of CYP1A2 activity. In this challenge test, a specified amount of caffeine is ingested, after which two or three saliva samples are measured at specific times. Because caffeine is almost completely absorbed in the intestine, its clearance rate reflects the metabolic activity of the P450 enzymes. Other probes are available for specific P450 enzymes, e.g., erythromycin (breath test) to measure CYP3A4 activity. ) 6 3. Measuring individual susceptibility There is increasing interest in the role human genome variations play in modifying the effect of environmental health hazards, rendering some individuals or groups more susceptible to post-exposure development of disease.12 More than 99 percent of human DNA is identical in all individuals, yet the less than one percent of DNA that differs from person to person ensures that no two humans (other than identical twins) are exactly alike. To create all the cells and tissues in the body, DNA must replicate itself billions and trillions of times, creating numerous opportunities for errors. The most common error is called a single nucleotide polymorphism or SNP (pronounced “snip”), in which a single nucleotide in a gene is changed. SNPs in a gene may increase – or more commonly, decrease – the activity of detoxifying enzymes, either of which can be harmful. For instance, CYP1B1 is responsible for 4-hydroxylation of estrogen and activation of polycyclic aromatic hydrocarbons (which occur, for example, in cigarette smoke, car exhaust, and charbroiled foods). Thus activation of this enzyme produces oxidative stress and 4-hydroxyestrogens, which cause DNA damage in breast tissue. Other SNPs have been associated with lower 2:16-hydroxy estrone ratios and increased risk of breast cancer, especially with concomitant xenobiotics exposure and accumulation. Test panels for SNPs involved in detoxification are now available through selected laboratories. Genetic testing, once of only theoretical interest for the future, is increasingly becoming part of our quest to individualize patient treatment and to assess risk. Of course this gives new meaning to the famous words of Claude Bernard, who said that the bacterium is nothing, but the terrain is everything! Tests for SNPs related to detoxification enzymes assess the terrain the toxin will encounter, thus the predisposition of the patient to be affected by the toxin. 4. Indirect assessment through symptoms This method, although the least specific, offers an inexpensive, practical means of following patients Journal of Biomedical Therapy 2007 ) Vol. 1, No. 2 with toxicity. Here, the constellation and severity of symptoms play a role, so a simple questionnaire* is administered and then repeated every time the patient comes for a follow-up. In effect, the patient serves as his or her own control from baseline. Movement of symptoms can also be used as a diagnostic predictor, as symptoms tend to move from deeper to more superficial organs and from the deposition phase to the excretion phase as toxins are eliminated and the patient improves. The detoxification questionnaire is a self-administered test that includes questions about all the major toxicity symptoms. Practical management of bioaccumulated toxins After a careful history and a thorough medical examination, the patient should be classified according * To obtain a copy of the Detox questionnaire, please contact your local Heel distributor. ) I n Fo c u s to the severity of his or her illness, using either the Disease Evolution Table or a questionnaire. If available, one or more specialized tests may be added. Patients with high toxic loads (either a point count of over 100 on the questionnaire or multiple markers in urinary metabolic testing) and patients with specific health problems (e.g., cancer, obesity, prior drug addiction, flare-ups of inflammatory disease, etc.) constitute a group that needs organotropic, supportive treatment of the organs of detoxification and elimination before drainage is implemented. After six weeks of supportive treatment, the regimen shifts to functiotropic support of tissue drainage (Detox-Kit). Patients with low toxic exposure and mild symptoms such as skin rashes and fatigue may begin immediately with the functiotropic/ drainage approach (see Table 1 for summary). As mentioned above, it is vitally important to allow slow exchange systems to release all accumulated toxins. In patients with high toxic loads, this may take several months. Lymphomyosot is thus added to the reg- imen for several weeks or months to ensure complete detoxification. 3. Crinnion WJ. Environmental medicine, part one: the human burden of environmental toxins and their common health effects. Altern Med Rev 2000; 5(1): 52-63. 4. Armstrong B, Hutchinson E, Unwin J, Fletcher T. Lung cancer risk after exposure to polycyclic aromatic hydrocarbons: A review and meta-analysis. Environ Health Perspect 2004;112(9):970-978. 5. Brody JG, Rudel RA. Environmental pollutants and breast cancer. Environ Health Perspect 2003;111(8):1007-1019. 6. Welshons WV, Thayer KA, Judy BM, Taylor JA, Curran EM, vom Saal FS. Large effects from small exposures. I. Mechanisms for endocrine-disrupting chemicals with estrogenic activity. Environ Health Perspect 2003;111(8):994-1006. 7. Van Brandt B. The Disease Evolution Table (DET). J Biomed Ther 2007;Spring:13-15. 8. Smit A. Practical detoxification and drainage. J Biomed Ther 2007;Winter:11-15. 9. Liska D, Lyon M, Jones D. Detoxification and Biotransformational Imbalances. Explore 2006;2(2):122-140. 10.Watson WP, Mutti A. Role of biomarkers in monitoring exposures to chemicals: present position, future prospects. Biomarkers 2004;9(3):211-242. 11.Pizzorno JE, Murray MT. Detoxification: a naturopathic perspective. Nat Med J 1998;1:6-17. 12.Kelada SN, Eaton DL, Wang SS, Rothman NR, Khoury MJ. The role of genetic polymorphisms in environmental health. Environ Health Perspect 2003;111(8):1055-1064. Conclusion Treatment of chronic toxin accumulation is individualized according to the severity of the intoxication and the patient’s regulatory status. Several tools are available to asses these factors, but simple questionnaires seem to be the most practical and inexpensive choice. Advanced organotropic organ support is employed first in severe cases, followed by the functiotropic Detox-Kit for drainage. Use of Lymphomyosot over weeks or months ensures drainage of slow exchange compartments such as adipose tissue.| References: 1. Anway MD, Cupp AS, Uzumcu M, Skinner MK. Epigenetic transgenerational actions of endocrine disruptors and male fertility. Science 2005;308(5727):1466-1469. 