Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
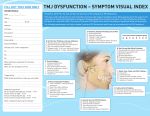
Trismus: Diagnosis and Management Considerations for the Speech Pathologist Melissa Walker, M.S. CCC-SLP Katie Burns, M.S. CCC-SLP ASHA November 16, 2006 Definition From the Greek trismos; grating, grinding Traditional Definition – “Tonic contraction of the muscles of mastication” – Taber’s Cyclopedic Medical Dictionary Current Definition – Any restriction in mouth opening, including restriction caused by infection, trauma, surgery, or radiation Congenital or acquired Definition Uniform criteria is lacking! Various criteria for presence of trismus… – Mouth opening <20mm (Jen et. al., 2002) – Mouth opening <40mm (Nguyen et. al., 1988) – Severity Scales Mild, >30mm; Moderate, 15-30mm; Severe, <15mm (Thomas et. al., 1998) Generally, opening of <35-40mm a functional guideline Less than 18-20mm, oral alimentation is difficult Incidence Reported incidence varies greatly, anywhere from 5% to 38% Incidence increases in irradiated patients Incidence increases with head and neck cancer diagnosis – 36%, Nasopharyngeal tumors – 55%, Parapharyngeal tumors – Parotid gland Complications of Trismus Poor oral hygiene Complications of conditions associated with head and neck cancer treatments Reduced access for oral examination and dental procedures Dysphagia Aspiration and related complications Malnutrition Decreased access for medical procedures, including intubation Inability to use dentures or oral/ pharyngeal prosthetics Speech deficits Airway compromise Pain Anatomy Review Bones: The Mandible Only moveable bone in skull Capable of rapid movement Moves in multiple planes Function: http://zemlin.shs.uiuc.edu/Skull/defult.htm – Mastication – House teeth – Modify dimensions of vocal tract Ligaments Lateral Ligament – Limits & guides movement – Stabilizes Sphenomandibular Ligament – Limits protrusive and mediotrusive movements – Limits passive jaw opening Stylomandibular Ligament – Relaxes with jaw opening Courtesy N. Capra Muscles Bumann & Lotzmann 2002 www.nidcr.nih.gov Muscle Movement Elevation – Masseter – Temporalis – Medial Pterygoid Depression – – – – Digastric Mylohyoid Geniohyoid Lateral Pterygoid Protrusion – External pterygoid – Internal pterygoid Retraction – – – – Temporalis Mylohyoid Geniohyoid Anterior digastric Lateral – External pterygoid – Temporalis Vascular and Neural Supply Vascular Neural Temporomandibular Joint Most active joint in the body Controls mandibular movement Complex and easily damaged joint www.Dr.Spiller.com Easily evaluated TMJ Movement Translation – Upper part of the joint capsule – Bilateral movement – Condyle slips forward and downward over the articular eminence – Suprahyoid muscles Rotation – Lower part of the joint capsule – Condyle rotates within the glenoid fossa – Lateral pterygoids Jaw Opening Initial Phase – Condyle rotates Intermediate Phase – Condyle translates Terminal Phase – Condyle reaches maximum rotation and translation Bumann & Lotzman Jaw Closing Initial Phase Intermediate Phase Terminal Phase The Masticatory System is a Biologic System (Bumann Model) A healthy system adapts and compensates in response to influences – – – – Malocclusion Dysfunction Parafunctional activities Trauma Symptoms arise when the adaptive mechanisms of connective tissue and the compensatory mechanisms of muscles have been exhausted Differential Diagnosis Trismus: Differential Diagnosis Infectious Neurologic Craniofacial/ Dental Oncology – Tumor, Treatment Congenital/ Developmental Trauma Iatrogenic Differential Diagnosis: Infection Odontogenic Infection – – – – Pupal Periodontal Most frequently third molar Secondary to