Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
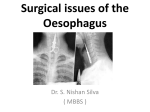
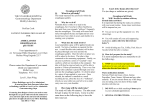
Nig. Of J. Hosp. /Wed. Vol. 18(2)April. -June, 2008 A Clinicopathologic Review Of Oesophageal Carcinoma In Lagos *F.B. Abdulkareem, *C.A. Onyekwere, **N.A Awolola, and *A.A.F Banjo *Dept of Morbid Anatomy, College of Medicine University of Lagos, Idi araba, P.M.B. 12003, Surulere, Lagos, Nigeria **Dept of Morbid Anatomy, Lagos University Teaching Hospital, .-.,-• Id/araba, P.M.B.12003, Surulere, Lagos, Nigeria v + Dept of Medicine, Lagos State University Teaching Hospital, :-,/. Ikeja, Lagos, Nigeria. Correspondence to:. F.B. Abdulkareem ABSTRACT: ••"H".v ,c-ma>.,; ..:•":"*•:' . ~«;'"•'• , <-' .•" growing malignancy in the United States2. Oesophageal cancer has a widely variable geographic incidence in Africa; while it is low in some parts such as Nigeria representing 0.4-0.6% of all malignant tumours 3 4 , it accounts for 13.8% in Addis Ababa and Kenya 56. It is an endemic disease in Transkei, a region along the Indian Ocean coast in South Africa, which is regarded as an epicentre of the disease in Africa7. It is the most important male cancer in some parts of Africa 68. Epidemiological studies have identified tobacco, consumption of maize contaminated by Fusarium verticilloides and nitrosamine as well as HPV infection as risk factors associated with the development of cancer of the oesophagus9'11. Tobacco and HPV infection have been associated with non-endemic Oesophageal cancer while the endemic cancer has been associated with maize meal which is used as staple food due to contamination by fungal mycotoxins as well as nutritional deficiencies 1213 The peak age incidence is in the 6th decade in most studies although adenocarcinoma appears to be commoner in males under the age of 40years 14.There is a racial variation in the histological types with a predominance of squamous cell carcinoma SCC) in blacks which represents over 90% of all Oesophageal cancers in Africa 4'68. Adenocarcinoma is the predominant type in Western countries 14. In fact adenocarcinoma of the oesophagus is said to be the malignancy with the fastest growing incidence in the US, having increased 6 times in 3 decades2. The middle third of the oesophagus is the commonest site for SCC while the tower third is the commonest site for adenocarcinoma5'6'8'14. Most patients present with dysphagia and weight loss with dysphagia being the most important and the first symptom. As most patients present at advanced stage, mortality is very high and even in operable tumour, post operative mortality is about 50%15. The aim of this study is to review the clinicopathological characteristics of Oesophageal carcinoma in Lagos, South West Nigeria. •'•'> Background: Oesophageal cancer is the 6th most common cause of cancer death world wide. While the incidence is low in some parts of Africa such as Nigeria accounting for 0.40.6% of all malignant tumours, it is endemic in Transkei, in South Africa, which is regarded as an epicentre of the disease in Africa. Objective: To document the age and sex distribution, clinical as well as histopathological characteristics of Oesophageal carcinoma in Lagos, SW Nigeria, Methods: The paraffin embedded blocks and slides as well as pathology reports of Oesophageal carcinoma collected between 1995 and 2007 from Morbid Anatomy Department of the Lagos University Teaching Hospital and between 2002 and 2007 from two private histopathology laboratories in Lagos State were reviewed. The clinical data such as the age, sex, and clinical summary were extracted from demographic information in patients' case file. Results: Twenty cases representing 2.8% of all gastrointestinal tumours were recorded. The mean age ? was 65.4years(SD-12.3) with M:F ratio of 1:1. Squamous cell carcinoma predominated; 18 cases (90%); the • remaining two cases (one of which showed evidence of Barrett's oesophagus) were adenocarcinoma (10%). All presented at advanced stage with dysphagia and weight loss with or without vomiting, regurgitation, and/or haematamesis. Two third had mid Oesophageal fungating masses, the remaining were located in the lower third. Two cases had surgery, the rest were not fit for any intervention. Conclusion: Oesophageal cancer is not common in Lagos, Nigeria, majority are squamous cell carcinoma. Late presentation gives it a dismal outlook. Although the overall survival is poor, efforts at improving quality of life by palliative measures should be encouraged. Key Words: Oesophageal cancer, squamous carcinoma, dysphagia .; INTRODUCTION •;.iyv j - i i ^ -, MATERIALS AND METHODS ii Oesophageal cancer is the 681 most common cause of cancer death world wide'. A six fold increase in incidence has been reported over the last decade in Americans and Oesophageal adenocarcinoma is said to be the fastest '-'V :.:'-,'. IV'1 i> vh::--. ;, ^\)^ -: ' The materials consisted of paraffin embedded blocks and slides as well as pathology reports of oesophageal carcinoma cases collected between 1995 and 2007 from the archives of Morbid Anatomy Department of the Lagos 53 University Teaching Hospital (LUTH) and between 2002 and 2007 from two other private histopathology laboratories in Lagos State. The relevant haematoxylin and eosin stained slides were reviewed and (in poorly differentiated tumours), special stains such as Periodic Acid Schiff stain, Alcian blue stain were utilized where necessary to demonstrate the presence of neutral and acid mucin respectively. Presence or absence of columnar metaplasia with goblet cells was also recorded to ascertain any associated Barrett's oesophagus. The clinical information such as the age, sex, and clinical summary were extracted from the histopathology request forms and the patients' case files in their various clinics or hospitals. Also noted was the presence or absence of features of reflux oesophagitis as well as the endoscopic findings and forms of management. The tumours were classified using the standard histological characteristics and graded according to the degree of histological differentiation. The data were then analyzed using Microsoft Excel and presented as tables and figures RESULTS A total of 20 cases representing 2.8% of all gastrointestinal tumours were recorded during the period of study (11 cases from the Morbid Anatomy dept, LUTH 1995-2007 and 9 cases from two private laboratories in Lagos from 2002-2007). The age range was 43-84years age with a mean of 65.4years; SD-12.3(Figure 1). The male: female ratio is 1:1 Of all the cases, only two had oesophagectomy specimens in addition to biopsy; the remaining were endoscopic biopsy samples. Histologically, squamous cell carcinoma (SCC) predominated; 18 cases (90%) with 2 cases (10%) of adenocarcinoma. Six cases each (33%) of the SCC were well, moderately and poorly differentiated respectively. One of the adenocarcinoma cases showed evidence of Barrett's oesophagus. All the patients presented at advanced stage (stages III and IV) with dysphagia and weight loss (100%), 75% presented with additional vomiting/regurgitation, while 10% presented with retrosternal pain and haematamesis (Figure 2). Two third of the cases had mid oesophageal fungating and/or ulcerating masses causing varying degrees of luminal obstruction, the remaining were located in the lower third. Only two cases whose tumour was located in the lower third of oesophagus had surgical intervention, the rest were not fit for any intervention.. 50-59 60-69 70-79 > 80 unspecified Agegroupinyears Om ale • fern a l e Figure 1: Age & Sex distribution of cases of oesophageal carcinoma To 8 retrosternal pain I J haematasis vomiting + regurgriation dysphagia+ weight loss i i 0% 20% 40% 60% 80% 100% : 120% Percentage of pa« ente : Figure 2: Clinical features of oesophageal carcinoma in Lagos, Nigeria ;f>, DISCUSSION < This study has shown that oesophageal carcinoma is uncommon in Lagos, South West Nigeria indicating a frequency of 1.5 cases per annum. This is far low compared to the finding of Pindiga et al in Ibadan, also in South West Nigeria who recorded 177 cases in SOyears (6cases per annum)4. Although oesophageal cancer has widely variable geographic incidence, the difference between our study and that of Ibadan could partly be explained by the presence of a virile cardiothoracic unit in the latter which has been absent in Lagos for over a decade. The presence of experts and improved hospital facility for diagnosis in an area has often been associated with attendant increase in incidence6. Until a few years ago, Morbid Anatomy department of LUTH was the only histopathological facility available to government and private hospitals in Lagos State. Lagos which is a commercial city, situated in South Western part of Nigeria has a population of about 9 million and the inhabitants are representatives from all the major cultural tribes in Nigeria. Inadequate endoscopic facilities may also have contributed to non diagnosis of the disease. It is no wonder then that the present series is the first histopathology report from Lagos. In this study oesophageal cancer (EC) accounted for 2.8% of all malignant gastrointestinal tract(GIT) tumours; a figure which is lower than 9.5-13.3% recorded in previous studies from Nigeria and 32.5% recorded from Addis Ababa816'17. When compared with reports from other parts of Africa such as Kenya, Ethiopia and South Africa, the incidence of oesophageal cancer in Nigeria appears to be relatively low5 8. Other parts of the world with high incidence of this cancer include Northern Iran, Kazakhastan, and Northern China with incidence exceeding 200 per 100.00018. In Kenya, it was found to be the commonest cancer in males representing 13.8% of all malignant tumours6. In Transkei, South Africa, it was reported to be a major cause of death with age standardized rate of 357.2 per 100,000 for age between 35-64years '9. Several risk factors have been implicated in the geographic variation in incidence of EC. In endemic high incidence areas, the histological type is SCC which is the one that has been associated with the presence of certain carcinogens in the environment including tobacco, HPV infection, fungal mycotoxins, nitrosamines, solanum nigrum710"13. Fungal mycotoxins, fumonisin B1 produced by fusarium verticilloides is found in commercial corn world wide but much more common in high incidence areas 12 20. Both the fungus and the toxins are known to be carcinogenic. Tobacco has strong association with non-endemic EC worldwide; higher with increased consumption 2 '. In Zimbabwe, the relative risk f o r oesophageal cancer was 5.7 among male smokers of 15 sticks or more per day". Nitrosamines in non-endemic areas has been proven to be carcinogenic and its effect is dose and time related acting as co-carcinogen with other agents and is found in tobacco and some foods (dried spices, fried bacon and beer) with high urinary excretion having been reported in China21. HPV has been identified in 67-71% of SCC of EC in endemic areas, particularly types 11, 16, 18 which cause neoplastic transformation through their oncoproteins E6 and E72223. Human papilloma virus (HPV) appears not to play significant role in pathogenesis of SCC of EC in the UK 24. Although no definite exposure to any of these predisposing agents was established in any of our patients, it will be worthwhile to explore these risk factors particularly in Nigeria where HPV prevalence of 26.3-42.2% has been reported in cytological samples of Nigerian women 2526. Maize diet in various forms is consumed by inhabitants of this country and due to increasing urbanization; many more individuals are being exposed to tobacco and alcohol. The male: female ratio of 1:1 in this study concurs with previous studies from Ibadan, SW Nigeria 4, and Kenya6 but contrasts with 3.4:1 recorded in the US". The difference could be explained by the higher incidence of adenocarcinoma (81%) in the US study which also noted that adenocarcinoma had greater male predominance with ratio of 4.9:1 than 1.2:1 for SCC 14. The mean age of 64.5years in this study also concurs with previous studies from within and outside Nigeria4'6'14'27. SCC is the predominant histological type of EC in this study accounting for 90% of cases. This is similar to reports from other parts of Africa and India in which over 90% are SCC46827. This contrast with studies from the USA in which adenocarcinoma accounted for 81% and SCC accounted for 17%14. In another study among Asian/Pacific Islanders in the US, the rate of oesophageal SCC was 81% higher than in whites28. The high prevalence of adenocarcinoma in Western countries reflects the pathophysiology of the tumour which has been associated with gastro-oesophageal reflux disease (GERD). Only two of our cases, (10%) were adenocarcinoma, with one case showing histological features of Barrett's oesophagus. Although data from Africa is scanty, a review of GERD in African literature by several workers have confirmed that overall, there is higher prevalence of GERD and adenocarcinoma in western countries than in all regions of sub-saharan Africa and that although urbanisation has increased the risk factors associated with GERD, the impact of this is yet to be seen 29,30 The location of the tumour within the length of the oesophagus varies with the histological type. SCC is commonly found in the middle and distal third of the oesophagus while adenocarcinoma is more commonly located in the distal third. In this study, over 60% of our cases were located in the middle third, the remaining in the lower third which is consistent with previous studies68. The two most common symptoms present in all our patients were dysphagia and weight loss which is similar to previous studies from within and outside Africa 4 6 ' 8 1 4 31 Dysphagia and weight loss are so commonly associated that some authors regard them as being pathognomonic 6. Dysphagia is usually associated with bulky tumours that obstruct the oesophageal lumen, impairing its function and causing pain14; the reason why most patients also have associated vomiting and regurgitation as well odynophagia and or retrosternal pain. Only two of our patients presented with haematemasis, a symptom which is less common. EC in Nigeria has a dismal prognosis because of the advanced stage at presentation. Majority of our patients presented with late stage disease; (stages III and IV) making them inoperable. In operable cases, resection even when successful only offers palliation for severe dysphagia not cure. Several workers have reported high post-operative mortality of over 50%, following oesophagectomy for oesophageal carcinoma15 33'35. Oesophageal cancer is therefore not common in Lagos, Nigeria, majority are squamous cell carcinoma. Late presentation gives it a dismal outlook. Although the overall survival is poor, efforts at improving quality of life by palliative measures should be encouraged. •; ACKNOWLEDGEMENT We are grateful to the management of The Specialist laboratory and Histolab diagnostics limited for allowing us access to their records. REFERENCES 1. Hendricks D, Parker Ml. Oesophageal cancer in Africa. IUBMB Life. 2002; 53:263-8. 2. Pohl H, Welch HG. The role of over-diagnosis and reclassification in the marked increase of oesophageal adenocarcinoma incidence. J Natl Cancer Inst 2005; 97:142-6. 3. Okobia MN, Aligbe JU. Pattern of malignant diseases at the University of Benin Teaching Hospital. Trap. Doct. Apr 2005; 35: 91-92. 4. Pindiga HU, Akang EE, Thomas JO, Aghadiuno PU. Carcinoma of the oesophagus in Ibadan. East Afr Med J, 1997;74:307-10. 5. Ahmed AA. The surgical management and outcome of oesophageal cancer in Addis Ababa. Ethiop Med J, 2000; 38:147152.. 6. Wakhisi J, Patel K, Buziba N, and Rotich J. Esophageal cancer in north rift valley of western Kenya, Afr Health Sci. 2005; 5: 157-163 7. Sammon AM. Carcinogens and endemic squamous cancer of the oesophagus in Transkei, South Africa. Environmental initiation is the dominant factor; tobacco or other carcinogens of low potency or concentration are sufficient for carcinogenesis in the predisposed mucosa. Med Hypotheses. 2007; 69:125-31. 8. Ali A, Ersumo T, Johnson O. Oesophageal carcinoma in Tikur Anbessa Hospital, Addis Ababa. East Afr Med J. 1998; 75:590-3. 9. Walker AR, Adam F, Walker J, Walker BF. Cancer of the oesophagus in Africans in sub-Saharan Africa: any hopes for its control? Eur J Cancer Prev. 2002; 11:413-8. 10. Yu MC, Garabrant DH, Peters JM, MackTM. Tobacco, alcohol, diet, occupation and carcinoma of the oesophagus. Cancer Res 1988; 48:3843-8. 