2. Calabrese EJ, Baldwin LA. Hormesis: Ushaped dose responses and their centrality in toxicology. Trends Pharmacol Sci 2001;22(6):285-291. Liver Urinary tract/ Kidney Lymph Gallbladder Connective tissue Advanced organ support for six weeks for patients with severe toxicity Hepar comp. Solidago comp. Hepar comp. Thyreoidea comp. Alternative products (if above not available) Hepeel Reneel Basic detoxification and drainage for 12 weeks Detox-Kit Detox-Kit Detox-Kit ChelidoniumHomaccord Detox-Kit For cellular detoxification, add Coenzyme comp./ Ubichinon comp. Coenzyme comp./ Ubichinon comp. Coenzyme comp./ Ubichinon comp. Coenzyme comp./ Ubichinon comp. Coenzyme comp./ Ubichinon comp. Pulsatilla comp. Note Cellular detoxification is best added during the advanced organ support phase, although in some cases (e.g., inflammatory skin disease), it is not added until the basic detoxification phase. Continue with Lymphomyosot for 4-6 weeks for patients with mild toxicity and 12 weeks for patients with severe toxicity. Dosage Ampoules: In general, 3-1 times weekly 1 ampoule i.m., s.c., i.d. Drops: In general, 10 drops 3 times daily ) Table 1: Advanced and basic detox therapy Journal of Biomedical Therapy 2007 ) Vol. 1, No. 2 7 ) What Else Is New? Napping is no substitute for a good night’s sleep If another woman likes the way he looks … Left: Daytime napping in young Parents should forget about daytime naps for their children and instead make sure the kids get to bed on time. A recent study examined the relationship between sleep patterns and the behavior and intelligence of 738 children aged two to twelve. Children who took naps during the day had a harder time going to sleep at night and getting up the next morning. Other studies indicate that due to sleep deficits, children who nap are also more likely to be moody in the mornings and to perform poorly on intelligence tests. The consequences are similar when children go to sleep too late, even if they do not nap during the day. Parents are advised to be consistent about ensuring that their children go to bed (and go to sleep) in time to get all the sleep they need in one uninterrupted period of rest. That women and men think differently was known long before the publication of books such as Men are from Mars, Women are from Venus or Why Men Don’t Listen and Women Can’t Read Maps. Many studies have confirmed that the genders process emotional events and logical sequences differently. A new study now illustrates gender differences in behavior as well. In this study, men and women were asked to rate the attractiveness of men in photos. The researchers showed the viewers pairs of male faces with the profile of a woman between them. In some cases, the woman was smiling; in others she was not. If the woman appeared to be smiling at one man, female viewers also tended to find him the to their peers who only sleep at night. children may be linked to poorer sleep and mental functioning in comparison Right: Women will prefer the men that other women find attractive. more attractive of the two, whereas male viewers rated him as the less attractive. The authors concluded that women judge a man’s attractiveness according to how other women react to him. By contrast, men react negatively to men whom women consider attractive – a fact the researchers associated with the competitive character of male thinking. Proceedings of the Royal Society 2007;274(1611):899-903 New Scientist June 30, 2007;(2610):14 F O R P RO F E S S I ONA L U S E ON LY ) 8 The information contained in this journal is meant for professional use only, is meant to convey general and/or specific worldwide scientific information relating to the products or ingredients referred to for informational purposes only, is not intended to be a recommendation with respect to the use of or benefits derived from the products and/or ingredients (which may be different depending on the regulatory environment in your country), and is not intended to diagnose any illness, nor is it intended to replace competent medical advice and practice. IAH or anyone connected to, or participating in this publication does not accept nor will it be liable for any medical or legal responsibility for the reliance upon or the misinterpretation or misuse of the scientific, informational and educational content of the articles in this journal. The purpose of the Journal of Biomedical Therapy is to share worldwide scientific information about successful protocols from orthodox and complementary practitioners. The intent of the scientific information contained in this journal is not to “dispense recipes” but to provide practitioners with “practice information” for a better understanding of the possibilities and limits of complementary and integrative therapies. Some of the products referred to in articles may not be available in all countries in which the journal is made available, with the formulation described in any article or available for sale with the conditions of use and/or claims indicated in the articles. It is the practitioner’s responsibility to use this information as applicable and in a manner that is permitted in his or her respective jurisdiction based on the applicable regulatory environment. We encourage our readers to share their complementary therapies, as the purpose of the Journal of Biomedical Therapy is to join together like-minded practitioners from around the globe. Written permission is required to reproduce any of the enclosed material. The articles contained herein are not independently verified for accuracy or truth. They have been provided to the Journal of Biomedical Therapy by the author and represent the thoughts, views and opinions of the article’s author. Journal of Biomedical Therapy 2007 ) Vol. 1, No. 2 ) What Else Is New? Pedestrians chatting on a cell phone in street traffic pose a significantly higher risk to both themselves and others than either iPod users or ordinary pedestrians. What to do when your avatar is sick? Alternative treatment for apes, snakes, and elephants Cell phones distract pedestrians Since 2003, an artificial world has been in the making on the online platform “Second Life” (www.sec ondlife.com). This imaginary world promises its inhabitants, called avatars, a life in paradise. Each user has the opportunity to create his or her own avatar as a virtual alter ego. Avatars are usually attractive, rich, and successful. They acquire property, build houses, and buy and sell with virtual money. They can also take advantage of medical services. Recently, the first German-speaking medical practice opened in “Second Life,” offering office hours for one hour each week. A virtual nurse cares for patients in the practice. Mental health patients can seek treatment in the clinic of an Australian psychiatrist. Health services such as Ann Myers Medical Center or the New Babbage Medical League provide information and tips about health issues, and eight national Institutes of Health are registered. Of course, there is no way to tell whether real medical professionals stand behind the virtual offerings. Increasingly, sick animals in the Singapore Zoo are being treated (and cured) with alternative therapies instead of conventional medicine. Chinese herbal mixtures often help when classical medicine fails. For example, phytotherapy was used to cure an orangutan’s digestive problems and a snake’s chronically swollen snout, and acupuncture was successful in treating a limping female elephant. The zoo’s head veterinarian emphasizes that he uses Western medicine first but is having increasingly frequent success with alternative medicine. Ärztezeitung April 17, 2007 The results of a recent study may mark the beginning of hard times for cell phone users. The researchers concluded that pedestrians using cell phones in street traffic posed a greater danger to themselves and the general public than either iPod users or ordinary pedestrians. The scientists chose a common, everyday situation for their investigation: They observed how many individuals attempted to cross a street without first checking for oncoming vehicles. Almost half (48 percent) of the cell phone users were so engrossed in their conversations that they attempted to cross the street without checking for traffic. This behavior was observed in only 16 percent of the iPod users among participants in the study. Surprisingly, 25 percent of the ordinary pedestrians who made up the control group also attempted to cross without first checking for traffic. Possible fallout from this study might include future restrictions on cell phone use by pedestrians on public streets or loss of insurance coverage for cell phone users who cause accidents. When conventional medicine fails, New Scientist June 2, 2007;(2606):19| Ärztezeitung May 21, 2007 veterinarians of the Singapore Zoo resort to alternative therapies such as Chinese herbal mixtures. Journal of Biomedical Therapy 2007 ) Vol. 1, No. 2 ) 9 ) Practical Protocols Detoxification and Drainage Eliminating toxins from the body By Bruce H. Shelton, MD, MD(h), DiHom There are very few patients who don’t need detoxification and drainage intervention at all. Furthermore, each patient’s status is unique, so in designing a treatment plan, it is important to strike a balance between the patient’s previous exposure (toxic load) and the organism’s ability to detoxify (regulation ability). F ) 10 or this purpose, patients are generally divided into two groups. Group 1 includes patients with mild to moderate toxicity. In general, these are patients with mild symptoms and exposure. They elect to do a general cleansing or have milder diseases such as headaches, acne, etc. Group 2 includes patients with severe toxicity (known exposure) as well as patients with severe diseases such as cancer, autoimmune diseases, etc. These patients’ regulation ability is reduced. Group 2 also includes former drug addicts as well as patients who have received chemotherapy. Due to their advanced toxicity, group 2 patients need advanced supportive detoxification that prepares the organs of detoxification and elimination for the drainage phase (accomplished primarily through Lymphomyosot, a component of the Detox-Kit). The advanced organ support is thus more organotropic in character, whereas the basic detoxi- fication and drainage is more functiotropic. In general, advanced organ support is administered for six weeks, followed by use of the Detox-Kit. In most cases, tissues will still need to be drained of residual toxins, so the use of Lymphomyosot alone is advised for several months longer (for protocols, see BT Winter 2007). Special case 1: Patients with inflammatory skin disease, such as eczema or psoriasis The skin, classically called the “mirror of the soul,” is also a mirror of the liver and the gut. In cases of skin disease, it is essential to remember that the P450-containing system in the skin is the same as that in the liver and in the gut. Psoriasis patients in particular need bowel cleansing, which should be part of the initial advanced organ support. Thus Mucosa compositum and Cutis Journal of Biomedical Therapy 2007 ) Vol. 1, No. 2 compositum play a special role in these patients, although functiotropic medications such as Nux vomica-Homaccord, Berberis-Homaccord, and Lymphomyosot, along with Hepeel, are the mainstays in the treatment of skin disease. Patients with inflammatory skin disease are at high risk of flare-ups if toxin drainage is initiated before the liver and gut are ready to cope with the load. These patients need to be treated with care even though they may not seem very ill. In some cases, flare-ups will simply mean that patients need higher doses of cortisone, but in other cases hospitalization may become necessary if skin sloughing is severe. Patients with eczema are in a Th2 rigidity state, so they should first undergo several weeks of initial immunomodulation to get the disease under control, followed by advanced organ support, before the drainage period is initiated. Engystol is the medication of choice together with the appropriate suis-organ preparation, in this case Cutis compositum. By contrast, patients with psoriasis are in a Th1 state, so they should be treated with Traumeel oral ampoules and Cutis compositum. In both cases, it is preferable to add the catalysts during the drainage phase rather than during advanced organ support (see protocol in Table 1). ) Practical Protocols Psoriatic plaques are areas of inflammation and excessive skin production. They frequently occur on the skin of the elbows and knees. Disease-specific treatment For Th1 rigidity: Traumeel and Cutis compositum For Th2 rigidity: Engystol and Cutis compositum Schwef-Heel Weeks 1-4 (or even longer in severe cases) Liver Urinary tract/ Kidney Lymph Advanced organ support Skin Gut Cutis comp. Mucosa comp. Note Due to the high incidence of leaky gut in inflammatory skin diseases, initial treatment of the gut and immune system is paramount. The suis organs induce Th3 cells, and thus immunetolerance to the corresponding organs. Dosage Ampoules: In general, 3-1 times weekly 1 ampoule i.m., s.c., i.d. Connective tissue Drops: In general, 10 drops 3 times daily Advanced organ support Duration: 6 weeks Liver Urinary tract/ Kidney Advanced organ support Hepar comp. Solidago comp. Alternative products (if above not available) Hepeel Reneel Liver Basic detoxification and drainage For cellular detoxification, add Lymph Skin Gut Connective tissue Cutis comp. Mucosa comp. Thyreoidea comp. Galium-Heel/ Lymphomyosot Schwef-Heel Nux vomicaHomaccord Pulsatilla comp. Urinary tract/ Kidney Lymph Skin Gut Connective tissue Detox-Kit Detox-Kit Detox-Kit Detox-Kit Detox-Kit Coenzyme comp./ Ubichinon comp. Coenzyme comp./ Ubichinon comp. Coenzyme comp./ Ubichinon comp. Coenzyme comp./ Ubichinon comp. Coenzyme comp./ Ubichinon comp. Basic detoxification and drainage Coenzyme comp./ Ubichinon comp. Note Because Schwef-Heel is a potency chord, it does not cause aggravation to the extent classically ascribed to sulfur-containing medications. Adjuvant use of probiotics throughout the treatment should be considered. Dosage Ampoules: In general, 3-1 times weekly 1 ampoule i.m., s.c., i.d. Drops: In general, 10 drops 3 times daily ) Table 1: Protocol for inflammatory skin disease Journal of Biomedical Therapy 2007 ) Vol. 1, No. 2 11 ) Practical Protocols Chronic fatigue syndrome is a complex and highly debilitating disorder characterized by chronic mental and © Stockbyte/Getty Images physical exhaustion. It occurs more often, but not exclusively, in women. Special case 2: Patients with chronic fatigue syndrome to the onset of the syndrome. Due to general immune imbalance (Th2 rigidity) and mitochondrial impairment in these patients, advanced organ support is essential, but even before that, support for the mucous membranes, the immune system, and the neuroendocrine system is helpful. This is best done with a combi- All patients with chronic fatigue syndrome have some form of toxicity. Some of these patients present primarily with symptoms of intoxication and have a history of toxic exposure, often temporally related Disease-specific treatment nation of Mucosa compositum and Tonsilla compositum. After two weeks, advanced organ support can begin, followed by the drainage phase. If relapse occurs during the drainage phase, advanced organ support should be resumed for at least another six weeks (see protocol in Table 2).