Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
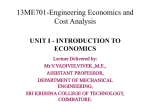
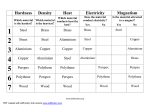
Clinical Science (1991) 81,289-295 289 Editorial Review Aluminium: gastrointestinal absorption and renal excretion C. J. LOTE AND H. SAUNDERS Department of Physiology,The Medical School, University of Birmingham, Birmingham, U.K. INTRODUCTION. SOURCES ABILITY OF ALUMINIUM AND BIOAVAIL- Aluminium is the most abundant metal and constitutes 8% of the earth’s crust. It is a normal constituent of vegetable and animal tissues and is present in raw untreated water. In domestic tap-water supplies, aluminium may be present in high concentrations either from its presence in raw water or, more commonly, as a result of its use during the water-purification process. Aluminium in the metallic form is widely used for both industrial and domestic purposes, and a variety of aluminium salts are used in foods, fluids, cosmetics and medications. The toxicity of aluminium in patients with renal failure is now well documented, and dialysis encephalopathy, osteomalacia and anaemia are recognized hazards in such patients if aluminium is not excluded from dialysis fluids and medications. The safe levels of aluminium in food, water, medications and infusion fluids for subjects with normal renal function are unknown, but aluminium has been implicated as causative agent in a number of dementia diseases, including Alzheimer’s disease. There are a number of recent reviews of aluminium toxicity [l-51. In contrast to these, in the present review, we concentrate on the mechanisms of absorption and excretion of aluminium, rather than the consequences of aluminium deposition in the body. The normal dietary source of aluminium is food and water to which aluminium has been added or in which there is naturally a high content [6,7]. The normal daily intake of aluminium is estimated to be approximately 9 mg/day in teenage and adult females and 12-14 mg/day in teenage and adult males [7]. However, it has been stated that “the inappropriate choice of foods, methods of food preparation and non-prescription drugs can readily increase the daily intake of aluminium to several thousand mg each day” [8]. Such high aluminium intakes are particularly likely in Correspondence: Dr C. J. Lote, Department of Physiology, The Medical School, University of Birmingham, Birmingham B15 2TT, U.K. individuals who ingest aluminium-containing drugs as antacids or phosphate-binders. Tea leaves contain relatively large amounts of aluminium, since tea plants accumulate aluminium from the soil [9]. Koch el al. [lo] reported “that at least some of the aluminium present in tea is absorbed and that tea consumption must be considered in any assessment of the total dietary intake of aluminium in human beings”. However, tannin, also present in tea, is an inhibitor of gastrointestinal aluminium absorption [loa], and hence the bioavailability of the aluminium in tea is relatively low. Aluminium salts have a number of functions when used as food additives [8]. For example, the acidic forms of sodium aluminium phosphate are added to commercial cake mixes and self-raising flour as E541, where they act as leavening agents in reaction with sodium bicarbonate. The alkaline forms of these aluminium salts are added to processed cheeses as emulsifying agents. Another source of aluminium is baby-milk powder. Freundlich et al. [l11reported that the aluminium content of a variety of milk powders that they analysed ranged from 124 to 351 pg/l, although values as high as 2346 pg/l have been reported in highly processed and modified milk powders [12]. The aluminium content of normal breast milk is 2-10 pg/l. Koo el al. [12] proposed that aluminium contamination of baby-milk powders was due to the use of raw materials such as soya bean, additives (for example calcium and phosphorus), manufacturing processes and the type of storage container. The aluminium contpt of domestic water supplies is recognized as a potential major source of exposure for this metal ion in patients with chronic renal failure, since dialysis fluids may contain aluminium, and such patients may also be taking oral aluminium-containing drugs as phosphate-binders. The critical concentration of aluminium in dialysis fluid (above which there will be a significant net transfer of aluminium to the patient) is a matter of some debate, but ranges from about 14 ,ug/l[13] to 27 pg/l [ 141; ideally, the dialysate aluminium concentration should be well below this. An epidemiological survey of haemodialysis patients, indicated that those who were C. J. Lote and H. Saunders 290 receiving haemodialysis therapy using water with an aluminium content greater than 50 pg/l had an increased incidence of both fracturing osteodystrophy and dialysis encephalopathy [ 151. During a single haemodialysis session with such a high aluminium concentration in the water, up to 100 mg of aluminium could be transferred to the patient. In normal subjects, drinking about 2 litres of water/day, it is unlikely that more than about 2 mg of aluminium would be ingested, only a proportion of which is absorbed (see below). Nevertheless, a recent epidemiological survey [16] has indicated a link between the aluminium content of drinking water and the prevalence of Alzheimer’s disease, although it should be mentioned that the risk of Alzheimer’s disease was only 1.5 times higher in districts where the mean aluminium concentration in drinking water was high ( > 0.11 mg/l) than in districts where the aluminium concentration was low ( < 0.01 mg/l), and the data were adjusted to take account of differences in diagnostic rate of Alzheimer’s disease with distance from a computed tomography scanning unit. GASTROINTESTINAL MINIUM ABSORPTION OF ALU- The gastrointestinal tract is a major cellular barrier to aluminium absorption, and, furthermore, most naturally occurring aluminium compounds are highly insoluble. The normal daily aluminium uptake from food and drinking water is approximately 10 mg. That gastrointestinal absorption of aluminium does occur is clearly demonstrated by the fact that both plasma aluminium coacentration and urinary aluminium excretion are increased after high oral doses (i.e. greater than 10 mg/kg body weight) of aluminium (for example, [17-211). Wilhelm et al. [5] have recently surveyed the data in the literature on gastrointestinal absorption of aluminium, and it is clear that the methodology employed to assess gastrointestinal absorption can have a major bearing on the interpretation of the findings. Aluminium absorption from the intestinal lumen is initially into the intestinal mucosal cells, and only a small proportion of this uptake continues into the blood [22]. The aluminium in the mucosal cells is subsequently excreted in the faeces when the cells desquamate. Consequently, balance studies (where aluminium uptake is determined as intake minus faecal elimination and urinary excretion) tend to overestimate uptake. Absorbed aluminium is primarily excreted in the urine, but the urinary excretion of aluminium is not an infallible guide to absorption because aluminium may accumulate in body tissues, and a very minor fraction is excreted in the bile [20-241. This biliary excretion (0.1% of total aluminium-polyoxo complexes at pH values over 4, but insufficiency [25]. Factors affecting aluminium absorption The details of the mechanism of aluminium absorption remain unclear. The factors which influence aluminium absorption are listed in Table 1, and provide clues to the physiological processes involved. Physicochemical factors. The solubility of aluminium salts in aqueous solution is complex, and is influenced by pH and by other ionic species [26]. In acidic solutions (below pH 4), aluminium in solution is found as A1(H20)63+,often written in an abbreviated form simply as A13+.This A1(H20)63+ can form colloidal aluminium-polyoxo complexes at pH values over 4, but these redissolve if the pH is lowered or raised, since in alkaline solutions aluminium is again soluble as AI(H0);. Free A13+ is decreased by the presence of phosphate, which forms insoluble salts. In contrast, citrate enhances the solubility of A13+, and at pH 2-5 a neutral soluble citrate-aluminium complex exists [26,27]. How d o the above facts relate to aluminium absorption? There is considerable evidence that citrate enhances the intestinal absorption of aluminium [29-321, and this effect is largely attributable to the formation of the soluble citrate-aluminium chelate. However, citrate may have additional effects on aluminium absorption, either by facilitating transcellular absorption or by opening the tight junction and enhancing the paracellular movement of aluminium [33]. Citrate is known to open epithelial tight junctions in cultured cells [34], and this finding has been supported by work on proximal (rat) jejunal segments in Ussing chambers [21]. The interactions of citrate with calcium are also likely to have effects on aluminium absorption. Calcium inhibits the absorption of aluminium, and thus more aluminium will be absorbed from water with a low calcium concentration. These observations suggest that the mechanism of aluminium uptake in the gut may share some features of the calcium absorption process [35, 361. In isolated rat jejunal slices, aluminium uptake was reduced by calciumchannel blockers and increased by calcium-channel activators [37]. These findings raise the possibility that the effects of citrate on aluminium absorption may involve calcium. Citrate is an effective chelator of calcium, and in the renal proximal tubule such complex formation inhibits citrate and calcium absorption [38]. In the gut, similar complexation of calcium with citrate may make calcium unavailable for absorption, thereby enhancing aluminium absorption. However, it is not entirely clear why citrate may inhibit calcium absorption but facilitate aluminium absorption. There are also antagonistic interactions between aluminium and fluoride absorption in the gut. Ingestion of aluminium hydroxide decreases the intestinal absorption of fluoride [39]. High aluminium and low fluoride concentrations in the water supply for dialysis patients increases the incidence of encephalopathy and bone fractures [40]. Related to these findings is the observation from an epidemiological study [41] that in areas where domestic tap water was highly fluorinated, there were fewer reported cases of Alzheimer’s disease compared with areas with low fluorinated water. Aluminium ( A P + ) forms strong complexes with F- [26]. The above findings Gastrointestinal absorption and renal excretion of aluminium 291 Table 1. Factors affecting aluminium absorption Effect on aluminium absorption Physical factors Citrate Silicic acid Iron Fluoride Physiological factors Pathophysiological factors Enhances Inhibition? ?(seethe text) Inhibition PH Calcium Changes from neutral enhance absorption? PTH Enhances Enhances 1,12-DihydroxyvitaminD, Uraemia imply that such complexes, if formed in the gut, are not readily absorbed. Silicic acid [Si(OH),] has a strong affinity for aluminium. A recent report has indicated that the silicic acid content of water has a major effect on the bioavailability of aluminium, with aluminium bioavailability decreasing with increasing silicic acid content [42]. The same authors suggest that this could occur in the gut as a result of the formation of hydroxy-aluminosilicates [43]. There is persuasive evidence that aluminium can substitute for iron in a number of sites in the body [44, 451, and several research groups have investigated the possibility that the mechanisms of iron absorption from the gut may be involved in aluminium absorption. The mucosal cells of the small intestine (primarily the duodenum) take up iron, and it is bound intracellularly to a protein, apoferritin, to form ferritin. Some of the iron enters the plasma where it is bound to the protein transferrin. Aluminium can be bound by both ferritin and transferrin. It is likely that the aluminium which binds to ferritin in the mucosal cells is largely not absorbed into the plasma, but remains bound and is eliminated from the body when the cells are shed into the intestinal lumen. Whether iron in the intestinal lumen influences aluminium absorption is a question which cannot be answered with certainty at present. Van der Voet & de Wolff [46] concluded that Fe2+ reduced aluminium absorption, whereas Fe3+ had no effect. Cannata et al. [47] proposed that the mechanism for intestinal absorption of aluminium might involve a ‘common pathway’ for metal ions including iron, since they found that iron uptake by ferritin prevented aluminium absorption. However, Blaehr et al. [48] found that iron in the intestine stimulates aluminium absorption. A variety of metal ions can bind to transferrin, but they do not bind to the ironbinding site. It may be that Fe2+has an allosteric effect on the transferrin molecule, preventing aluminium from fitting its binding site. The interrelationships between iron and aluminium absorption remain confused. There is also some evidence for a negative interaction between aluminium and sodium during intestinal absorption [49]. Physiological and pathophysiological factors. Parathyroid hormone (PTH) increases the gastrointestinal absorption of aluminium [50, 511; in patients with renal failure who were not on dialysis or receiving aluminium- Inhibition Enhances containing phosphate-binders, those patients who developed osteomalacia had high serum PTH levels (3.1 k 1.4 ng/ml compared with a normal value of less than 0.5 nglml), with the implication that this led to increased dietary aluminium absorption [52]. However, it is reported that in uraemic rats, in which gastrointestinal aluminium absorption is enhanced (see below), PTH does not further increase aluminium absorption [53]. In addition to the above reports of effects of PTH on aluminium absorption, there are also reports that aluminium depresses PTH release [54]. Burnatowska-Hledin et al. [55] have shown that 1,12dihydroxyvitamin D, increases the gastrointestinal absorption of aluminium, a finding which, like the PTH data above, supports the view that aluminium and calcium absorption may have related mechanisms. The kidneys are the main route of aluminium excretion, and consequently the gastrointestinal absorption of aluminium is of great importance in patients with compromised renal function. There is evidence that uraemia per se increases gastrointestinal absorption of aluminium in man and the rat [56, 571. Uraemic children also have an increased incidence of aluminium loading and toxicity [58],perhaps because they need large doses of phosphatebinders relative to body weight; and the effects of uraemia and citrate on aluminium absorption appear to be synergistic [21]. Fig. 1 illustrates the factors which influence gastrointestinal absorption of aluminium. Fate of absorbed aluminium What happens to the fraction of dietary aluminium which does enter the plasma? Aluminium binds to plasma proteins, mainly to the iron-binding protein transferrin and to albumin [44]. There are wide variations in the reported values for the extent of aluminium binding to protein: the range is 8% [59] to 98% [60]. Although the former of these studies was in man, and the latter in the rat, nevertheless species variation seems to be of minor importance. Much more important is the methodology used to assess binding. In general, the findings are based on ultrafiltration experiments. Gidden et al. [59] have demonstrated that the ultrafilterability of plasma aluminium depends on aluminium concentration, i.e. increasing the aluminium concentration decreases aluminium C. J. Lote and H. