Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
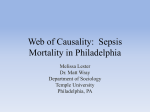
Multicenter, double-blind, placebo-controlled study of the use of filgrastim in patients hospitalized with pneumonia and severe sepsis* Richard K. Root, MD; Robert F. Lodato, MD, PhD; Ward Patrick, MD; John Francis Cade, MD, PhD; Nick Fotheringham, PhD; Steven Milwee, PharmD; Jean-Louis Vincent, MD, PhD; Antonio Torres, MD; Jordi Rello, MD; Steve Nelson, MD; for the Pneumonia Sepsis Study Group Objective: To determine the safety and efficacy of filgrastim (r-metHuG-CSF) in combination with intravenous antibiotics to reduce the rate of mortality in patients with pneumonia and sepsis. Design: This study was multicenter, double-blind, and randomized. Setting: Intensive care units Patients: Adult patients with bacterial pneumonia, either acquired or nosocomial, as confirmed by chest radiograph and positive culture or Gram-negative stain, and severe sepsis, defined as sepsis-induced hypotension or organ dysfunction. Interventions: Standard antibiotic therapy with or without filgrastim (300 g/day) or placebo administered as a 30-min intravenous infusion. The study drug was started within 24 hrs of enrollment and was continued for 5 days or until the white blood cell count reached >75.0 ⴛ 109 cells/L. Measurements and Main Results: The primary end point was the occurrence of mortality through day 29; secondary end points included occurrence of subsequent organ dysfunction, time to discharge from intensive care unit, number of days on mechanical A study of the epidemiology of severe sepsis in the United States determined the national prevalence to be 751,000 cases for the calendar year 1995 with a crude mortality of 28.6% or 215,000 cases (1). The annual increase in severe sepsis cases *See also p. 635. University of Washington, Seattle, WA (RKR), Amgen, Thousand Oaks, CA (SM, NF), The University of Texas Health Sciences Center, Houston, TX (RFL), Hopital Erasme, Brussels, Belgium (J-LV), Queen Elizabeth II Health Sciences Center, Halifax, Nova Scotia, Canada (WP), Hospital Clinical I Provincial, Barcelona, Spain (AT), The Royal Melbourne Hospital, Parkville, Australia (JFC), Hospital Universitari Joan XXIII, Tarragona, Spain (JR), Louisiana State University Health Sciences Center, New Orleans, LA (SN). Supported by Amgen, Thousand Oaks, CA. Address requests for reprints to: Steve Nelson, MD; John H. Seabury Professor of Medicine, Pulmonary/Critical Care Medicine, Louisiana State University Medical Center, Suite 3205, MEB, 1901 Perdido St, New Orleans, LA 70112. E-mail: [email protected] Copyright © 2003 by Lippincott Williams & Wilkins DOI: 10.1097/01.CCM.0000048629.32625.5D Crit Care Med 2003 Vol. 31, No. 2 ventilatory support, and time to death. Study-related observations were recorded through day 10 and included vital signs, onset of organ dysfunction, clinical laboratory variables, and adverse events. Filgrastim increased the white blood cell count to a median peak of 31.7 ⴛ 109 cells/L from a baseline of 12.3 ⴛ 109 cells/L. The two groups were well matched and did not differ significantly with regard to severe adverse events, time to death, occurrence of end-organ dysfunction, days of intensive care unit hospitalization, or days on mechanical ventilatory support. Mortality was low in both treatment groups; the mortality rate in patients with adult respiratory distress syndrome was similar between the two groups. Conclusions: The addition of filgrastim to the antibiotic and supportive care treatment of patients with pneumonia complicated by severe sepsis appeared to be safe, but not efficacious in reducing mortality rates or complications from this infection. (Crit Care Med 2003; 31:367–373) KEY WORDS: pneumonia; sepsis; clinical trials; phase 3; filgrastim; mortality; multiple organ failure was projected to be 1.5%, with the burgeoning elderly population accounting for both the highest incidence and mortality rates. Despite improvements in antimicrobial therapy and supportive care, these data indicate that improved approaches for the management of severe sepsis are a major unmet medical need (2). The lungs constitute the site of origin in at least 50% of the patients with severe sepsis (1, 3). With 6 million cases, 500,000 hospitalizations, and 50,000 deaths from community-acquired pneumonia occurring annually (4), new strategies are needed beyond the appropriate use of antibiotics and proper respiratory and supportive care to improve outcomes in patients with severe cases of pneumonia. Preclinical studies demonstrated that filgrastim (r-metHuG-CSF) can enhance both neutrophil production and function, and improve survival in a variety of animal models of pneumonia (5). In a large (756 patients) placebo-controlled trial, filgrastim given as an adjunct to antibiotics in the treatment of severe community-acquired pneumonia promptly increased circulating neutrophil counts and was well tolerated (6). Furthermore, in a large