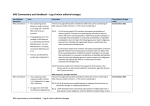
Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Neonatal Abstinence Syndrome Lauritz Meyer, MD September 11, 2015 SDPA Conference Disclosure • I have no financial relationships to disclose. Objectives • Describe the incidence of Neonatal Abstinence Syndrome in the United States • Identify common symptoms of Neonatal Abstinence Syndrome • Familiarize with scoring systems for Neonatal Abstinence Syndrome • Identify treatment strategies for Neonatal Abstinence Syndrome Neonatal Abstinence Syndrome • Defined as a group of clinical signs and symptoms in a neonate resulting from prolonged exposure to illicit or prescribed drugs • Also called Neonatal Drug Withdrawal • Short term syndrome but may have long lasting effects • Can be caused by in-utero exposure or iatrogenic exposure in hospitalized neonates Opiate History • Opium derived from the poppy • First records of opium addiction are from the late 18th century • Increase in opioid addiction among women noted in the 19th century Opiate History • Morphine isolated in 1804 o Use among women was associated with sterility • Heroin synthesized in 1874 • Initially thought addiction among women did not affect infants Opiate History • 1875: first reported case of neonatal abstinence o More over years, most died, no specific treatment • 1903: First report of neonate surviving abstinence after Tx with morphine o Called Congenital Morphinism • 1947: Seizures in a baby with Congenital Morphinism were successfully treated with morphine o Led to increased awareness and name changed to Abstinence Syndrome in Neonates Opiate History • Methadone: • Introduced in 1964 as a replacement treatment for opioid addiction • Methadone clinics became very common for treating recovering heroin addicts • Initially thought to not cause withdrawal in neonates, likely secondary to increased half life but since has become a common cause of NAS Opiate History • Buprenorphine: • Approved as an alternative to methadone for opioid addiction in U.S. in 2002 o Sublingual tablets • Also leads to NAS o May cause less severe NAS symptoms than methadone Illicit Drug Use in the U.S. • 2013 National Survey on Drug Use and Health o 9.4% of population age 12 and older used illicit drugs within the past month (24.6 million individuals) o 5.4% of pregnant women aged 15-44 were current illicit drug users • 14.6% in age 15-17 year olds • 9% in the first trimester • 4.8% in the second trimester • 2.4% in the third trimester o 22.9% of population age 12 and older were binge alcohol users in the past month (60.1 million individuals) • 6.3% were defined as heavy drinkers o 9.4% of pregnant women were current alcohol users, 2.3% were binge drinkers, and 0.4% were heavy drinkers Illicit Drug Use in the Upper Midwest • 2013 National Survey on Drug Use and Health o South Dakota • 6.17% of 12 years and older have used illicit drugs in the past month (42 thousand individuals) o Minnesota • 7.63% of 12 years and older have used illicit drugs in the past month (343 thousand individuals) o Iowa • 7.34% of 12 years and older have used illicit drugs in the past month (188 thousand individuals) Incidence of NAS • Rising • Incidence has nearly doubled in the past 15 years based on national ICD-9 coding • Becoming more widespread o No longer just inner cities o Increased use of prescription pain medications in pregnant women o Improved recognition of NAS NAS Causing Drugs • Opioids o Morphine, Methadone, Hydromorphone, Fentanyl, Heroin • CNS Depressants o Benzodiazepines, Alcohol, Barbiturates • CNS Stimulants o Amphetamines, Cocaine, Nicotine, Caffeine • Hallucinogens o LSD, inhalants, mescaline • Polysubstance use • SSRIs Opioids • Among the world’s oldest known drugs o Use of opium poppy goes back milennia • Three types: natural, endogenous, and synthetic • Produces analgesia by binding to mu-opioid receptors in the CNS, PNS, and GI system o Leads to inhibition of noradrenaline release • Effects include: o o o o Sedation Euphoria Respiratory depression Decreased GI motility • Long term use leads to physical dependence