| Aletris-Heel Followed by detoxification therapy: Liver Urinary tract/ Kidney Weeks 1-2 Lymph Gut Tonsilla comp. Mucosa comp. Weeks 3-8: Advanced organ support Hepar comp. Solidago comp. Tonsilla comp. Alternative products (if above not available) Hepeel Reneel Galium-Heel Nux vomica-Homaccord Pulsatilla comp. Weeks 9-20: Basic detoxification and drainage Detox-Kit Detox-Kit Detox-Kit Detox-Kit Detox-Kit For cellular detoxification, add Coenzyme comp./ Ubichinon comp. Coenzyme comp./ Ubichinon comp. Coenzyme comp./ Ubichinon comp. Coenzyme comp./ Ubichinon comp. Coenzyme comp./ Ubichinon comp. Thyreoidea comp. Note These patients need very gradual treatment. Because they often have multiple chemical sensitivities, it is advisable to first restore the integrity of the gut lining while administering Tonsilla comp. to support the adrenals and the hypothalamus. This also supports the immune system. Dosage Ampoules: In general, 3-1 times weekly 1 ampoule i.m., s.c., i.d. Drops: In general, 10 drops 3 times daily Table 2: Protocol for chronic fatigue syndrome ) Connective tissue 12 Journal of Biomedical Therapy 2007 ) Vol. 1, No. 2 ) Re s e a r c h H i g h l i g h t s Obesity’s Helper in Triggering Diabetes The role of POPs in the pathogenesis of type 2 diabetes mellitus By Catherine E. Creeger I stasis model assessment (HOMA) method.4 The authors selected 19 POPs detected in at least 60% of study subjects and then examined associations of POPs and HOMA of insulin resistance (HOMA-IR) within 5 POP subclasses. n 2006, an international team of researchers analyzed a data subset of the U.S. National Health and Nutrition Examination Survey (NHANES) and discovered striking dose-response relations between serum concentrations of persistent organic pollutants (POPs) and pre valence of diabetes.1 NHANES, conducted by the U.S. Centers for Disease Control and Prevention, was designed to be nationally representative of the non-institutionalized U.S. civilian population. This first study revealed strong associations between both organochlorine (OC) pesticides and nondioxin-like polychlorinated biphenyls (PCBs) and diabetes. Moreover, the prevalence of diabetes was quite low among subjects with high BMIs but low serum concentrations of POPs.1 POPs stored in adipose tissue may therefore play a considerable role in the pathogenesis of diabetes.2,3 Objective In a recently published subsequent study, the team of authors reviewed the same dataset to investigate POPs and insulin resistance (a frequent precursor of type 2 diabetes) in nondiabetic subjects. Research design and methods The NHANES surveys included data on serum concentrations of various biologically important POPs or their metabolites and estimated insulin resistance using the homeo- Results The sample of 749 participants included 46.3% males and 49.7% Caucasians. Mean age was 48.2 ± 18.9 years. Among 5 subclasses of POPs, only OC pesticides correlated strongly with HOMA-IR in these non-diabetic subjects, although specific individual nondioxin-like PCBs were also associated with higher HOMA-IR values. The findings suggest that chlordane (an agricultural pesticide banned in the US since the 1980s) may be the most important POP involved in the pathogenesis of type 2 diabetes by influencing insulin resistance, although there has been no experimental study on the possible biological mechanism(s). Conclusions The present study found serum concentrations of OC pesticides to be strongly and positively associated with insulin resistance among nondiabetic subjects. Coupled with the previous study’s findings on associations between POPs and diabetes, the current results suggest that background environmental exposure to some POPs, especially OC pesticides, may be critically involved in Journal of Biomedical Therapy 2007 ) Vol. 1, No. 2 the pathogenesis of diabetes through a pathway involving insulin resistance. In the POP subclass of OC pesticides and their metabolites, oxychlordane (a chlordane metabolite) and trans-nonachlor (a chlordane impurity) were most strongly associated with insulin resistance in non-diabetic subjects. The interaction between OC pesticides and obesity on the risk of both insulin resistance and diabetes suggests that POPs stored in adipose tissue may play a role in the current epidemic of type 2 diabetes.| (Excerpted from: Lee DH, Lee IK, Jin SH, Steffes M, Jacobs DR. Association between serum concentrations of persistent organic pollutants and insulin resistance among nondiabetic adults. Diabetes Care 2007; 30(3):622-628.) References: 1. Lee DH, Lee IK, Song KE, Steffes M, Toscano W, Baker BA, Jacobs DR Jr. A strong doseresponse relation between serum concentrations of persistent organic pollutants and diabetes: results from the National Health and Examination Survey. Diabetes Care 2006; 29:1638-1644. 2. Porta M. Persistent organic pollutants and the burden of diabetes. Lancet 2006;368: 558-559. 3. Lee DH, Jacobs DR, Porta M. Could low level background exposure to persistent organic pollutants contribute to the social burden of type 2 diabetes? J Epidemiol Community Health 2006;60:1006-1008. 4. Centers for Disease Control and Prevention. Third National Report on Human Exposure to Environmental Chemicals. Atlanta, GA: CDC, 2005. ) 13 ) Around the Globe Spain: Homotoxicology in “Flamenco Country” ) 14 By Rüdiger Schneider, PhD W gram in Manual Medicine and Applied Homotoxicology. The course of study encompasses more than 600 hours of lectures (300 hours each of theoretical and practical work) and awards internationally recognized European continuing education credits. Similar programs emphasizing homotoxicology are already in the planning stages at various other universities. Workshops on homotoxicology are another means of increasing physicians’ knowledge about the use of antihomotoxic medications in daily medical practice. hat is Spain, one of Europe’s favorite vacation destinations, best known for? Bullfights, sherry, Don Quixote, the Prado, the Real Madrid soccer/football team… Each year, many tourists visit Spain’s gorgeous landscapes and bustling cities, enjoy its national cuisine (who can resist paella?), join in its traditional fiestas, or spend their vacations relaxing on its beaches. The Spaniards are proud of their country, their culture, their history, and, last but not least, their language, noted for its rapid-fire tempo. Homotoxicology has been established in Spain for many years. Laboratorios Heel España, S.A.U., with its headquarters near Madrid, may still be known to some of you under its former name, Phinter-Heel. Its initial offerings also included classical homeopathic medications. Meanwhile, the business has grown to employ more than 80 people and successfully markets antihomotoxic medications in Spain. Heel España has its own manufacturing facilities and produces many Heel products locally. As in many other countries, the keystone of Heel España’s success is continuing education programs and symposia, which attract more than 200 participants per event. Through the company’s efforts, homotoxicology is also finding a home in Spanish universities. For example, the Universidad Complutense in Madrid is even offering a masters-level pro- Focus on detoxification Detoxification is an essential component of the antihomotoxic therapeutic model. The other two pillars of antihomotoxic therapy (cellular activation/organ strengthening and immunomodulation) take effect best only after accumulated toxins have been eliminated from the patient’s body. Consequently, basic detoxification with the Detox-Kit (which includes Lymphomyosot, Nux vomica-Homaccord, and Berberis-Homaccord, all in liquid form) is one of the cornerstones of continuing education programs for physicians in Spain. Many health-conscious Spaniards already rely on the Detox-Kit. It is well known that Spain is crazy for sports, especially soccer/football, so it is not surprising that homotoxicology has also found its way Journal of Biomedical Therapy 2007 ) Vol. 1, No. 2 into the country’s elite sporting events: Heel España has succeeded in becoming the sole sponsor of the AEMEF, an association of the team physicians of all 1st and 2nd league soccer/football clubs in Spain, such as Atlético Madrid, Real Madrid, and FC Barcelona. Heel España holds workshops on biopuncture for the physicians and physiotherapists of this association. The workshops demonstrate the effectiveness of suitable antihomotoxic medications in treating sports injuries and show practitioners that this treatment approach ensures a speedy recovery and facilitates an early return to sports activities. | Heel España is the official sponsor of the AEMEF. ) Around the Globe New E-learning Course on Homotoxicology Get your certificate now! By Bruno Van Brandt T he International Academy for Homotoxicology (IAH) provides high-level educational programs and materials on homo toxicology and promotes the homotoxicological model in daily practice. The IAH has recently introduced an abbreviated course on the basics of homotoxicology, available as an e-learning program. Enrolment, study, and certification are free of charge. IAH educational material is written by the world’s leading experts in homotoxicology. It is regularly updated and monitored for scientific accuracy. The IAH abbreviated online course is the fastest way to get up to speed on antihomotoxic therapy. The course centers around detailed discussion of approximately 1000 illustrated slides on 20 main topics in homotoxicology. The high ly instructive and well-illustrated handouts are downloadable and printable from the internet website. Th0 E DH A Co rt iso l How it works Access the IAH website at www.iahonline.com and register. Once you have logged in, select “The IAH Abbreviated Course” and then “Lectures to study” to view the e-learning curriculum. By clicking on the individual lectures, you can open the PDF files and either study the material on screen or print the lectures to make your own textbook. Successfully completing an online multiple-choice examination at the end of the course leads to IAH certification. Just select “Examination” and follow the instructions. After passing the exam, you will receive your certificate by mail within a few weeks. Everything on the IAH website is functionally related to the course of study. There are no distractions or disruptions, no commercial pop-ups or extraneous links competing for your attention. Once on the website, you can concentrate on learning the basics of antihomotoxic treatment. The many advantages of this IAH abbreviated internet course include: After passing the exam, students will receive a certificate. • Studying when and where you want, at your own pace • Absolutely no charge for the program • Course presented in clear, succinct language • Material regularly updated and monitored for scientific accuracy • Practical tips for therapy and follow-up • Convenient online multiple-choice examination • Certification by the IAH, the only worldwide academy for homotoxicological education The IAH abbreviated online course is open to medical doctors and li censed healthcare professionals.| Th3 Th2 Th1 IL-4, 13 IL-2 IFN-gamma TGF-beta IL-5 IL-10 TNF Inhibition Inflammation Allergy Page taken from the lecture “Immunomodulation” © IAH 2007 by of hormones ed the mother tly DHEA) is call many other (and subsequen to manufacture Pregnenolone many body d by the body for use ary is it ess e nec aus researchers bec g our sex hormones that are ne, cortisol, etc.). They are udin gestero and mineral hormones, incl osterone, pro s such as fat ., estrogen, test y body function racteristics, and functions (e.g ntenance of man mai and female cha e the mal for e other responsible ss, maintaining demand to thes stre on it s ing troll vert con metabolism, con EA and then y produces DH in the others. The bod ns ctio iated rea g of Th-1 med hormones. e on the long unity or skewin but will stimulat es cellular imm Th-1 reactions, retion of cortisol DHEA stimulat sec bits m inhi -ter isol that a long reas cort balance, whe nce, inducing We can state iated reactions. g at the Th-2 side of the bala auto-immune term Th-2 med win cer. Some will induce a ske and even can (e.g., stress) une diseases, -imm auto . e hn) allergies, som the ., morbus Cro both sides of Th-1 driven (e.g in TGF-β, inhibit diseases are dysbalance but the release of or cells, over intervene in the As Th-3 regulat ulation), it does not directly reg ion. and balance (down β or Th-2 express 1 IL-1 Thof n the both bits the secretio el S the intensity of 1 Traumeel S inhi is why Traume duction. That research that bit cortisol pro We know from ng others. mediators inhi F-α. These two flammation, amo Curriculum of the IAH abbreviated course in homotoxicology Journal of Biomedical Therapy 2007 ) Vol. 1, No. 2 ) 15 ) Re f r e s h Yo u r H o m o t ox i c o l o g y Synergy Between Functiotropic and Organotropic Therapy By Alta A. Smit, MD The three fundamental pillars of antihomotoxic medicine – detoxification and drainage, immunomodulation, and organ support – are implemented to optimize restoration of equili brium. Homotoxicology sees the body’s attempts to maintain homeostasis as symptoms and the extent to which regulation is possible or not possible as disease. T ) 16 he Disease Evolution Table classifies the progression of disease. In simple terms, the regulation/compensation (R/C) division separates phases in which the patient is still able to regulate towards health from phases in which only compensation is possible. Applying the pillars can assist the patient’s attempts at regulation. To the left of the R/C division, we are dealing primarily with disturbances in function; to the right, disturbances in both function and structure are present. This distinction is less clear in the impregnation phase (where cell death may be visible only on the microscopic level) than in the degeneration and dedifferentiation phases (where structural disturbances generally become macroscopic). Clearly, therefore, diseases that involve only functional disturbances will require a different approach than diseases involving disturbances in structure as well as function. During the excretion, inflammation, and deposition phases, regulation still takes place via excretory mechanisms, so physiological support will reactivate the organism’s self-regulation. However, once the condition has progressed to the right of the R/C division, healing cannot be achieved without structural support for specific organs. Classification of antihomotoxic medicines: organotropic vs. functiotropic Organotropic medications act on a specific organic system or tissue, whereas functiotropic medications have biochemical and metabolic effects on several organ systems. Among antihomotoxic medicines, the action of the homaccords and many of the basic combination medications is functiotropic, whereas the composita and catalysts act organotropically. Each pillar, therefore, presents both functiotropic and organotropic therapeutic options. Taking the detoxification and drainage pillar as our first example, the Detox-Kit contains two homaccords – Berberis-Hom accord, with functiotropic effects on the kidneys, and Nux vomica-Hom accord, with functiotropic effects on the intestines and liver – along with one basic combination (Lymphomyo sot, which acts on the lungs, liver, matrix, and kidneys). A homaccord is a combination of two or three single-ingredient potency chords with identical potencies. As with most antihomotoxic medicines, the action of homaccords is both synergistic and complementary. Much has been written about the choice of potencies in the accords. Dr. Reckeweg was also a musician, and many scholars believe there are similarities between some ) Re f r e s h Yo u r H o m o t ox i c o l o g y Functiotropic Organotropic Basic combinations Composita Homaccords Injeels (e.g., Hepeel) (e.g., Hepar compositum) (e.g., Nux vomica-Homaccord) (e.g., Hepar suis-Injeel) Fig. 1: Organ strengthening of the liver of the accords and chords in music.1-3 There are also mathematical models that explain the choice of dilutions in the homaccords. In any case, there is no doubt that the homaccords are an essential part of antihomotoxic treatment. In the Detox-Kit, they effectively deal with mild to moderate toxicity in all diseases to the left of the R/C division. In more serious illnesses, the homaccords (like the basic combinations) serve to restart regulation and are generally administered after a period of organ support. Basic combinations are the other component of functiotropic treatment. Here, too, the combination of synergistic and complementary effects induces physiologic regulation. Traumeel and Lymphomyosot are two of the most well-known combinations. There is a long history of therapeutic use of organ extracts in homeopathy. In homotoxicology, the work of August Bier is thought to have influenced Reckeweg to include them in the antihomotoxic repertoire. In his work on treating chronic disease, Bier had noticed that organ extracts are more effective than secretory products of the same organs and concluded that treating disease in a specific organ requires a prepared extract of that organ. Through their work in the Charité clinic in Berlin, Bier and Reckeweg were able to demonstrate empirically that organ therapy is a superior form of treatment for chronic disease. Now scientific evidence is emerging to support the idea of “resonance” between organ extracts and their corresponding organs. Today, fetal human liver cells and liver extracts are being used for liver regeneration.4 If therapy with extracts of a particular tissue has regenerative effects on that tissue, the same should hold true of the organotropic suisorgan preparations in antihomotoxic medicines. Composita and suis-organ Injeels are examples of medications containing organ extracts. The importance of Reckeweg’s formulations, however, lies in the fact that he recognized the interdependence among different organ systems, as mentioned above. Thus the formula of Cutis compositum includes liver and adrenal extracts, recognizing the relationships between the skin and stress hormones and between the P450 detoxification enzymes in the skin and the liver. Of course the inclusion of liver and adrenal extracts also counteracts iatrogenic damage from products used in skin disease. On the right side of the R/C division, use of catalysts as well as composita becomes mandatory. Because no cell can function without energy, Journal of Biomedical Therapy 2007 ) Vol. 1, No. 2 the role of catalysts in maintaining cell health is increasingly being re cognized, along with their therapeutic possibilities. For this reason, advanced organ support protocols include catalysts in addition to a number of composita containing suis organ extracts. Conclusion Functiotropic and organotropic me dications are administered either singly or in combination, depending on the severity of the disease process. An example is basic detoxification and drainage and advanced organ support in the liver, which can be depicted as shown in Figure 1.| References: 1. Milani L. Re-Homaccord® nudo: analisi cri tica sugli accordi di potenza e potenze accor date. Medicina Biologica 2005;23(4): 45-51. 2. Cahis M. Exact homoeopathy. In: Transactions of the Eighth Quinquennial Homoeopathic International Congress. Vol 2. London: Publisher unknown;1911:125-147. 3. Cahis M, Kubasta, Kubasta S. Die Homöopathie experimentell bewiesen. Berliner homöopathische Zeitschrift 1913;(4):1-12. 4. Ochenashko OV, Nikitchenko YV, Volkova NA, Mazur SP, Somov AY, Fuller BJ, Petrenko AY. Functional hepatic recovery after xenotransplantation of cryopreserved fetal liver cells or soluble cell-factor administration in a cirrhotic rat model: Are viable cells necessary [published online ahead of print August 27, 2007]? J Gastroenterol Hepatol. PMID: 17725601. ) 17 ) M a r k e t i n g Yo u r P r a c t i c e Marketing to Target Groups Are You Getting the Patients You Deserve? By Marc Deschler Marketing specialist “You can’t determine who comes to your practice,” said a therapist I met with recently. I countered with questions: Would seniors feel comfortable with designer furniture? How long would self-employed patients be willing to wait? Eventually, he admitted that deliberate measures actually can influence a practice’s clientele. I t is no secret anymore that patients want to be known by name and given friendly service and personal care. However, all of this simply ensures that you will get patients; it does nothing to steer specific types of patients in your direction. If you want to define a specific target group for your practice, you need to ask yourself two questions: 1. Who are my current patients? 2. Who are the patients I want to treat? Statistics on office visits alone tell you precious little – only whether you are seeing more patients or fewer than before. Your patient database or Rolodex ought to supply basic answers to question 1. ) 18 Journal of Biomedical Therapy 2007 ) Vol. 1, No. 2 What information do you need? 1. What is the age distribution of my patients? Five-year increments are a practical way of grouping your patients by age: How many of your patients are ages 1-5, 6-10, etc.? Heavily represented age groups will be readily apparent. It is also useful to compare this information to data on your community as a whole so you can tell whether the age distribution in your practice is typical of your area. Community-wide data should be available from local authorities. 2. What is the gender break down? 3. What is the distribution of privately or publicly ensured and self-paying patients, policyholders and family members, working patients and retirees/seniors? 4. Where do my patients come from? Creating a table of postal codes will allow you to estimate your catchment area. ) M a r k e t i n g Yo u r P r a c t i c e How well do you know your clientele? A patient questionnaire will tell you who your patients are and what they expect from you. 5. Why do patients come to my practice? A patient questionnaire is a quick and easy way to answer this question. (After making modifications, use a second questionnaire to assess the success of your efforts.) 6. When and how often do patients come to my practice? Knowing the frequency and timing of office visits of each of these patient groups will help you schedule your office hours more effectively. After you have identified your current clientele, the next step is to decide on your future target group. That is easy for businesses that sell products – they simply drop certain sales areas or step up their advertising on the basis of which groups buy the most. In a healthcare practice, however, you will want to consider whom you want to serve and can treat most effectively. Steps to take 1. Define your goals. These goals need to be quantifiable, realistic, and specific. To accomplish the goal of having more patients who pay out-of-pocket, all you need to do is treat 51 such patients this year in comparison to 50 last year. Make your goal specific: In the next two quarters, I will see 40 new patients in the 30-40 year age range. 2. Identify problems experi enced by your target group. Unless you know what your target group is looking for, you cannot offer solutions. For example, are you targeting working people who value short waiting times? 3. Develop solutions. What will the solutions look like? Brainstorm with your assistants or seek advice outside your practice. Possible solutions might include offering evening and weekend office hours or guaranteed appointment times; improving the parking situation, changing the services you offer, changing the ambiance in your office, etc. 4. Implement solutions. The best solutions amount to nothing without meticulous planning and implementation. Do you need to have a team meeting about scheduling changes? Optimize your appointment planning, talk to your landlord, take a continuing educa- tion course, or improve the signage in your office? Make sure everyone on your staff knows who needs to do what and when. Conclusion Getting the patients you want requires discipline, strategizing, and in-depth information about your current patients. Current data can also help you identify deviations from your target state and respond quickly. Specializing in a particular target group will have positive effects not only on your job satisfaction but also on your ability to survive in the marketplace. The internationally known marketing expert Edgar K. Geffroy once said something to the effect that lasting security is achieved only through customers in the form of target groups. You will not have to worry about growing your practice as long as you specialize in one target group and constantly keep its needs in mind. It is true that most practitioners do not need to be concerned about growth, but good target marketing also increases patient loyalty and ensures a steady income due to returning patients.| To define a specific target group, health care practitioners need to decide which patients they want to treat. Journal of Biomedical Therapy 2007 ) Vol. 1, No. 2 ) 19 ) Specialized Applications Detoxification of Patients in the Dedifferentiation Phase By Kristy Anderson, ND Toxins and cancer are closely related. A number of environ mental toxins contribute to the development of cancer and may do so even in minute doses through the process of hormesis.1 Toxins may affect the DNA itself and act as genotoxins, or they may function as adjuvants to the development of certain cancers in genetically susceptible individuals.2,3 C ancer therapies themselves are toxic and harmful to healthy cells as well as diseased cells. Anti neoplastic agents are useful in treating tumors but have several side effects and may accumulate in the tissues, increasing the toxic burden. There is also clear evidence that some antineoplastic drugs are themselves carcinogenic.4 ) 20 Special precautions in cancer patients As a general rule, patients undergoing active chemotherapy should be put on only the advanced organ support phase of detoxification, not on the drainage part with Lymphomyosot, because the concentration of chemotherapy drugs needs to be maintained for as long as possible for full effectiveness (see protocol in Table 1). Unless they are in true long-term remission, patients with soft tumors such as lymphoma and leukemia should not undergo drainage with Lymphomyosot and Galium-Heel at all. Increased lymph drainage may spread the tumor. Severely debilitated patients or patients who are in remission or post chemo but still weakened should not undergo aggressive detoxification and drainage. Special care is also needed in patients with hormone-dependent cancers such as breast or prostate cancer, which may respond to endocrine-disrupting toxins (e.g., organochlorines) released from the matrix. Detoxification and especially drainage should be extremely gradual in these patients. They often benefit from a longer period of advanced organ support (12 weeks) and from administering the components of the Detox-Kit in succession rather than simultaneously: Nux vomicaHomaccord first, followed by Berberis-Homaccord and finally Lymphomyosot. (For the general protocol and rationale for advanced organ support vs. basic detoxification, see BT Spring 2007.) Journal of Biomedical Therapy 2007 ) Vol. 1, No. 2 With these considerations in mind, we can separate patients into groups with different detoxification needs: 1. Healthy patients at high risk for cancer In such cases, treatment is prophylactic and can often be quite aggressive. However, for patients in one of the high-risk groups (including obese patients or those with known high toxin exposure) advanced organ support must be administered first, as described in Table 1. Detoxification and drainage should be performed at least twice a year for three years, especially if the patient is non-reactive. (Non-reactive patients are often not susceptible to acute feverish illnesses but are susceptible to deep viral recurrences, such as Epstein-Barr and zoster. This is a sign of Th2 rigidity and is therefore indicative of a low cellular immunity, which is a risk factor in cancer.) Extended drainage with Lymphomyosot (at least 12 weeks after the basic detoxification and drainage with the Detox-Kit is completed) is advised. These patients may experience an episode of acute feverish illness, which is a good sign. 2. Patients in remission who need to detoxify aggressively This group consists of patients who have completed cancer therapy and are officially in remission after subsequent check-ups. Their detoxifica- ) Specialized Applications tion needs are similar to those of group 1, but detoxification should be more gradual, especially as these patients may have residual kidney and liver damage from aggressive chemotherapy. For them, the detoxification and drainage process begins with an advanced organ support phase, followed by the basic detoxification and drainage phase. Again, drainage alone is continued for several weeks after the basic treatment. 3. Able-bodied patients with seemingly incurable cancers Here, the aim is to prolong high quality of life. Antihomotoxic medicine is very well suited to these patients, and they often enjoy a heightened sense of well-being after a course of treatment. In general, the Disease-specific treatment drainage phase is not implemented in these patients unless they are well and the tumor is progressing slowly. Support for cellular respiration is very important in these cases, as is advanced organ support, which allows the body to detoxify at its own pace (for general protocols, see BT Winter 2007). The organism needs extra energy to detoxify properly, so it must be sufficiently vigorous before detoxification and drainage are initiated. Since the object is to preserve quality of life, aggressive detoxification and drainage should not be implemented. 4. Cancer patients who have received chemotherapy As mentioned earlier, at least six weeks should elapse between com- pleting chemotherapy and beginning tissue drainage. See the protocol in Table 1 for treatment during chemo and support afterwards.| References: 1. Calabrese EJ, Baldwin LA. Hormesis: Ushaped dose responses and their centrality in toxicology. Trends Pharmacol Sci 2001;22(6): 285-291. 2. Armstrong B, Hutchinson E, Unwin J, Fletcher T. Lung cancer risk after exposure to polycyclic aromatic hydrocarbons: A review and meta-analysis. Environ Health Perspect 2004; 112(9):970-978. 3. Brody JG, Rudel RA. Environmental pollutants and breast cancer. Environ Health Perspect 2003;111(8):1007-1019. 4. Haussmann W. Carcinogenicity of cytostatic agents – Secondary malignancy after chemotherapy. In: Rüther U, Nunnensiek C, Schmoll H-J, eds. Secondary Neoplasias Following Chemotherapy, Radiotherapy, and Immunosuppression. Contrib Oncol. Vol 55. Basel: Karger; 2000:36-61. 