11. Vizcaino Ap, Parkin DM, Skinner ME. Risk factors associated with oesophageal cancer in Bulawayo, Zimbabwe. Br J Cancer, 1995; 72: 769-73. 12. Turner PC, Nikiema P, Wild CP. Fumonisin contamination of food: progress in development of biomakers to better assess human health risks. Mutat Res. 1999; 443:81-93. 13. Sammon AM, Iputo JE. Maize meal predisposes to endemic squamous cancer of the oesophagus in Africa: breakdown of esterified linoleic acid to free form in stored meal leads to increased intragastric PGE2 production and low -acid reflux. Medical Hypothesis, 2006; 67: 1431-1436. 14. Schlansky B, Dimarino Jr AJ, Loren D, Infantolino A, Kowalski T, Cohen S. A survey of oesophageal cancer: pathology, stage and clinical presentation.Alimen Phamacol Ther 2006, 23: 587-593. 15. Obajimi MO, Ogunseyinde AO, Brimmo IA, Adebo AO. Trans-hiatal oesophagectomy as palliative treatment for carcinoma of the oesophagus. East Afr. Med J 2002; 79:311-6. 16. Atoba MA, Olubuyide IO, Aghadiuno PO. Gastrointestinal malignancies in a young tropical African population. Trap. Doct; 1989; 19:135-136. 17. Obafunwa JO. Pattern of alimentary tract tumours in Plateau state: a middle belt area of Nigeria. J of Trop Med & Hyg. 1990; 93: 351-354. 18. Zhang ZX, Li BY, Jin SS. Epidemiologic trends of oesophageal cancer in Linxian Shi Guan Gan Zhi Yaqn Fiu-Lixian. 1990; 1:1-14 19. Doll R. The geographical incidence of cancer. Br J Cancer 1969; 1:1-8. 20. Marasas WF. Fumonisins: their implications for human and animal health. Nat Toxins 1995; 3:193-198 21. Lu S, Ohshima H, Fu HM. Urinary excretion of N-nitrosamino acids and nitrates by inhabitants of high and low-risk areas for oesophageal cancer in Northern China: endogenous formation of nitroso-proline and its inhibition by vitamin C. Cancer Res 1986; 46:1485-1491. 22. Cooper K, Taylor L, Govind S. Human papillomavirus DNA in oesophageal carcinomas in South Africa. J.Pathol. 1995; 175:273-277. 23. Williamson AL, Jaskiesicz K, Gunning A. The detection of HPV in oesophageal lesions. Anticancer Res. 1991; 11:263-265. 24. Morgan RJ, Perry AC, Newcomb PV, Hardwick RH, Alderson D. Human papillomavirus and oesophageal carcinoma in the UK. EurJ Surg Oncol. 1997; 23:513-517. 25. Thomas JO, Herrero A, Omigbodun AA, Ojemakinde K, Ajayi IO, Fawole A et al. .Prevalence of papillomavirus infection in women in Ibadan, Nigeria: a population-based study. British Journal of Cancer (2004) 90, 638-645. 26. Tornesello ML, Duraturo ML, Buonaguro L, Vallefuoco G, Piccoli R, Palmieri S et al. Prevalence of human papillomavirus genotypes and their variants in high risk West Africa women immigrants in South Italy. Infect Agent Cancer. 2007, 3;2:1-9. 27. Matsha T, Erasmus R, Kafuko AB, Mugwanya D, Stepien A, Parker Ml. Human papillomavirus associated with oesophageal cancer. J Clin Pathol 2002; 55:587-590. 28. Cherian JV, Sivaraman R, Muthusamy AK, Jayanthi V. Carcinoma of the esophagus in Tamil Nadu (South India): 16-year trends from a tertiary center. J Gastrointestin Liver Dis. 2007; 16:245-249. 29. Wu X, Chen VW, Ruiz B, Andrews P, Su J, Correa P. Incidence of oesophageal and gastric carcinomas among American Asians/Pacific Islanders, whites and blacks. Cancer, 2005, 106:683-692. 30. Segal I. Gastro-oesophageal reflux disease complex in sub-saharan Africa.(review). Eur J Cancer Prev. 2001; 10:209-212. 31. Kang JY. Systematic review: Geographic and ethnic differences in gastrooesophageal reflux disease. Pharmacol Ther 2004; 20:705-717. 32. Lakatos PL, Lakatos L, Fuszek P, Lukovich P, Kupcsulik P, Halbasz J, Schaff Z, Papp J.Incidence and pathologic distribution of oesophageal cancer at the gastro-oesophageal junction between 1993-2003. Orv Hetil 2005;146:411-416. 33. Osinowo O, Alonge T. Oesophageal reconstruction using the stomach. West Afr J Med 1992; 11:235-243. 34. Sinzobahamvya N. Oesophagectomy for carcinoma of the oesophagus-early results. Cent Afr J Med, 1990; 36:304-308. 35. Adegboye V.O, Obajimi M.O, Ogunseyinde A.O, Brimmo I.A, Adebo A.O. Trans-hiatal oesophagectomy as palliative treatment for carcinoma of the oesophagus. East Afr Med J 2002; 79:311-319.