Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Calorie restriction wikipedia , lookup
Hadrosaur diet wikipedia , lookup
Gluten-free diet wikipedia , lookup
Vegetarianism wikipedia , lookup
Low-carbohydrate diet wikipedia , lookup
Epidemiology of metabolic syndrome wikipedia , lookup
Saturated fat and cardiovascular disease wikipedia , lookup
Ketogenic diet wikipedia , lookup
Raw feeding wikipedia , lookup
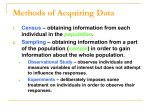
Dietary Approaches to Stop Hypertension Diet and Incidence of Stroke Results From 2 Prospective Cohorts Susanna C. Larsson, PhD; Alice Wallin, MSc; Alicja Wolk, DMSc Downloaded from http://stroke.ahajournals.org/ by guest on April 29, 2017 Background and Purpose—High adherence to the Dietary Approaches to Stop Hypertension (DASH) diet is associated with lower risk of hypertension, the major risk factor for stroke. We examined whether adherence to the DASH diet is inversely associated with the incidence of stroke. Methods—The study population comprised 74 404 men and women (45–83 years of age), without stroke at baseline, from the Cohort of Swedish Men and the Swedish Mammography Cohort. Diet was assessed with a food-frequency questionnaire. A modified DASH diet score was created based on consumption of vegetables, fruits, legumes and nuts, whole grains, low-fat dairy, red meat and processed meat, and sweetened beverages. Stroke cases were identified through linkage to the Swedish National Patient and Cause of Death Registers. Relative risks and 95% confidence intervals were estimated using Cox proportional hazards regression model. Results—During 882 727 person-years (mean, 11.9 years) of follow-up, 3896 ischemic strokes, 560 intracerebral hemorrhages, and 176 subarachnoid hemorrhages were ascertained. The modified DASH diet score was statistically significantly inversely associated with the risk of ischemic stroke (P for trend=0.002), with a multivariable relative risk of 0.86 (95% confidence interval, 0.78–0.94) for the highest versus the lowest quartile of the score. The modified DASH diet score was nonsignificantly inversely associated with intracerebral hemorrhage (corresponding relative risk=0.81; 95% confidence interval, 0.63–1.05) but was not associated with subarachnoid hemorrhage. Conclusions—These findings indicate that high adherence to the DASH diet is associated with a reduced risk of ischemic stroke. Clinical Trial Registration—URL: http://www.clinicaltrials.gov. Unique identifiers: NCT01127698 and NCT01127711 for the Swedish Mammography Cohort and the Cohort of Swedish Men, respectively. (Stroke. 2016;47:986-990. DOI: 10.1161/STROKEAHA.116.012675.) Key Words: epidemiology ◼ food ◼ proportional hazards models ◼ prospective studies ◼ risk factors ◼ stroke T he Dietary Approaches to Stop Hypertension (DASH) diet is rich in vegetables, fruits, and low-fat dairy products and has reduced amounts of saturated fat, total fat, and cholesterol.1,2 This diet considerably reduces blood pressure in hypertensive and normotensive individuals.1 Because hypertension is the major risk factor for stroke, the DASH diet may lower stroke risk. Few studies have examined this hypothesis.3,4 Therefore, we assessed the association between adherence to the DASH diet and incidence of stroke in Swedish middle-aged and older adults. between 1918 and 1952 (n=100 303) received, by mail, a 350-item questionnaire that sought information on diet and other risk factors for chronic diseases; 48 850 men (49%) completed the questionnaire. The Swedish Mammography Cohort was established in 1987 to 1990 with the aim to assess the association of dietary and hormonal factors with the risk of breast cancer.5 In the late autumn of 1997, Swedish Mammography Cohort participants who were still alive and living in the study area received a new questionnaire that was identical, except for