* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Patient safety wikipedia , lookup
Nurse–client relationship wikipedia , lookup
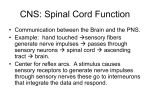
Sensory substitution wikipedia , lookup



![[SENSORY LANGUAGE WRITING TOOL]](http://s1.studyres.com/store/data/014348242_1-6458abd974b03da267bcaa1c7b2177cc-150x150.png)