Opioids • Withdrawal o The initial condition that led to the diagnosis of NAS o Abrupt discontinuation leads to: • Massive release of noradrenaline • Leads to autonomic, behavioral, and GI symptoms/signs o Timing, presentation, and severity of symptoms dependent upon maternal and neonatal factors • Drug, dosage, time since last use, placental transfer, metabolism • Mu-opioid receptor (OPRM1) and catechol-o-methyltransferase (COMT) gene genetic variations affect the need for and the length of treatment Opioids • Neonates exposed in-utero have signs/symptoms of opioid withdrawal 55-94% of the time • Addition of other maternal or neonatal medications, neonatal diet, and environmental stimuli can affect the severity and incidence of NAS • Symptoms can present within the first 24 hours of life, or be delayed for 7 days or longer o Dependent on type of drug, metabolism, etc. Clinical Symptoms of NAS due to Opioids • Neurologic o o o o o o o o o Tremors Irritability Increased wakefulness High-pitched cry Hypertonicity Hyperactive reflexes Exaggerated Moro Seizures Frequent sneezing/yawning • Gastrointestinal o o o o o o Vomiting/diarrhea Poor feeding Uncoordinated suck Constant sucking Dehydration Poor weight gain/FTT • Autonomic o o o o o Excessive sweating Temperature instability Nasal stuffiness Mottling Yawning Video • https://www.youtube.com/watch?v=2eP5EnFSG0c Clinical Symptoms (cont.) • Seizures occur in 2-11 percent of NAS cases • EEG abnormalities have been seen in up to 30% of NAS cases attributed to opioids • Increased incidence of Small for Gestational Age (SGA) births • Increased incidence of respiratory difficulties Timing of Withdrawal • Wide variation dependent upon the half-life of the drug and the recent history of drug use • Symptoms can present within the first 24 hours for short half life drugs (Heroin), but may not present for 72 hours up to 7 days or longer for long half life drugs (Methadone, Buprenorphine) • Neonates born to mothers who have gone >7 days from last use are at much lower risk for NAS, but still require close monitoring Methadone • Common prescription drug used for recovering Heroin addicts • Long half life leads to delayed presentation of NAS symptoms for several days • Higher daily doses are more likely to lead to NAS o >95% of infants will develop symptoms with doses >20mg/day • Difficult to wean mothers during pregnancy due to high risk of fetal complications with abrupt dose changes Buprenorphine • Increasing use for opiate withdrawal including during pregnancy • Lower transplacental transfer due to higher molecular weight o Thought to lower the incidence and severity of NAS • Decreased length of stay for infants with NAS • Subutex – buprenorphine only • Suboxone – buprenorphine plus naloxone to guard against misuse Fentanyl • Use of transdermal patch increasing for treatment of chronic pain • Short half life leads to rapid symptoms of NAS in the first 24 hours • Risk of rapid withdrawal for mother if lose access to supply of patches • Breastfeeding a concern due to risk of rapid withdrawal Depressants • Alcohol withdrawal can present 3-12 hours after birth • May show symptoms of NAS similar to opioid withdrawal although usually more mild • Benzodiazepine withdrawal can have a variable onset dependent upon half life and dosage Stimulants • Methamphetamine and cocaine have low rates of NAS requiring therapy • Symptoms at birth more likely the result of drug effects vs withdrawal o Similar symptoms to opioid NAS – tremors, irritability, poor sleep pattern, excessive sucking, etc • High rates of prematurity and IUGR status • Increased risk of placental abruption • Common to see polysubstance use SSRIs • Used in 7-13% of pregnancies • 10-30% risk of Poor Neonatal Adaptation Syndrome • Tremors, increased tone, high pitched cry, poor sleep patterns are common symptoms • Increased rate of respiratory distress • Increased risk of PPHN • Generally presents in the first 48 hours of life and resolve within another 48 hours • Paroxetine (Paxil) carries the highest risk Withdrawal vs Toxicity • Withdrawal: o Symptoms develop as the amount of drug decreases, indicative of dependence on the drug o Most common with opioids, but also with depressants and SSRIs • Toxicity: o Symptoms present early and decrease as the drug is metabolized o Most common with stimulants such as cocaine or methamphetamine Premature Infants • Lower risk of developing NAS <35 weeks • Central Nervous System developmentally immature o Motor dysfunction less able to be expressed • Lower total drug exposure in-utero • Lower fat stores limits build up in the body • Lack of accurate assessment tools to identify symptoms in premature infants – all assessment tools created for term infants • Risk decreases with decreasing GA Iatrogenic NAS • Many NICU patients are exposed to opioids and benzodiazepines during their stay (surgical, sedation for PPHN, ect.) • May develop after 5-7 days of exposure to fentanyl/morphine or benzodiazepines • Important to recognize the risk and treat these infants similar to in-utero exposure to avoid adverse outcomes What To Do? • Neonate is at risk for NAS based on known exposure history or has other risk factors that are concerning for possible NAS • Drug Screen • Initiate abstinence scoring system • Close observation Drug Screening • Urine o Low sensitivity due to need for a recent exposure to show positive o Rapid turn around time (within 24 hours) • Meconium o High sensitivity and specificity o Slow turn around time (days to a week) o May miss meconium if stooled in-utero or at birth and not collected • Umbilical Cord o Increasing use o Not dependent upon collection of urine or meconium o Eliminates possibility of false positive secondary to exposure after birth Abstinence Scoring • Several scoring systems are available with no clear standard • Not drug specific – primarily for opiates • Most hospitals choose one and adapt to their needs • Two most common: Finnegan Neonatal Abstinence Scoring System, Neonatal Withdrawal Scoring System (Lipsitz) • Others available: Ostrea criteria, Neonatal Withdrawal Inventory, Riley Infant Pain Scale Finnegan Finnegan • Most widely used scoring system • Comprised of 20 most common signs and grouped into CNS, metabolic/respiratory, and GI categories • Each symptom assigned a score based on significance and potential for harm • Cumulative score of 7 or less considered mild NAS without need for pharmacologic treatment • Scores >8 suggest careful monitoring and likely need for pharmacotherapy Lipsitz • Assigns a score of 0 to 3 for tremors, irritability, reflexes, stools, muscle tone, skin abrasions, and tachypnea • Assigns a score of 0 to 1 for frequent sneezing, frequent yawning, and vomiting or fever • A score of 5 or greater suggests opiate exposure • A score of 8 or greater indicates need for pharmacotherapy Treatment • Goals of treatment: o Allow the infant to withdraw without excessive excitation that can lead to withdrawal symptoms o Especially important to avoid the most severe, i.e. seizures o Establish a physiologic sleep pattern o Establish consistent weight gain o Allow the infant to communicate needs with caregivers o Help the infant manage new stimuli in its new environment Non-pharmacologic Treatment • First line therapy is ALWAYS non-pharmacologic • Required for all infants with suspected NAS • Keep environmental stimulation to a minimum o Low light o Quiet environment • • • • • Swaddling Gentle handling with cares/cluster cares Quick response to symptoms Demand feeding ***Cuddlers*** Non-pharmacologic treatment • Many large centers with a high population of NAS cases have a specific section or completely separate NICU dedicated to the care of NAS babies • Nursing care with experience in caring for NAS babies is crucial to help ensure a safe and swift recovery Pharmacotherapy • Decision to initiate pharmacotherapy based on abstinence scoring and the known or suspected drug exposure • Indicated when non-pharmacologic treatment is insufficient • Indicated for moderate/severe symptoms • Required to prevent severe complications, i.e. seizures Pharmacotherapy • Drawbacks: o Increases length of drug exposure o Increases length of