subgroup of the patients who had multilobar disease, filgrastim treatment accelerated radiologic resolution, reduced complications, and shortened hospitalization in the intensive care unit (6). In various experimental models of sepsis, filgrastim-treated animals have lower mortality rates associated with greater clearance of bacteria and endotoxin and a reduction in cytokine levels compared with placebo controls. Results of a small phase 1/2 pneumonia sepsis study in a severely ill population (Acute Physiology and Chronic Health Evaluation II scores ⬎25) demonstrated the ability of filgrastim to increase absolute neutrophil counts; filgrastim-treated patients had improved resolution of shock 367 and a lower occurrence of mortality (7). Filgrastim was well tolerated and, specifically, acute respiratory distress syndrome rates were not different between placebo and filgrastim-treated groups. Based on these encouraging preclinical and clinical data, it was hypothesized that the addition of filgrastim to a regimen of intravenous antibiotics would reduce the rate of mortality in patients with pneumonia and sepsis. MATERIALS AND METHODS Study Design. The institutional review boards of all participating institutions approved the study design, and all patients or legal guardians gave written informed consent before any study-specific tests were done. The study design was multicenter, doubleblind, randomized, and placebo-controlled. Patients who met the eligibility requirements were randomized to receive filgrastim or placebo in a 1:1 ratio using a predetermined randomization list. A separate randomization list was generated for each center. Study drug was initiated as soon as possible (always within 24 hrs of meeting study entry criteria) and was continued for 5 days or until the white blood cell count was ⬎75.0 ⫻ 109 cells/L. Studyrelated observations, consisting of vital signs, onset of organ dysfunction, laboratory values, and adverse events, continued through day 10. Patient survival on day 29 was determined. Patients. Adult patients (⬎18 yrs old) hospitalized with either community-acquired or nosocomial bacterial pneumonia were eligible for study entry if they met specific inclusion criteria. These criteria included presence of infiltrates on chest radiograph compatible with a diagnosis of bacterial pneumonia, confirmed by a positive culture of the blood, protected specimen brush, or bronchoalveolar lavage (for patients on ventilatory support ⱖ3 days). Patients had to have fever (temperature ⱖ38°C), tachypnea (⬎20 breaths/minute or need for mechanical ventilatory support), and tachycardia (heart rate ⬎90 beats/minute). In addition, patients had to have a diagnosis of pneumonia-induced severe sepsis by at least one of the following organ dysfunctions: sepsis-induced hypotension, acute respiratory distress syndrome, disseminated intravascular coagulation, acute oliguria, or lactic acidosis as defined in the protocol. Patients were not eligible for participation if they were pregnant or breastfeeding; had a life expectancy (unrelated to the acute infection) of ⬍72 hrs, cardiogenic shock as the primary acute condition, uncontrolled hemorrhage, or the presence of full-thickness thermal or chemical burns (⬎20% of body surface); had a white blood cell count ⬎40 ⫻ 109 cells/L, had history of New York Heart Association class IV heart failure; had do-notresuscitate orders, or had known hypersensitivity to Escherichia coli-derived products. 368 Treatment. Filgrastim (300 g/day) or placebo (vehicle in an identical vial) (Amgen, Thousand Oaks, CA) were administered as a 30-min intravenous infusion for 5 days, until the white blood cell count was ⬎75 ⫻ 109/L, or until the day intravenous antibiotics were discontinued, whichever came first. The study drug was administered as soon as possible and within 24 hrs of meeting criteria for severe sepsis and within 4 hrs of randomization. Subsequent doses were given at 24-hr intervals after the first dose and within 5 hrs after the results of a white blood cell count were known. Supportive Care and Monitoring. Full supportive care was given as required. Concomitant medications, including antibiotics, were administered as medically indicated by the treating clinicians. Baseline assessments included clinical evaluation (vital signs, Acute Physiology and Chronic Health Evaluation II score, electrocardiogram, chest radiograph, arterial blood gases, and sputum and blood cultures). During the course of the study, vital signs and complete blood counts were recorded daily, and patients were monitored for organ dysfunction, adverse events, concomitant medications, blood transfusions, and procedures. Chest radiographs, arterial blood gases, and other blood panels were done as clinically indicted. Study End Points and Sample Size. The primary efficacy end point was the occurrence of mortality through day 29. Secondary efficacy end points included occurrence of subsequent end-organ dysfunction through day 10, days on mechanical ventilatory support through day 29, time to death, and time to an intensive care unit discharge. The safety end points were the occurrence of adverse events through day 10, changes from baseline in laboratory parameters, and mortality through day 29. A sample size of 700 patients was calculated to provide 80% power to detect a reduction in 28-day mortality from 35% in the placebo group to 25% in the filgrastim-treated group. The estimated placebo rate was based on the observed mortality rates in the sample populations with severe sepsis enrolled in previous Amgen-sponsored studies as well as the published literature. Statistical Methods. The proportions of deaths occurring on or before day 29 and the proportion of patients with new end-organ dysfunction on or before day 10 were compared using the Cochran-Mantel-Haenszel test with stratification by center. A center-pooling algorithm was devised in which centers were pooled to ensure that each pooled center had at least one patient on each treatment and at least one experiencing each outcome. Kaplan-Meier estimates of the distributions of survival time and time to intensive care unit discharge were compared between treatment groups with the log-rank test, and days on mechanical ventilatory support were compared with the Wilcoxon’s rank-sum test. Adverse events were tabulated by body system, severity, and relationship to study drug. No interim analysis was planned, and none was performed. RESULTS Patients From April 1996 through December 1998, 701 patients from 96 hospital centers in the United States, Canada, Australia, and Europe were enrolled in this study and randomized to receive filgrastim (n ⫽ 348) or placebo (n ⫽ 353). Forty-four patients (6.3% of all patients) did not complete the study for reasons other than death. The two study groups were balanced in terms of age, sex, race, and baseline comorbid medical disorders, including vital signs and blood gases (Table 1). All patients who participated in this study presented with either community-acquired pneumonia (80%) or nosocomial pneumonia (20%); the distribution was approximately equal in both groups. A blood culture was performed at baseline for 672 patients (96%) (Table 2), and a respiratory secretion culture was performed at baseline for 625 patients (89%) (Table 3). Twenty-nine percent of the patients were bacteremic, with Streptococcus pneumoniae and Staphylococcus aureus the most frequently found pathogens. Drug Administration and Responses A total of 699 patients received at least one dose of study drug and were evaluable for safety. Two patients died before receiving study drug (one in each group). Eighty-four percent of all patients received the complete 5-day course of study drug. The median highest white blood cell count (i.e., the median of the highest individual patient values) was 19.3 ⫻ 109 cells/L in the placebo group and 31.7 ⫻ 109 cells/L in the filgrastim group (Fig. 1). The median time to each peak white blood cell count was 9 days in the placebo group and 4 days in the filgrastim group. Once filgrastim therapy was discontinued, the white blood cell count returned to baseline, usually within 3 days. The most frequently prescribed antibiotics were third-generation cephalosporins (64% to 66%), followed by macrolides (53% to 56%), and aminoglycosides (40% to 44%). This usage is consistent Crit Care Med 2003 Vol. 31, No. 2 Table 1. Summary of key demographic and baseline characteristics and risk factors in patients with pneumonia and severe sepsis Placebo (n ⫽ 353) Filgrastim (n ⫽ 348) 60.0 (16.4) 19–93 58.9 (17.1) 16–93 with the broad-spectrum coverage administered to patients with severe pneumonia. Study End Points Age, yrs, mean (SD) Age range, yrs Sex, n (%) Men Women Risk factors, n (%) Anemia Diabetes mellitus COPD Current alcohol abuse Current smoker Sepsis-induced hypertension ARDSa DIC Acute oliguria Lactic acidosis Pulse, beats/min, mean (SD) Respiratory rate, breaths/min, mean (SD) APACHE II score, mean (SD) White blood cell count (⫻109/L), median 247 106 (70) (30) 240 108 161 (46) 71 (20) 130 (37) 99 (28) 146 (41) 239 (68) 83 (24) 20 (6) 117 (33) 87 (25) 131.9 (22.5) 33.7 (12.1) 24.2 (6.9) 12.4 (69) (31) 157 (45) 74 (21) 109 (31) 101 (29) 150 (43) 227 (65) 82 (24) 19 (5) 107 (31) 104 (30) 133.6 (22.7) 33.3 (11.2) 24.3 (7.5) 12.3 COPD, chronic obstructive pulmonary disease; ARDS, acute respiratory distress syndrome; DIC, disseminated intravascular coagulation; APACHE, Acute Physiology and Chronic Health Evaluation. a ARDS is defined as (in the absence of overt cardiac disease): PAO2/FIO2 ratio ⱕ200; diffuse bilateral infiltrates on chest radiograph; requirement for mechanical ventilation with positive end-expiratory pressure ⱖ5; pulmonary artery occlusion pressure ⬍19 mm Hg if a pulmonary artery catheter was in place. The diagnosis of protocol-defined ARDS was made on the day all four criteria were met. Table 2. Most frequently reported respiratory