some sex-specific questions, to the questionnaire used in the Cohort of Swedish Men. A total of 39 227 women (70% response rate) answered the 1997 questionnaire. Because the 1987 to 1990 questionnaire did not include information on major risk factors for stroke, we used the 1997 questionnaire as baseline for this study. We excluded men and women with an incorrect or a missing personal identification number (n=540), those who died before the start of follow-up (n=81), those with stroke or ischemic heart disease (n=7790) or cancer (n=4403) before baseline, and those who had inadequately completed the dietary questionnaire (n=859). This left 74 404 participants (39 969 men [age, 45−79 years] and 34 435 women [age, 49−83 years]) for analysis. Ethical approval was acquired from the Regional Ethical Review Board at Karolinska Institutet in Stockholm, Sweden. Methods Study Population We used data from 2 Swedish population–based prospective studies: the Cohort of Swedish Men and the Swedish Mammography Cohort. The Cohort of Swedish Men began in the late autumn of 1997 when all men who resided in Västmanland or Örebro County and were born Received January 6, 2016; final revision received January 26, 2016; accepted January 28, 2016. From the Unit of Nutritional Epidemiology, Institute of Environmental Medicine, Karolinska Institutet, Stockholm, Sweden. Correspondence to Susanna C. Larsson, PhD, Unit of Nutritional Epidemiology, Institute of Environmental Medicine, Karolinska Institutet, SE-171 77 Stockholm, Sweden. E-mail [email protected] © 2016 American Heart Association, Inc. Stroke is available at http://stroke.ahajournals.org DOI: 10.1161/STROKEAHA.116.012675 986 Larsson et al DASH Diet and Stroke Risk 987 Diet Assessment and DASH Score Downloaded from http://stroke.ahajournals.org/ by guest on April 29, 2017 A food-frequency questionnaire (FFQ), designed to measure the Swedish diet, was used to assess diet. Participants were asked to report their average intake of 96 foods/food items during the past year. Eight predefined frequency categories, ranging from never to ≥3 times per week, were provided for most foods. For frequently consumed foods (eg, milk, yogurt, and bread), participants were asked to indicate their exact consumption per day or per week. The validity and reproducibility of the FFQ have been described previously.6,7 For example, the mean correlation coefficient between fourteen 24-hour recall interviews and FFQ-based estimates was 0.65 for macronutrients. The DASH diet used in this study was adapted from the DASH diet score created by Fung et al.3 The score by Fung et al3 included vegetables, fruits and fruit juices, legumes and nuts, whole-grain products, low-fat dairy foods, red meat and processed meat, sweetened beverages, and sodium. We modified this score by excluding sodium because the FFQ used in the Swedish Mammography Cohort and Cohort of Swedish Men cohorts did not include salt used in cooking or at the table, and therefore, total dietary sodium intake could not be estimated. Sodium restriction was not included in the original DASH diet.1 Participants were classified into quintiles by their consumption of each food component. For the first 5 components, participants were provided a score from 1 to 5 for being in the lowest to the highest quintiles of intake. Scores were reversed (5–1 for the lowest to the highest quintiles) for red meat and processed meat and sweetened beverages for which low consumption was desired. The modified DASH (mDASH) diet score ranged from 7 (minimal adherence) to 35 (maximal adherence). Assessment of Covariates The baseline (1997) questionnaire contained information about education, weight, height, physical activity (including walking/bicycling and exercise over the preceding year), smoking status and history, aspirin use, family history of myocardial infarction before 60 years of age, alcohol consumption, and history of hypertension, high cholesterol levels, and diabetes mellitus. Data on atrial fibrillation were acquired from the Swedish National Patient Register. We defined diabetes mellitus as a diagnosis of diabetes mellitus in the Swedish National Patient Register or the Swedish National Diabetes Register and complemented with self-reported history of diabetes mellitus. Body mass index was calculated as weight divided by the square of height (kg/m2). Pack-years of smoking history were calculated by multiplying the number of packs of cigarettes smoked per day by the number of years of smoking. Case Ascertainment and Follow-Up Incident stroke cases were ascertained by linkage with the Swedish National Patient Register (includes inpatient and outpatient [nonprimary care] data) and the Swedish Cause of Death Register (also includes nonhospitalized cases). Stroke cases were classified according to the International Classification of Diseases, 10th Revision codes: I63 for ischemic stroke, I61 for intracerebral hemorrhage, and I60 for subarachnoid hemorrhage. Validation studies of the Swedish National Patient Register have found that 96% of stroke cases are identified via this register8 and that 92% of the patients with stroke are correctly classified.9 Participants contributed person-time of follow-up from January 1, 1998, to the date of diagnosis of stroke, death from any cause, or censoring date (December 31, 2010), whichever came first. Statistical Analysis Participants were classified into quartiles according to their adherence to the mDASH diet. We also analyzed the mDASH diet score as a continuous variable (per 5-U increment; about 1 SD). Cox proportional hazards regression models stratified on age (in months), and sex was used to estimate hazard ratios (hereafter referred to as relative risk) with 95% confidence intervals (CIs). Multivariable models included education (less than high school, high school, or university), family history of myocardial infarction before 60 years of age (yes or no), smoking (never; past <20 or ≥20 pack-years; and current <20 or ≥20 pack-years), aspirin use (never, 1–6 tablets per week, and ≥7 tablets/wk), walking/bicycling (quintiles), exercise (quintiles), body mass index (kg/m2; continuous), and history of hypertension (yes or no), hypercholesterolemia (yes or no), diabetes mellitus (yes or no), and atrial fibrillation, as well as total energy intake (kcal/d; continuous) and alcohol consumption (g/d; sex-specific quintiles). The proportional hazards assumption (tested using Schoenfeld residuals) was satisfied. We performed tests for trend by creating a variable containing the median value for each quartile of the mDASH diet score. This variable was entered as a continuous variable in the model. Stratified analyses by smoking status (ever or never) and history of hypertension (yes or no), hypercholesterolemia (yes or no), diabetes mellitus (yes or no), and atrial fibrillation (yes or no) were conducted to assess potential effect modification. Multiplicative interaction was tested by including an interaction term into the multivariable model that also included the stratification variable and the mDASH diet score (in quartiles). The likelihood ratio test that compared models with and without the interaction terms was used to test the statistical significance of the interactions. All P values were 2-tailed (α=0.05). The statistical analyses were performed using SAS (version 9.4; SAS Institute, Cary, NC). Results Compared with participants with low adherence to the mDASH diet score, those with high adherence were slightly older and were more likely to be have a postsecondary education but less likely to be current smokers and overweight (Table 1). Furthermore, they were more physically active and consumed less alcohol. During 882 727 person-years (mean, 11.9 years) of followup, 3896 ischemic strokes (2223 in men and 1673 in women), 560 intracerebral hemorrhages (348 in men and 212 in women), and 176 subarachnoid hemorrhages (80 in men and 96 in women) were ascertained. The associations between the mDASH diet score and the risk of stroke types are presented in Table 2. The mDASH diet score was statistically significantly inversely associated with the risk of ischemic stroke. Compared with men and women in the lowest quartile of the mDASH diet score, those in the highest quartile had a 14% (95% CI, 6–22) reduced risk of ischemic stroke. Each 5-U (≈1 SD) increment of the mDASH diet score was associated with 7% (95% CI, 3–10) reduced risk of ischemic stroke. The association between the mDASH diet score and the ischemic stroke did not differ by sex (P for interaction=0.81). High adherence to the mDASH diet was associated with a statistically nonsignificant lower risk of intracerebral hemorrhage but was not associated with subarachnoid hemorrhage. When we stratified the analysis by selected risk factors, the inverse association between the mDASH diet score and the ischemic stroke was stronger in never smokers (multivariable relative risk for the highest versus the lowest quartile=0.80; 95% CI, 0.70–0.92) than in ever smokers (corresponding relative risk=0.89; 95% CI, 0.78–1.01; P for interaction=0.02). The association was not modified by history of hypertension, hypercholesterolemia, diabetes mellitus, or atrial fibrillation at baseline (P for interaction>0.18 for all). Discussion In this prospective study of middle-aged and older adults, adherence to the DASH diet was inversely associated with the incidence of ischemic stroke. Individuals in the highest 988 Stroke April 2016 Table 1. Age-Standardized Baseline Characteristics According to the Modified Dietary Approaches to Stop Hypertension Diet in 74 404 Swedish Adults Quartile of the mDASH Diet Score, Range (Median) Characteristics* 7–18 (16) 19–21 (20) 21–23 (23) 24–35 (27) 18 171 18 521 18 312 19 400 60.0±9.7 60.1±9.5 60.2±9.3 60.5±9.0 Postsecondary education, % 12 16 20 25 Family history of myocardial infarction, % 15 15 15 16 Current smokers, % 31 26 22 18 No. of participants Age, y Aspirin use ≥7 tablets per wk, % 6.4 6.6 6.6 6.9 Walk/bicycle ≥40 min/d, % 29 32 35 40 Exercise ≥2 h/wk, % 48 55 60 67 Overweight (BMI≥25 kg/m ), % 53 51 49 46 Hypertension, % 22 21 21 20 Hypercholesterolemia, % 10 11 11 11 Diabetes mellitus, % 5.9 5.7 5.8 6.2 Atrial fibrillation, % 1.8 1.7 1.6 1.7 Alcohol intake, g/d 12±22 10±16 10±17 8.6±12 Vegetables, servings 1.7±1.1 2.4±1.4 3.1±1.7 4.0±2.2 Fruits and juices, servings 0.9±0.7 1.4±1.0 1.9±1.2 2.7±1.4 Legumes and nuts, servings 0.1±0.1 0.1±0.1 0.1±0.2 0.2±0.3 Whole grains, servings 2.4±1.9 3.3±2.1 3.8±2.2 4.7±2.3 Low-fat dairy, servings 0.8±1.3 1.3±1.6 1.8±1.9 2.7±2.3 Red and processed meat, servings 1.4±0.8 1.2±0.8 1.2±0.8 1.0±0.8 Sweetened beverages, servings 1.1±1.5 0.6±1.1 0.4±0.8 0.2±0.6 2 Downloaded from http://stroke.ahajournals.org/ by guest on April 29, 2017 Daily food consumption BMI indicates body mass index; and mDASH, modified Dietary Approaches to Stop Hypertension. *Values are mean±SD if not otherwise indicated. quartile of the mDASH diet had a statistically significant 14% lower risk of ischemic stroke compared with those in the lowest quartile. There was some evidence of an inverse association between the mDASH diet and the intracerebral hemorrhage, but results were not statistically significant. Two previous prospective studies have reported results on the DASH diet, using the score created by Fung et al,3 in relation to the risk of stroke.3,4 The largest of these studies included 88 517 middle-aged US nurses of which 1242 and 440 women developed ischemic stroke and hemorrhagic stroke, respectively, during 24 years of follow-up.3 In that cohort, Fung et al3 found that the DASH diet score was statistically significantly inversely associated with the risk of total stroke (relative risk for the highest versus the lowest quintile=0.83; 95% CI, 0.71– 0.96) but not ischemic or hemorrhagic stroke possibly because of the smaller number of cases. In a Dutch cohort study of 33 671 adults, including 527 total stroke cases diagnosed over 12.2 years of follow-up, each 1-SD increment of the DASH diet score was associated with a statistically significant 10% lower risk of total stroke.4 In this study, the inverse relationship between the mDASH diet and the risk of ischemic stroke seemed to be stronger in never smokers. However, as several stratified analyses were conducted, the stronger association in never smokers may be a chance finding. In contrast to our findings, in the Nurses’ Health Study, the DASH diet score was more strongly inversely associated with total stroke risk in smokers than in nonsmokers although a test for interaction was not statistically significant.3 The DASH diet has similarities with the Mediterranean diet, which has been associated with a lower risk of ischemic but not hemorrhagic stroke.10,11 However, 2 studies observed no statistically significant association between the Mediterranean diet and the risk of ischemic12,13 or hemorrhagic stroke,12 but the number of ischemic stroke cases (n=177) was limited in one of those studies.13 Like the DASH diet, the Mediterranean diet is abundant in plant foods (vegetables, fruit, nuts, and legumes) and low in red and processed meat. A major difference between the 2 diets is that low-fat dairy products are emphasized in the DASH diet2 but not in the Mediterranean diet where dairy products are considered a detrimental component.14 Other main differences are that the DASH diet is characterized by low amounts of sweets and sugar-containing beverages and, unlike the Mediterranean diet, does not Larsson et al DASH Diet and Stroke Risk 989 Table 2. Relative Risks (and 95% Confidence Intervals) of Stroke Types According to Adherence to the Modified Dietary Approaches to Stop Hypertension Diet in 74 404 Swedish Adults, 1998–2010 Quartile of mDASH Diet Score, Range (Median) 7–18 (16) 19–21 (20) 21–23 (23) 24–35 (27) P Trend* Per 5 U Ischemic stroke Men and women Cases, n 1061 966 947 922 … 3896 211 158 219 049 218 877 233 643 … 882 727 Age and sex adjusted 1.00 0.90 (0.82–0.98) 0.87 (0.80–0.96) 0.81 (0.74–0.89) <0.0001 0.91 (0.88–0.94) Multivariable† 1.00 0.91 (0.83–1.00) 0.90 (0.83–0.99) 0.86 (0.78–0.94) 0.002 0.93 (0.90–0.97) 1.00 0.93 (0.83–1.04) 0.92 (0.82–1.03) 0.89 (0.78–1.01) 0.06 0.94 (0.89–0.99) 1.00 0.86 (0.75–1.00) 0.87 (0.75–1.01) 0.80 (0.69–0.92) 0.005 0.91 (0.86–0.97) Cases, n 156 147 142 115 … 560 Age and sex adjusted 1.00 0.95 (0.76–1.20) 0.94 (0.75–1.18) 0.74 (0.58–0.95) 0.02 0.89 (0.81–0.98) Multivariable† 1.00 1.00 (0.79–1.25) 0.99 (0.78–1.25) 0.81 (0.63–1.05) 0.14 0.93 (0.84–1.03) 1.00 1.04 (0.78–1.37) 1.03 (0.77–1.38) 0.87 (0.62–1.22) 0.52 0.96 (0.84–1.09) 1.00 0.91 (0.61–1.38) 0.91 (0.60–1.36) 0.69 (0.45–1.06) 0.08 0.87 (0.73–1.03) 42 51 37 46 … 176 Age and sex adjusted 1.00 1.13 (0.75–1.71) 0.78 (0.50–1.23) 0.85 (0.55–1.31) 0.25 0.91 (0.77–1.09) Multivariable† 1.00 1.17 (0.77–1.78) 0.84 (0.53–1.33) 0.95 (0.60–1.50) 0.55 0.96 (0.80–1.16) Person-years Men Multivariable† Women Multivariable† Downloaded from http://stroke.ahajournals.org/ by guest on April 29, 2017 Intracerebral hemorrhage Men and women Men Multivariable† Women Multivariable† Subarachnoid hemorrhage Men and women‡ Cases, n mDASH indicates modified Dietary Approaches to Stop Hypertension. *Calculated by assigning the median value to each quartile and treating this variable as a continuous variable. †The Cox proportional hazards regression model is stratified on age (months) and sex and includes education, family history of myocardial infarction before 60 years of age, smoking status, and pack-years of smoking, aspirin use, walking/bicycling, exercise, body mass index, history of hypertension, hypercholesterolemia, diabetes mellitus, and atrial fibrillation and intakes of total energy and alcohol. ‡Analyses by sex were not conducted because of the small number of cases. emphasize moderate alcohol consumption. Furthermore, the Mediterranean diet is characterized by a high intake of olive oil or a high ratio of monounsaturated to saturated fat, whereas the DASH diet is low in fat. Besides a blood pressure–lowering effect, the DASH and Mediterranean diets may lower the risk of ischemic stroke through potential antiatherosclerotic effects as these diets are rich in antioxidants from plant foods and are low in saturated fatty acids and cholesterol. Strengths of this study are the prospective design, objective information on stroke diagnoses obtained via linkage with Swedish registers, and the large number of stroke cases, in particular ischemic stroke. A limitation is the lack of information on salt used in cooking and at the table. We could, therefore, not include dietary sodium in the mDASH diet score. The DASH-Sodium trial showed that additional sodium restriction resulted in even greater blood pressure reduction than the DASH diet without sodium restriction.15 Another limitation is the observational design. Hence, the possibility that residual confounding may have affected our findings cannot be ruled out. Because dietary intake was self-reported through a single FFQ, some misclassification of diet was inevitable. This study is further limited by the lack of data on cardioembolic, largeartery, and lacunar ischemic stroke subtypes. We could, therefore, not investigate whether the DASH diet is more strongly associated with a certain subtype. Finally, as participants were middle-aged and older Swedish adults who were relatively healthy, the generalizability of our results to younger adults, nonwhites, and less healthy populations is unclear. In conclusion, results from this prospective study of generally healthy adults indicate that a diet that resembles the DASH diet, which is widely promoted by the National Heart, Lung, and Blood Institute for the prevention and treatment of 990 Stroke April 2016 hypertension,2 is associated with a reduced risk of ischemic stroke. Sources of Funding This work was supported by grants from the Swedish Stroke Association, the Swedish Research Council for Health, Working Life and Welfare, and the Swedish Research Council/Council for Infrastructures. The funders had no role in the design, implementation, analysis, or interpretation of the data, or in the decision to submit the paper for publication. Disclosures None. References Downloaded from http://stroke.ahajournals.org/ by guest on April 29, 2017 1. Appel LJ, Moore TJ, Obarzanek E, Vollmer WM, Svetkey LP, Sacks FM, et al. A clinical trial of the effects of dietary patterns on blood pressure. DASH Collaborative Research Group. N Engl J Med. 1997;336:1117– 1124. doi: 10.1056/NEJM199704173361601. 2.United States Department of Health and Human Services. National Heart, Lung, and Blood Institute. Your Guide to Lowering Your Blood Pressure with DASH. http://www.nhlbi.nih.gov/health/resources/heart/ hbp-dash-at-glance. Accessed January 23, 2016. 3. Fung TT, Chiuve SE, McCullough ML, Rexrode KM, Logroscino G, Hu FB. Adherence to a DASH-style diet and risk of coronary heart disease and stroke in women. Arch Intern Med. 2008;168:713–720. doi: 10.1001/archinte.168.7.713. 4. Struijk EA, May AM, Wezenbeek NL, Fransen HP, Soedamah-Muthu SS, Geelen A, et al. Adherence to dietary guidelines and cardiovascular disease risk in the EPIC-NL cohort. Int J Cardiol. 2014;176:354–359. doi: 10.1016/j.ijcard.2014.07.017. 