stay o May impact maternal-infant bonding as a result • Benefits: o Decreases the acute signs of NAS o Decreases the risk of severe complications like seizures or failure to thrive Pharmacotherapy • Ideally treat with the same class of drug as that causing NAS • Choice can be a challenge when drug of exposure is unknown or in setting of polysubstance use Pharmacotherapy • Mainstay of therapy has been opioids • Opioids are first line treatment based on available evidence • Historic use of tincture of opium and paregoric have fallen out of favor due to safety concerns • Morphine and Methadone are the two most common opioids used to treat NAS • Buprenorphine is a potential option but limited safety and efficacy data in neonates o Sublingual dosing appeal Pharmacotherapy Morphine • Variety of dosing regimens available for Morphine • High dose o 0.08-0.1 mg/kg every 4 hours PO • Low dose o 0.03-0.04 mg/kg every 4 hours PO • With either regimen, the dose may be increased by 20% every 8 hours until symptoms are well controlled • Typical maximum dose is 0.2 mg/kg/dose • Other regimens include escalation by changing to every 3 hour dosing Pharmacotherapy Morphine • Weaning is individualized to each patient • Typical approach is to maintain current dose when adequate symptom control is achieved • After 48-72 hours of stability may begin weaning • Wean by decreasing dose by 20% every other day • May require delayed taper or escalation if symptoms worsen Pharmacotherapy Methadone • Typical starting dose of 0.05-0.1 mg/kg every 6 hours PO • Adjust doses up and down by ~20% as needed similar to Morphine • May require less frequent adjustments since half life is longer and effects of dose changes may be slower to manifest than with Morphine nd 2 Line Treatment • Used for severe NAS that is not controlled with a first line agent • Phenobarbital o Most commonly used second line drug • Diazepam o First line if the known cause of NAS is a benzodiazepine • Clonidine o Used to avoid the sedative effects of phenobarbital Phenobarbital Preferred medication for non-opiate NAS GABA agonist Does not prevent seizures at typical NAS doses Minimal benefit for GI symptoms Usual dose: 16 mg/kg loading dose, then 2-8 mg/kg/day divided BID for maintenance • Route: Oral, IV, or IM • Continue treatment until Morphine or Methadone are weaned off before weaning phenobarbital • Taper phenobarbital by 10-20% per day • • • • • Diazepam • Requires caution due to limited capacity of infants to metabolize • Contains sodium benzoate o Requires monitoring for jaundice as it may displace bilirubin for conjugation and excretion • Initial dose 1-2 mg every 8-12 hours • May also consider lorazepam or midazolam dependent on preference and experience Clonidine • Effective adjunctive medication with opioids in shortening the duration of treatment • Centrally acting alpha adrenergic agonist • Requires monitoring for hypotension and bradycardia • Initial dose 0.5-1 mcg/kg followed by 3-5 mcg/kg/day divided every 4-6 hours • Requires taper due to risk of hypertension and tachycardia with abrupt discontinuation Naloxone • Contraindicated in the treatment of NAS due to the risk for rapid and severe NAS symptoms • May precipitate seizures in some neonates Iatrogenic NAS • Treat with same drug class that was used for pain control/sedation • Calculate total daily cumulative dose and divide into a schedule of equivalent medication o Do not forget PRN doses!! Nutrition and NAS • May have increased metabolic demands o May require significant increase in kcal/kg/day to offset losses from NAS o Fortified feeds • Ad lib demand schedule o Prompt response to hunger cues important o May be frequent, small volume feeders • Requires close monitoring of weight gain/loss and fluid status o Vomiting and loose stools may lead to increased fluid requirements • PO intake may be poor N o NG supplementation or IV hydration Breastfeeding • Low rates of breastfeeding among NAS affected neonates • AAP supports breastfeeding in appropriate situations • May help with withdrawal symptoms • Requires strict adherence and review of