pathogens in baseline blood cultures Streptococcus pneumoniae Staphylococcus aureus Escherichia coli Pseudomonas aeruginosa Staphylococcus species Streptococcus group A Placebo (n ⫽ 353) Filgrastim (n ⫽ 348) 70 (20.5) 21 (6.1) 13 (3.8) 9 (2.6) 8 (2.3) 3 (0.8) 60 (18.1) 16 (4.8) 5 (1.5) 2 (0.6) 2 (0.6) 4 (1.2) Given as number (percent). Table 3. Most frequently reported respiratory pathogens in baseline sputum cultures Streptococcus pneumoniae Staphylococcus aureus Haemophilus influenzae Pseudomonas aeruginosa Escherichia coli Klebsiella pneumoniae Streptococcus beta hemolytic Neisseria species Moraxella catarrhalis Enterobacter cloacae Serratia marcescens Enterobacter aerogenes Streptococcus group B Staphylococcus species Proteus mirabilis Given as number (percent). Crit Care Med 2003 Vol. 31, No. 2 Placebo (n ⫽ 353) Filgrastim (n ⫽ 348) 76 (23.8) 74 (23.2) 39 (12.2) 24 (7.5) 21 (6.6) 11 (3.4) 10 (3.1) 8 (2.5) 7 (2.2) 6 (1.8) 6 (1.8) 6 (1.8) 5 (1.5) 4 (1.2) 4 (1.2) 70 (22.8) 55 (17.9) 29 (9.4) 23 (7.4) 15 (4.8) 15 (4.8) 6 (1.9) 2 (0.6) 6 (1.9) 6 (1.9) 5 (1.6) 3 (0.9) 4 (1.3) 8 (2.6) 3 (0.9) Efficacy End Points. A total of 191 patients died during the study, 90 in the placebo group and 101 in the filgrastim group. The occurrence of mortality through day 29 was 25.5% in the placebo group and 29.0% in the filgrastim group. This difference between the two groups was not statistically significant (p ⫽ .383, Cochran-Mantel-Haenszel test stratified by pooled center). In patients with community-acquired pneumonia, the mortality rates were 24% (placebo) and 28% (filgrastim) compared with patients with nosocomial pneumonia with 31% (placebo) and 33% (filgrastim), respectively. These rates were not significantly different for the filgrastim and placebo groups in either form of severe pneumonia. The median time to death was ⬎28 days for both the placebo and filgrastim groups (Fig. 2). The distributions were not significantly different between the treatment groups (p ⫽ .261, log-rank test). Each covariate effect was significant: age (p ⫽ .0001), number of endorgan dysfunctions (p ⫽ .0001), bacteremia (p ⫽ .0157), and Acute Physiology and Chronic Health Evaluation II Score (p ⫽ .0004). The overall occurrence of new endorgan dysfunctions was 40.0% in the placebo group and 42.6% in the filgrastim group (p ⫽ .524 according to CochranMantel-Haenszel test stratified by pooled center). Among antibiotics administered during the study, only the use of quinolones in the filgrastim-treated group showed a strong trend toward reduced 28-day mortality. With any use of quinolones from day 1 to day 5, there was 40% mortality in quinolone-placebo group (31/78) compared with 29% mortality in the quinolone-filgrastim group (18/62; p ⫽ .187; 95% confidence interval, 0.45– 1.18). This represented an absolute decrease in mortality of 11% and a relative risk of .73 (a 27% rate reduction). No other trends were noted for other antibiotics between the placebo and filgrastimtreated groups. A total of 686 patients (98%) were in an intensive care unit at study entry (placebo: n ⫽ 345, 97.7%; filgrastim: n ⫽ 341, 97.9%). The median time to intensive care unit discharge was 12 days in both groups (Fig. 3). The distributions 369 Figure 1. White blood cell response as median white blood cell count by study day. Median peak white blood cell count was 19.3 ⫻ 109 cells/L for placebo and 31.7 ⫻ 109 cells/L for filgrastim. Median study day of peak white blood cell count was day 9 for placebo (open circles) and day 4 for filgrastim (filled circles). The number of patients per treatment group per day is given at bottom of figure. were not statistically significantly different between the treatment groups (p ⫽ .780, log-rank test). No statistically significant difference was noted in days on mechanical ventilatory support (9.3 days in the placebo group and 9.6 days in the filgrastim-treated group; p ⫽ .835, logrank test). Safety End Points. A total of 2,517 adverse events were reported among 336 (95%) evaluable patients receiving placebo, and 2,484 adverse events were reported among 338 (97%) evaluable patients receiving filgrastim. Adverse events were generally similar in type and frequency between the two treatment groups. Severe adverse events were comparable between the two treatment groups: 128 (36%) patients in the placebo group and 137 (39%) patients in the filgrastim group had severe or life-threatening adverse events. The most frequent severe or life-threatening adverse events reported with at least a 2% difference in frequency between the two treatment groups were renal insufficiency, acute respiratory distress syndrome, hypotension, cardiac arrest, and acidosis. No clinically significant effect of filgrastim on laboratory values (other than white blood cell count) was observed. Filgrastim appeared to be safe and well tolerated when administered to 347 patients with pneumonia and severe sepsis. DISCUSSION Figure 2. Kaplan-Meier plot and log-rank test for time to death (expressed as percentage of patients surviving). Log-rank test, 1.262; p ⫽ .261. Open circles, placebo (n ⫽ 353); filled circles, filgrastim (n ⫽ 348). Figure 3. Kaplan-Meier plot and log-rank test for time to intensive care unit discharge (expressed as percentage of patients remaining in the intensive care unit). Log-rank test, 0.078; p ⫽ .789. Open circles, placebo (n ⫽ 345); filled circles, filgrastim (n ⫽ 341). 