5. Wolk A, Bergström R, Hunter D, Willett W, Ljung H, Holmberg L, et al. A prospective study of association of monounsaturated fat and other types of fat with risk of breast cancer. Arch Intern Med. 1998;158:41–45. 6. Khani BR, Ye W, Terry P, Wolk A. Reproducibility and validity of major dietary patterns among Swedish women assessed with a food-frequency questionnaire. J Nutr. 2004;134:1541–1545. 7. Messerer M, Johansson SE, Wolk A. The validity of questionnaire-based micronutrient intake estimates is increased by including dietary supplement use in Swedish men. J Nutr. 2004;134:1800–1805. 8.Ludvigsson JF, Andersson E, Ekbom A, Feychting M, Kim JL, Reuterwall C, et al. External review and validation of the Swedish national inpatient register. BMC Public Health. 2011;11:450. doi: 10.1186/1471-2458-11-450. 9. Appelros P, Terént A. Validation of the Swedish inpatient and causeof-death registers in the context of stroke. Acta Neurol Scand. 2011;123:289–293. doi: 10.1111/j.1600-0404.2010.01402.x. 10.Tektonidis TG, Åkesson A, Gigante B, Wolk A, Larsson SC. A Mediterranean diet and risk of myocardial infarction, heart failure and stroke: a population-based cohort study. Atherosclerosis. 2015;243:93– 98. doi: 10.1016/j.atherosclerosis.2015.08.039. 11. Tsivgoulis G, Psaltopoulou T, Wadley VG, Alexandrov AV, Howard G, Unverzagt FW, et al. Adherence to a Mediterranean diet and prediction of incident stroke. Stroke. 2015;46:780–785. doi: 10.1161/ STROKEAHA.114.007894. 12. Fung TT, Rexrode KM, Mantzoros CS, Manson JE, Willett WC, Hu FB. Mediterranean diet and incidence of and mortality from coronary heart disease and stroke in women. Circulation. 2009;119:1093–1100. doi: 10.1161/CIRCULATIONAHA.108.816736. 13. Gardener H, Wright CB, Gu Y, Demmer RT, Boden-Albala B, Elkind MS, et al. Mediterranean-style diet and risk of ischemic stroke, myocardial infarction, and vascular death: the Northern Manhattan Study. Am J Clin Nutr. 2011;94:1458–1464. doi: 10.3945/ajcn.111.012799. 14. Trichopoulou A, Costacou T, Bamia C, Trichopoulos D. Adherence to a Mediterranean diet and survival in a Greek population. N Engl J Med. 2003;348:2599–2608. doi: 10.1056/NEJMoa025039. 15.Sacks FM, Svetkey LP, Vollmer WM, Appel LJ, Bray GA, Harsha D, et al; DASH-Sodium Collaborative Research Group. Effects on blood pressure of reduced dietary sodium and the Dietary Approaches to Stop Hypertension (DASH) diet. DASH-Sodium Collaborative Research Group. N Engl J Med. 2001;344:3–10. doi: 10.1056/ NEJM200101043440101. Dietary Approaches to Stop Hypertension Diet and Incidence of Stroke: Results From 2 Prospective Cohorts Susanna C. Larsson, Alice Wallin and Alicja Wolk Downloaded from http://stroke.ahajournals.org/ by guest on April 29, 2017 Stroke. 2016;47:986-990; originally published online February 11, 2016; doi: 10.1161/STROKEAHA.116.012675 Stroke is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231 Copyright © 2016 American Heart Association, Inc. All rights reserved. Print ISSN: 0039-2499. Online ISSN: 1524-4628 The online version of this article, along with updated information and services, is located on the World Wide Web at: http://stroke.ahajournals.org/content/47/4/986 Permissions: Requests for permissions to reproduce figures, tables, or portions of articles originally published in Stroke can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office. Once the online version of the published article for which permission is being requested is located, click Request Permissions in the middle column of the Web page under Services. Further information about this process is available in the Permissions and Rights Question and Answer document. Reprints: Information about reprints can be found online at: http://www.lww.com/reprints Subscriptions: Information about subscribing to Stroke is online at: http://stroke.ahajournals.org//subscriptions/