risks and benefits with the mother before initiation Breastfeeding Allowed • Ok to breastfeed when mothers are on a stable dose of methadone or buprenorphine o Low doses excreted in breastmilk • Mothers who are in a treatment program prior to delivery or are enrolled into a program at birth o Requires strict adherence to the program with continued close follow up • No other contraindications to breastfeeding Breastfeeding Contraindications • Polysubstance abuse or history of non-adherence to treatment programs • HIV or other infectious risk • Mothers taking hydrocodone or oxycodone o Require closer monitoring as these drugs are highly excreted in breastmilk • Any illicit drug use during the 30 day period prior to delivery Breastfeeding • Best to follow strict feeding protocols to ensure a similar amount of breastmilk is provided each day • Have mothers pump and provided pumped breastmilk early on to ensure consistent volumes o Provide for 1-2 feeds on day 1, and gradually increase as supply increases over the following days • Discontinuation of breastfeeding o Important to stress weaning off of breastmilk as abrupt discontinuation may precipitate NAS symptoms at that time Discharge and Follow Up • Infants at risk for NAS require in-hospital monitoring until past the window for severe withdrawal • Dependent upon the drug exposure o With known history of short half life drugs such as morphine or hydrocodone, may be discharged after 72 hours o With known history of long half life drugs such as methadone, may be discharged after 5-7 days • Follow up visit should be scheduled within 2 days of discharge to ensure continued close monitoring Discharge after Treatment • Infants requiring pharmacotherapy: o Discharge frequently delayed until fully weaned off of medications with an adequate observation period off pharmacotherapy to ensure no rebound NAS o Discharge while still on therapy is an option if parents are reliable, taper is easily followed, and adequate follow up is assured o Extensive education about non-pharmacologic measures for treatment of symptoms and strict criteria for seeking evaluation are vital at discharge Prenatal Counseling • Important to be empathetic and nonjudgemental • Teratogenicity o Opioids and stimulants can cause SGA status, prematurity, abruption, SAB o Cocaine and methamphetamine may lead to long term neurodevelopmental issues • Expected Clinical Course o Observation for at least 3-7 days for signs and symptoms of NAS o Non-pharmacologic therapy is the primary treatment o Pharmacotherapy will require treatment that may last weeks to months Prenatal Counseling • Breastfeeding o Breastfeeding may be suitable in certain situations dependent upon the drugs used o Breastfeeding may help decrease NAS symptoms o Helpful to have a breastfeeding plan prior to delivery • Social Concerns o Vital to discuss the importance of caregiver involvement in treatment of NAS o Adherence to follow up schedule and treatment recommendations will be vital to outcomes Take Home Points • NAS is a common condition in newborns and the incidence is rising • Close monitoring is vital for infants at risk of NAS • Infants who demonstrate symptoms without known risk factors require evaluation for NAS • Non-pharmacologic measures are the first line therapy for NAS • Breastfeeding is not contraindicated in NAS in some situations and can be beneficial in NAS treatment References • • • • • • • Avery’s Diseases of the Newborn, 9th Ed. 2012 Burgos A, Burke B. Neonatal Abstinence Syndrome. NeoReviews. 2009;10(5)e222-229. Kocheriakota P. Neonatal Abstinence Syndrome. Pediatrics. 2014;134(2):e547-561. Tolia V, Patrick S, Bennett M, et al. Increasing Incidence of the Neonatal Abstinence Sydrome in the U.S. Neonatal ICUs. NEJM. 2015;372(22)2118-2126. Jansson L. Neonatal abstinence syndrome. UpToDate. 2015. Patrick S, Davis M, Lehman C, Cooper W. Increasing incidence and geographic distribution of neonatal abstinence syndrome: United States 2009-2012. J Perinatology. 2015. 1-6. 2013 National Survey on Drug Use and Health. http://www.samhsa.gov/data/populationdata-nsduh