370 Nosocomial pneumonia is frequently a fatal complication in hospitalized patients, particularly those who require mechanical ventilatory support for their medical problems (8, 9), and communityacquired pneumonia is a major health problem in Western Europe and North America. In the United States, pneumonia is the leading cause of death from an infectious disease and the sixth highest cause of mortality from any cause (10). Mortality rates are particularly high in elderly patients with community-acquired pneumonia of any etiology, even if not complicated by bacteremia (11). Younger patients with pneumococcal pneumonia and sepsis also suffer high mortalities, usually in excess of 20% (12). Improved therapeutic strategies are needed for patients who are severely ill with pneumonia and sepsis. A study that is focused on bacterial pneumonia with strict case definitions and entry criteria has the virtue of less heterogeneity of the Crit Care Med 2003 Vol. 31, No. 2 study patients and fewer microbial etiologies to be covered by antimicrobial treatment. This contrasts with the many published studies of severe sepsis in which at least 10% of the patients had no identifiable source or etiology for sepsis and may not have had infection as the cause of the systemic inflammatory response (13). This study was conducted to determine whether filgrastim, when added to a course of intravenous antibiotics and other standard management strategies, would reduce the rate of mortality in hospitalized patients with severe pneumonia and sepsis. Filgrastim administration increased white blood cell counts to a median peak of 31.7 ⫻ 109 cells/L from a baseline of 12.3 ⫻ 109 cells/L, and were significantly higher than in the placebo group. Although the study drug was administered in a blinded fashion, this increase in white blood cell count could be considered to limit the blinding of the study. Because the outcome was not different between the two groups, this study-design limitation is negligible. The median age, nature and prevalence of comorbid conditions, severity of illness, rates of bacteremia, prevalence of organ failures, and the need for supportive mechanical ventilatory support at study entry were well balanced and similar to data from other published large studies (8, 14). Mortality, the primary efficacy end point, was not significantly different between the placebo and filgrastim groups, regardless of whether the cause was community-acquired pneumonia or nosocomial pneumonia. In addition, no significant between-group differences were found for the secondary efficacy end points, including the occurrence of endorgan dysfunction, days on mechanical ventilatory support, time to death, and time to intensive care unit discharge. Severe adverse events were comparable between the two study groups. Acute respiratory distress syndrome was not unexpected in this patient population, and its frequency was within historical norms in both groups. Acute respiratory distress syndrome was reported in 41 (12%) patients in the placebo group and 56 (16%) patients in the filgrastimtreated group. A number of reasons are possible for this failure to detect any clinical benefit from adjunctive filgrastim treatment of a severe infection in which phagocytes are paramount in host defense. These might include faulty validity of the underlying Crit Care Med 2003 Vol. 31, No. 2 hypothesis, inadequate dosage or biological activity of exogenously administered G-CSF, improper study design, or failed execution. It is known that the amount of circulating endogenous G-CSF increases rapidly in patients with bacterial infections, and most evidence supports a primary role for this growth factor in generating the neutrophilic leukocytosis in such patients (15). Particularly high levels of endogenous G-CSF have been reported in patients with sepsis and septic shock; these paralleled similar elevations in interleukin-6 and leukemia inhibitor factor (16). The prompt and significant elevation of absolute neutrophil count in the filgrastim recipients in this present study indicates that the dosage chosen had appreciable biological activity, although a lack of augmentation of other known phagocytic activities in the setting of severe sepsis cannot be excluded (17). The choice of the antibiotic therapy that is paired with filgrastim administration may be important for optimizing favorable anti-infective interactions in these severely ill patients with sepsis arising from the lungs. As a class, quinolones exhibit excellent tissue and cell