injection Non-odontogenic Infection – – – – Tetanus Tonsillitis Meningitis Encephalitis Differential Diagnosis: Drug Toxicity Medications capable of causing trismus – Neuroleptic agents – Phenothiazines – Tricyclic antidepressants – Metaclopromide – Halothane (general anesthetic) Differential Diagnosis: Trauma Most commonly due to MVA, sport accidents, assault/ battery Most common mandibular fractures – Condylar (30%) – Angle (25%) – Body (20%) Trismus secondary to fracture often exacerbated by prolonged immobility Bony Ankylosis – Hematoma formation within joint space and subsequent fibrosis and calcification Differential Diagnosis: Neurologic Etiologies CVA and TBI – May result in severe trismus secondary to masseter spasticity – EMG will show abnormal tonic hyperactivity at rest ALS – Mazzini et. al. (1995), 9% of patients unable to undergo PEG placement secondary to severe masseter spasticity Restivo et. al. (2005) found masseter botulinum toxin denervation effective in reducing trismus caused by neurogenic spasticity Temperomandibular Disorder (TMJ Syndrome) TMJ pain and reflex spasm of muscles of mastication secondary to… – Excessive tension or anxiety, jaw clenching – Habits, including excessive gum chewing – Disc displacement – Malocclusion – Bruxism Symptoms may resolve on their own Differential Diagnosis: Arthritis True ankylosis unlikely TMJ Arthritis – 50% of those with rheumatoid arthritis have some involvement – Traumatic – Degenerative joint disease Differential Diagnosis: Congenital / Developmental Coronoid Hyperplasia – Abnormal bony elongation of normal coronoid process – Treatment is surgical Hecht Syndrome (Trismus Pseudocamptodactyly Syndrome ) Trotter's Syndrome Differential Diagnosis: Central Nervous System Conditions affecting the CNS may result in trismus, including – Multiple Sclerosis – Meningitis – Parkinson’s Disease – Epilepsy – Bulbar paralysis – Brain tumor – Scleroderma Post-Surgical Effects Dental injections – hematoma formation and infection Nerve damage Misalignment Damage to muscles Hyperextension of joint Scarring Radiation Therapy Trismus most likely when RT to TMJ, pterygoids, or masseter RT for tumors in the nasopharynx, base of tongue, salivary gland, maxilla/ mandible RT in excess of 6000 grays Patients being treated for recurrence Patients treated concurrently surgery and RT Chemotherapy agents may exacerbate the condition Time of Onset Most often a gradual onset, 8 – 12 weeks after completion of treatment May develop at any time following treatment Damage progresses at a rate of approximately 2.4% loss per month Without intervention, mean reduction of 32% opening at 4 years post treatment – Sciubba & Goldenberg, 2006, The Lancet Trismus Secondary to RT Radiation results in rapid formation of collagen – Progression often slow, may not notice until opening is <20mm – Patients may not be eating and not notice slow changes – Patients may think reduced jaw opening is normal Radiation results in on muscle results in fibrosis and contracture When muscles of mastication are in the field of radiation, edema, cell destruction, and fibrosis may result Trismus: Physiologic Effects Joint immobilization results in… – – – – – Reduced strength Fatiguability Rapid joint and muscle degeneration Inflammation, pain Flexion contractures (common in muscles acting across a damaged joint) – Shortening of muscle fibers – Disuse atrophy (Booth, F., 1987, Clin Orthop Relat Res, v219) Pathophysiology of Trismus www.atosmedical.com Evaluation The Trismus Team Patient Speech-Language Pathologist Physical Therapist Dentist/ Orthodontist Oral Hygienist Oral Surgeon Physician Radiation Oncologist Nurse Social Worker SLP Evaluation History and Interview Questionnaire Measure – – – – Interincisal opening Lateral movement Protrusion Retraction Palpation History and Interview Medical/ Surgical/ Trauma History Medications Quality of life measurements Pain history – – – Headaches Jaw Neck Dental status and history Speech and swallowing history Mandibular Function Impairment Questionnaire (MFIQ) (Stegenga et. al., 1993) 11 items assessing perceived difficulties – – – – – – – – – Social activities Speaking Taking a large bite Chewing hard, soft, and resistant foods Work and/ or daily activities Drinking Laughing Kissing Yawning (Stegenga et. al., 1993) Measurement Screening – “Three finger test” Measurement Tools – Boley Gauge – Manufacturer’s scales Dynasplint Therabite Influencing Factors – – – – – Dental alignment Age Gender Ramus length Gonial angle www.atosmedical.com Measurement Reliability Norms (Bumann & Lotzman, 2002) – – – – Jaw opening Laterotrusion Protrusion Retrusion 49-56mm 10-11mm 10-11mm 0-1mm Hypomobility – <40mm (Bitler et. al., 1991) – <35 (Dijkstra et.al.. et.al.. (2006) www.atosmedical.com Measurement Technique Active Opening Passive Opening Lateral Movement Retraction Protrusion Manual Functional Analysis Screen neck mbility At rest and with movement – – – Look Listen Palpate Joint Muscles of mastication Instrumental Evaluation General dental exam Panorex – Confirms degenerative joint changes – Quantify level of asymmetry CT MRI Casting Axiography – Evaluates trajectory Traditional Treatments None/ Compensation – Diet modification Clothespins Screws “Open your mouth” Manual pressure Chewing gum Tongue depressors Dental Treatments Elimination of behaviors that strengthen antagonists Intraoral orthotics Distraction osteogenesis Physical Therapy Icing/ Heat Massage Manipulation/ Traction Compression TENS EMG biofeedback Ultrasound Manual lymph drainage Exercise Facial-Flex Two minutes/ 2x a day Isometric/ Isokinetic Reduces scar formation and lip contraction Open to maximum comfort, close and hold for two seconds Treatment: Passive ROM Passive – External force is applied – Joint moves – Surrounding muscles inactive Benefits – – – – – Improved circulation Reduces inflammation Elongates muscle fibers Mobilizes joint Increases flexibility of connective tissue Buchbinder & Currivan (1991) Passive ROM Devices Dynasplint – Passive – Low load prolongedduration stretch – Spring-loaded – Hands-free option – Adjustable – Customized mouthpiece – 3x/ day for 30 minutes – Rented to patient www.dynasplint.com Therabite Therabite www.atosmedical.com – Efficacy is documented – Dental pads – Passive range of motion – Patient controlled – 7-7-7 protocol – 5-5-30 protocol Therapacer CPM Programmable 18-61 mm 100% passive Motorized Continuous 4-6 hours/day for 4-6 weeks Lateral and protrusive attachments The Final Word Abdel-Galil et.al. References Booth, F.W. (1987). Physiologic and biochemical effects of joint immobilization on muscle. Clinical Orthopaedics and Related Research, 219, 15-20. Buchbinder, D., Currivan, R., & Kaplan (1993). Mobilization regimens for jaw hypomobility ithe radiated patient: A comparison of three techniques. Journal of Oral Maxillofacial Surgery, 51 (8), 863-867. Bumann, A., & Lotzmann, U. (2002). TMJ Disorders and Orofacial Pain: The Role of Dentistryin a Multidisciplinary Diagnostic Approach (K.H. Rateitschak & H.F. Wolf, Eds.).New York: Thieme. Cohen, S.G. & Quinn, P.D. (1988). Facial trismus and myofascial pain associated with infections and malignant disease. Oral Surgery, Oral Medicine, and Oral Pathology, 65, 538-544. Dijkstra, P.U., Huisman, P.M., & Roodenburg, J. (2006). Criteria for trismus in head and