1. Select organ system where cancer is present 2. Add Ginseng compositum Advanced organ support (may be started during chemo) Liver Urinary tract/ Kidney Lymph Gut Connective tissue Advanced organ support Hepar comp. Solidago comp. Tonsilla comp. Mucosa comp. Thyreoidea comp. Alternative products (if above not available) Hepeel Reneel Nux vomica-Homaccord Pulsatilla comp. For cellular detoxification, add Coenzyme comp./ Ubichinon comp. Coenzyme comp./ Ubichinon comp. Coenzyme comp./ Ubichinon comp. Coenzyme comp./ Ubichinon comp. Coenzyme comp./ Ubichinon comp. Note The organotropic compositum medications support the organs of detoxification but do not stimulate active drainage. If patients are very ill, do not start them immediately on Ubichinon comp. Tonsilla comp. must be given by mouth. Cutis compositum (supportive in alopecia) can be added when chemotherapy affects the skin and hair. Dosage Ampoules: In general, 3-1 times weekly 1 ampoule i.m., s.c., i.d. Drops: In general, 10 drops 3 times daily Begin six weeks after chemotherapy or as a follow-up to advanced support: Disease-specific treatment 1. Medication specific to the type of cancer 2. Ginseng compositum Liver Urinary tract/ Kidney Lymph Gut Connective tissue Basic detoxification and drainage Detox-Kit Detox-Kit Detox-Kit Detox-Kit Detox-Kit For cellular detoxification, add Coenzyme comp./ Ubichinon comp. Coenzyme comp./ Ubichinon comp. Coenzyme comp./ Ubichinon comp. Coenzyme comp./ Ubichinon comp. Coenzyme comp./ Ubichinon comp. Note If patients develop expectoration from the lungs, Bronchalis-Heel can be added. Use with caution in patients with bronchial carcinoma as Bronchalis-Heel will promote expectoration, and thus mucous flow. Dosage Ampoules: In general, 3-1 times weekly 1 ampoule i.m., s.c., i.d. Drops: In general, 10 drops 3 times daily Table 1: Protocol for cancer patients after chemotherapy Journal of Biomedical Therapy 2007 ) Vol. 1, No. 2 ) 21 ) Making of ... Manufacturing Liquid Medications: How Do Those Drops Get Into the Bottle? By Rüdiger Schneider, PhD No one thinks twice about using liquid medications, especially drops for detoxification and drainage. I’m sure you’ve prescribed the Detox-Kit for your patients or perhaps even used it yourself. But have you ever wondered how those drops get into the bottle? I t all starts with the active ingredients. The mother tinctures are inspected before they are introduced into the manufacturing process. The German Homeopathic Pharmacopoeia (HAB), the basis for all production of homeopathic medications, dictates exactly which lab parameters must be tested. Heel’s internal rules require additional test ing to ensure that production meets GMP standards, so tests for microbiological purity are always performed in addition to tests for physical properties. Each liquid product has its own sheet of production instructions with a bill of material detailing exact quantities of the various components. After the mother tinctures pass in spection, the next step is making single-ingredient dilutions. A number of these dilutions are then combined into a “potency mixture” and potentized together by adding a precisely specified amount of an ethanol/water blend. The potentized mixtures are then combined to produce the finished product. A variety of active ingredients, usually in the form of mother tinctures or single potencies, are used in manufac- ) turing homeopathic drops. Exact quantities are given in the manufactur- 22 ing instructions, which are specific to each medication. Journal of Biomedical Therapy 2007 ) Vol. 1, No. 2 Every step of production is carefully monitored and precisely documented. Alternatively, single-ingredient dilutions may be potentized directly with the ethanol/water blend to create the finished product. Whether potency mixtures or individual potencies are used is precisely defined by the HAB and depends on which raw materials or mother tinctures are involved. To prevent mix-ups when weighing out single-ingredient dilutions, each dilution is labeled not only with its classical homeopathic description but also with a bar code that includes the batch number and material number. Before the newly completed finished product is packaged, it undergoes another series of tests for physical and microbiological properties, including pH, Hazen number, density, and TLC (thin-layer chromatography). The product is cleared for packaging only when all of the test results are satisfactory. Automated recording of all individual steps in the process allows the origins of each batch to be traced at One of the active ingredients of Lymphomyosot drops: Juglans regia, better known as walnut. Equal parts of the fresh leaves and the fresh rind of the green fruit are used to produce the mother tincture. any time. Clearance to proceed to the next step is also issued automatically. In addition, in-process monitoring ensures correct completion of individual production stages and intermediate stages even in complex production runs involving large numbers of ingredients. All workstations involved in either manufacturing or packaging the finished product are doubly inspected before being cleared for use. (Since four eyes are better than two, two employees complete the same checklist.) Before the finished product is packaged, the filling equipment is first cleaned and rinsed. Depending on the fill quantity (30 or 100 ml), the bottling machines can fill either four or six bottles simultaneously. Each assembly line can process approximately 4,000 units per hour, depending on the fill volume. The filling operation is followed by an initial automated inspection of fill levels. Next the tamper evident bottle caps are screwed on and tightened to a predetermined torque; labels (which already include the batch number and expiration date) are then applied. To avoid mix-ups and ensure automatic rejection of any incorrect or damaged packaging, all labels, package inserts, and boxes are marked with bar codes that are read by a scanner. Journal of Biomedical Therapy 2007 ) Vol. 1, No. 2 Filling, labeling, and packing the bottles are fully automated processes. Of course they are also monitored constantly. At this point, the process is nearing completion. The bottles (along with package inserts) are boxed, and the expiration date and batch number are printed on the boxes, which are checked again for completeness before each unit is sealed. A belt weigher at the end of the production line rechecks the fill level and rejects any underfilled bottles. After banding, the new batches are then ready for shipping. The process of manufacturing liquid homeopathic medications is highly complex and requires a correspondingly high degree of documentation. Every step of the way is monitored, and the documentation is constantly checked by the team leader and the production manager. The end result? Those familiar bot tles of drops, which are easy to use and ensure accurate dosing. The best-known example is the DetoxKit, which includes three liquid medications – Lymphomyosot, Nux vomica-Homaccord, and BerberisHomaccord – for detoxification and drainage. The Detox-Kit is becoming increasingly popular worldwide, but that’s hardly surprising, is it?| ) 23 ) Crossword Puzzle Solve the puzzle and win! Here’s how it works: Complete the crossword puzzle and enter the letters from the numbered boxes in the blanks to make a word. Then e-mail your solution to: [email protected] to enter it in our drawing before March 15, 2008. Ten lucky winners will receive copies of the book “Biological Medicine in Pediatrics” (Ulrich Wemmer, ed.). Please remember to include your complete mailing address. Results of the drawing are final. Good luck! Solution to last issue’s puzzle: T r au meel