penetration compared with -lactams (18). In addition, filgrastim has been reported to increase the intracellular uptake by neutrophils of some antibiotics, including ciprofloxacin (19). Our results indicate that patients receiving filgrastim and antibiotic therapy that included a quinolone for their initial treatment showed a strong trend toward decreased mortality. It is conceivable that if quinolones had been used more broadly, the increased numbers of patients treated may have been sufficient for a statistically significant result. Regarding the study design, the timing of the administration of filgrastim may have been too late in the course to alter the clinical outcome of these severely ill patients. In nearly all the preclinical studies of challenge models with bacteria or bacterial endotoxin, filgrastim was most beneficial when given either simultaneously with or before the infectious agent or endotoxin. Much less benefit was observed when filgrastim administration was delayed until well after initiation of the experimental infection (5). In the published clinical studies of filgrastim as an adjunct in the management of bacterial infections, beneficial results were most consistently observed when filgrastim was given as prophylaxis D elaying the administration of filgrastim to pa- tients with severe infection until a time that is well after initiation of antimicrobial treatment and the development of organ failures and systemic immunosuppression may provide little additional anti-infective benefit and is unlikely to restore systemic immunity. to patients at high risk to develop postoperative pneumonia or soft-tissue infections (20, 21) or when administered early in the management of nonseptic diabetic patients with localized soft-tissue infection (22). In a prospective, placebocontrolled trial of filgrastim in patients with bacterial pneumonia, only patients with multilobar disease without severe sepsis or multiple organ failures exhibited a strong trend toward reduced mortality (6). After this study was designed, additional knowledge emerged about the nature of the dynamic balance between systemic inflammatory and counterinflammatory mediators that evolves during the course of severe sepsis. Although the initial systemic responses to severe infection are accompanied by sharp increases in circulating inflammatory mediators, later in the course, the balance characteristically shifts toward the anti-inflammatory and immunosuppressive spectrum (23–25). In fact, the degree of increase in plasma concentrations of a variety of endogenous antiinflammatory mediators correlates strongly with adverse outcomes (26, 27). Furthermore, the extent of systemic immunosuppression, as measured by the reduced expression of human leukocyte antigen-DR on circulating mononuclear cells, also correlates directly with poor outcomes (28). 371 Several cytokines and growth factors, including G-CSF, appear to have a key role in the host’s attempts to restore systemic homeostasis in severe sepsis. In so doing, their systemic functions may be quite different from their actions at local sites of infection (29 –31). The initial responses at the local infection site are predominantly inflammatory and devoted to eliminating the offending pathogens. In contrast, the early systemic responses are usually anti-inflammatory and focus on restricting some of the damaging systemic consequences of severe local infection (32). With respect to G-CSF, its enhanced production in response to an infectious challenge is critical for recruiting and optimizing phagocytic activity at local sites, which are involved in the removal of offending pathogens (15, 17, 32). Conversely, the major systemic effects of G-CSF are both anti-inflammatory and immunosuppressive and appear to be focused on inhibition of the production and actions of inflammatory cytokines, as well as in expanding a T-helper lymphocyte response that might eventually lead to the production of specific antibodies to neutralize microbial pathogenic factors (31, 33–35). 2. 3. 4. 5. 6. 7. 8. 9. CONCLUSIONS Delaying the administration of filgrastim to patients with severe infection until a time that is well after initiation of antimicrobial treatment and the development of organ failures and systemic immunosuppression may provide little additional anti-infective benefit and is unlikely to restore systemic immunity. Further studies using these principles to explore the timing and ability of filgrastim to ameliorate or prevent the consequences of severe bacterial infection will be of great interest. 10. 11. 12. 13. ACKNOWLEDGMENTS We thank David Dale, MD, and Thomas Martin, MD, for helpful discussions and suggestions. Mitzi Armstrong, Naree Sukumoijia,; and the G-ID Clinical Study Management Team at Amgen were instrumental in the completion of this study. MaryAnn Foote, PhD, assisted with the writing of this manuscript. 14. 15. 16. REFERENCES 1. Angus DC, Linde-Zwirble WT, Lidicker J, et al: Epidemiology of severe sepsis in the United States: Analysis of incidence, out- 372 come, and associated costs of care. Crit Care Med 2001; 29:1303–1310 Zeni F, Freeman B, Natanson C: Antiinflammatory therapies to treat sepsis and septic shock: A reassessment. Crit Care Med 1997; 25:1095–1100 Wheeler AP, Bernard GR: Treating patients with severe sepsis. N Engl J Med 1999; 340: 207–214 Marston BJ, Plouffe JF, File TM Jr, et al: Incidence of community-acquired pneumonia requiring hospitalization: Results of a population-based active surveillance study in Ohio. The Community-Based Pneumonia Incidence Study Group. Arch Intern Med 1997; 157:1709 –1718 Nelson S: A question of balance. Am J Respir Crit Care Med 1999; 159:1365–1367 Nelson S, Belknap SM, Carlson RW, et al: A randomized controlled trial of Filgrastim as an adjunct to antibiotics for treatment of hospitalized patients with communityacquired pneumonia. J Infect Dis 1998; 8:1075–1080 Wunderink RG, Leeper KV, Schein RM, et al: Filgrastim in patients with pneumonia and severe sepsis or septic shock. Chest 2001; 119:523–529 Torres A, Aznar R, Gatell JM, et al: Incidence, risk, and prognostic factors of nosocomial pneumonia in mechanically ventilated patients. Am Rev Resp Dis 1990; 142:523–528 Richards MJ, Edwards JR, Culver DH, et al: Nosocomial infections in medical-surgical intensive care units in the United States. Infect Control Hosp Epidemiol 2000; 21: 510 –515 National Center for Health Statistics: Vital Statistics of the United States. 119th Edition. Washington, DC, U.S. Census Bureau Statistical Abstract of the United States, 1999, pp 99 Marrie TJ: Community-acquired pneumonia in the elderly. Clin Infect Dis 2000; 31: 1066 –1078 Feikin DR, Schuchat A, Kolczak M, et al: Mortality from invasive pneumococcal pneumonia in the era of antibiotic resistance 1995–1997. Am J Public Health 2000; 90: 223–239 Cohen J, Guyatt G, Bernard GR, et al: New strategies for clinical trials in patients with sepsis and septic shock. Crit Care Med 2001; 29:880 – 886 Ruiz M, Ewig S, Torres M, et al: Severe community-acquired pneumonia: Risk factors and follow-up epidemiology. Am J Respir Crit Care Med 1999; 160:923–929 Dale DC, Liles WC, Summer WR, et al: Review: Granulocyte colony-stimulating factor role and relationships in infectious diseases. J Infect Dis 1995; 172:1061–1075 Presneill JJ, Waring PM, Layton JE, et al: Plasma granulocyte colony-stimulating factor and granulocyte-macrophage colonystimulating factor levels in critical illness, including sepsis and septic shock: Relation to disease severity, multiple organ dysfunction, 17. 18. 19. 20. 21. 22. 23. 24. 25. 26. 27. 28. 29. 30. 31. 32. and mortality. Crit Care Med 2000; 28: 2344 –2354 Root RK, Dale DC: Granulocyte colonystimulating factor and granulocyte-macrophage colony-stimulating factor: Comparisons and potential for use in the treatment of infections in nonneutropenic patients. J Infect Dis 1999; 179:S342–S352 Moellering RC Jr: The place of quinolones in everyday clinical practice. Chemotherapy 1996; 42:54 – 61 McKenna PH, Nelson S, Andreson J: Filgrastim enhances ciprofloxacin uptake and bactericidal activity of human neutrophils in vitro. Abstr. Am J Crit Care Med 1996; 153S: A535 Schafer H, Hubel K, Bohlen H, et al: Perioperative treatment with filgrastim stimulates granulocyte function and reduces infectious complications after esophagectomy. Ann Hematol 2000; 79:143–151 Wenisch C, Werkgartner T, Sailer H, et al: Effect of preoperative prophylaxis with filgrastim in cancer neck dissection. Eur J Clin Invest 2000; 30:460 – 466 Gough A, Clapperton M, Rolando N, et al: Randomised placebo-controlled trial of granulocyte-colony stimulating factor in diabetic foot infection. Lancet 1997; 350:855– 859 Bone RC, Grodzin CJ, Balk RA: Sepsis: A new hypothesis for pathogenesis of the disease process. Chest 1997; 112:235–243 Dinarello CA: Proinflammatory and antiinflammatory cytokines as mediators in the pathogenesis of septic shock. Chest 1997; 112:321S–329S Rangel-Frausto SM, Pittet D, Hwang T, et al: The dynamics of disease progression in sepsis: Markov modeling describing the natural history and likely impact of effective antisepsis agents. Clin Infect Dis 1998; 27:185–190 Wray GM, Hinds CJ: Determinants of outcome from sepsis and septic shock. In: Yearbook of Intensive Care and Emergency Medicine. Vincent JL (Ed). Berlin, SpringerVerlag, 1997, pp 168 –179 Gogos C, Drosou E, Bassarus HP, et al: Proversus anti-inflammatory cytokine profile in patients with severe sepsis: A marker for prognosis and future therapeutic options. J Infect Dis 2000; 181:176 –180 Docke WD, Randow F, Syrbe U, et al: Monocyte deactivation in septic patients: Restoration by IFN-␥ treatment. Nat Med 1997; 3:678 – 681 van der Poll T, van Deventer SJ: Cytokines and anticytokines in the pathogenesis of sepsis. Infect Dis Clin North Am 1999; 13: 413– 426 Munford RS, Pugin J: The crucial role of systemic responses in the innate (nonadaptive) host defense. J Endotoxin Res 2001; 7:327–332 Hartung T, Docke WD, Handschuh DS, et al: Effect of filgrastim treatment on inflammatory cytokines and lymphocyte functions. Clin Pharmacol Ther 1999; 66:415– 424, Zhang P, Summer WR, Bagby GJ, et al: In- Crit Care Med 2003 Vol. 31, No. 2 nate immunity and pulmonary host defense. Immunol Rev 2000; 173:39 –51 33. Boneberg EM, Hareng L, Gantner F, et al: Human monocytes express functional receptors for granulocyte colony-stimulating factor that mediate suppression of monokines and interferon-␥. Blood 2000; 95:270 –276 34. Sloand EM, Kim S, Maciejewski JP, et al: Pharmacologic doses of granulocyte colonystimulating factor affect cytokine production by lymphocytes in vitro and in vivo. Blood 2000; 95:2269 –2274 35. Arpinati M, Green CL, Heimfeld S, et al: Granulocyte colony-stimulating factor mobilizes T helper 2-inducing dendritic cells. Blood 2000; 95:2484 –2490 APPENDIX Additional Members of the Pneumonia Sepsis Study Group Antonio Anzueto, Audie Murphy Memorial VA Hospital, San Antonio, TX; Mark Astiz, St. Vincent’s Hospital, New York, NY; Robert Balk, Rush Presbyterian Hospital, Chicago, IL; Robert Baughman, University of Cincinnati Hospital, Cincinnati, OH; Steven Belknap, St. Francis Medical Center, Peoria, IL; David Bihari, The St. George Hospital, Kogarah, Australia; Bonnie V. Bock, Private practice, Newport Beach, CA; Raymond Bracis, Halliday Medical Center, Portland, OR; Jonathan Burdon, St. Vincent’s Hospital, Fitzroy, Australia; Richard Carlson, Maricopa Medical Center, Phoenix, AZ; Jean Chastre, Hopital Bichat, Paris, France; Nathan Clumeck, Hopital St. Pierre, Brussels, Belgium; Lynell Collins, VA Medical Center, Louisville, KY; Richard Corbin, Carolinas Medical Center, Charlotte, NC; Gerald Criner, Temple Univer- Crit Care Med 2003 Vol. 31, No. 2 sity Hospital, Philadelphia, PA; Anthony Dal Nogare, University of Texas Southwest Medical Center, Dallas, TX; Jane Dematte-D’Amico, Columbia Michael Reese Hospital, Chicago, IL; Geoffrey Dobb, Royal Perth Hospital, Perth, Australia; David Dworzack, St. Joseph’s Hospital, Omaha, NE; Jean-Yves Fagon, Hopital Broussais, Paris, France; Harrison Farber, Boston Medical Center, Boston, MA; Stanley Fiel, MCP Hahnemann University, Philadelphia, PA; Simon Finfer, Royal North Shore Hospital, St. Leonards, Australia; Eugene Fletcher, University of Louisville Hospital, Louisville, KY; Marilyn Foreman, Moorehous School of Medicine, Atlanta, GA; Philip Fracica, St. Joseph’s Hospital, Phoenix, AZ; Brad Freeman, Washington University, St. Louis, MO; Barry Fuchs, Allegheny University Hospital, Philadelphia, PA; David Gelmont, LAC/USC Medical Center, Los Angeles, CA; Jonathan Gottlieb, Jefferson Medical College, Philadelphia, PA; Benoit Guery, Hopital de Tourcoing, Tourcoing, France; Jeffrey Hasday, University of Maryland School of Medicine, Baltimore, MD; Daren Heyland, Kingston General Hospital, Kingston, Canada; Hoi Ho, Texas Tech University Hospital, El Paso, TX; Andrew Holt, Flinders Medical Centre, Bedford Park, Australia; Donald Howard, Wilford Hall Medical Center, Lackland AFB, TX; William E. Hurford, Massachusetts General Hospital, Boston, MA; Luc Huyghens, A Z V U B, Brussels, Belgium; Robert C. Hyzy, Henry Ford Hospital, Detroit, MI; David Ingbar, University of Minnesota, Minneapolis, MN; Monroe Karetzky, Newark Beth Israel, Newark, NJ; Kim M. Kerr, UCSD Medical Center, San Diego, CA; Gary Kinasewitz, VA Medical Center, Oklahoma City, OK; James A. Kruse, Detroit Receiving Hospital, Detroit, MI; Stephen Lapinsky, Mt. Sinai Hospital, Toronto, Canada; Michael Littner, VA Medical Center, Sepulvada, CA; C. Kees Mahutte, VA Medical Center, Long Beach, CA; John Marshall, Toronto General Hospital, Toronto, Canada; George Matuschak, St. Louis University, St. Louis, MO; C. David Mazer, St. Michael’s Hospital, Toronto, Canada; Alan Multz, Long Island Jewish Hospital, New Hyde Park, NY; Erling Myhre, Lund University Hospital, Lund, Sweden; Karim Nazer, Danbury Hospital, Danbury, CT; Mary Therese, O’Donnell INOVA Health Systems, Falls Church, VA; Dan E. Olson, Medical College of Ohio, Toledo OH; Lucy Palmer, SUNY at Stony Brook, Stony Brook, NY; Martin Phillips, Sir Charles Gairdner Hospital, Nedlands, Australia; Susan Pingleton, University of Kansas Medical Center, Kansas City, KS; Robert Reynolds, PW Clinical Research, Asheville, NC; Mark Rumbak, Tampa General Hospital, Tampa, FL; Raffaele Schicchitano, Royal Adelaide Hospital, Adelaide, Australia; Terry Smith, Sunnybrook Health Sciences Center, North York, Canada; Guy Soo Hoo, VA Medical Center, Los Angeles, CA; Susan Stein, VA Medical Center, Sepulvada, CA; James Tan, Akron City Hospital, Akron, OH; Brian White, Comprehensive Research Services, Mogadore, OH; John Wilson, The Alfred Healthcare Group, Phahran, Australia; Richard Wunderink, Methodist Healthcare, Memphis, TN; Iven Young, Royal Prince Alfred Hospital, Camperdown, Australia; Marcus Zervos, William Beaumont Hospital, Royal Oak, MI 373