neck oncology. International Journal of Oral & Maxillofacial Surgery, 35, 337-342. Greco, J.M. & Van Sickels, J.E. (2001). The Efficacy of Continuous Passive Range of Motion oChronically Injured Temporomandibular Joints. Retrieved 4/6/2006. http://www.craniofacialhealth.com/vansickles.htm. Guralnick, W. and Kaban, L. (1976). Surgical treatment of mandibular hypomobility. Journal of Oral Surgery, 34, 343-348. Jen, Y.M., Lin, Y.S., Su, W.F., Hsu, W.L., Hwang, J.M., Chao, H.L., Liu, D.W., Chen, C.M., Lin, H.Y., Wu, C.J., Chang, L.P., & Shueng, P.W. (2002). Dose escalation using twice-daily radiotherapy for nasopharyngeal carcinoma: does heavier dosing result in a happier ending? International Journal of Radiation Oncology Biology Physics, 54, 14-22. Kadyan, V., Clairmont, A.C., Engle, M., and Colachis, S.C. (2005). Severe trismus as a complication of cerebrovascular accident. Archives of Physical Medicine and Rehabilitation, 86, 594-595. Marien, M. (1997). Trismus: causes, differential diagnosis, and treatment. General Dentistry, 45(4), 350-355. Mazzini, L., Corra, T., Zaccala, M., Mora, G., Del Piano, M., & Galante, M. (1995). Percutaneous endoscopic gastrostomy and enteral nutrition in amyotrophic lateral sclerosis. Journal of Neurology, 242, 695-698. McNeely, M.L., Olivo, S.A., & Magee, D.J.. (2006). A systematic review of the effectivenesss of physical therapy interventions for temporomandibular disorders. Physical Therapy, 86(5) 710-725 Miller,V.J., Karic, V., Myers,S.L. & Exner, H.V.(2000). The temporomandibular opening index(TOI) in patients with closed lock and a control group with no Temporomandibular disorders (TMD): an initial study. Journal of Oral Rehabilitation, 27, 815-816. Moipolai, V., Karic, V. & Miller, J. (2003). The effect of the gonial angle, ramus length, age and gender on the temporomandibular opening index. Journal of Oral Rehabilitation, 30, 1195-1199. Nguyen, T.D., Panis, X., Froissart, D., Legros, M., Coninx, P., & Loirette, M. (1988). Analysis of later complications after rapid hyperfractionated radiotherapy in advanced head and neck cancers. Journal of Radiation Oncology Biology Physics, 14, 23-25. Paterson, A.W., Ryan, W., & Rao-Mudigonda, V. (2006). Trismus: or is it tetanus? A report of a case. Oral Surgery, Oral Medicine, Oral Pathology, Oral Radiology, and Endodontics, 101, 437-441. Restivo, D.A., Maimone, D., Patti, F., Marchese-Ragona, R., Marino, G., & Pavone, A. (2005). Trismus after stroke/TBI: Botulinum toxin benefit and use prePEG placement. Neurology, 64, 2152-2153. Rosted, P., Jǿrgensen, V. (2002). Acupuncture Treatment of Pain Dysfunction Syndrome after Dental Extraction. Acupuncture in Medicine 20 (4),191-192 Simon, J. (2006). Diagnosing and treating the patient with restricted mandibular opening: a new approach. The Compendium of Continuing Education in Dentistry, 27(4), 245-251. Schwerdtfeger, K. & Jelasic, F. Trismus in Postoperative, Posttraumatic and Other Brain Stem Lesions Caused by Paradoxical Activity of Masticatory Muscles (1985). Acta Neurochirurgica, 76, 62-66. Stegenga, B., DeBont, L., Leeuw, R., & Boreing, G. (1993). Assessment of mandibular function impairment associated with temporomandibular joint osteoarthrosis and internal derangement. Journal of Orofacial Pain, 7(2), 183-195. Thomas, F., Ozanne, F., Mamelle, G., Wibault, P., & Eschwege, F. (1998). Radiotherapy alone for oropharyngeal carcinomas: the role of fraction size (2 Gy vs. 2.5 Gy) on local control and early and late complications. International Journal of Radiation Oncology Biology Physics, 15, 1097-1102. Zemlin, W. (1997). Speech and hearing science: anatomy and physiology 4th Ed. New York: Allyn & Bacon.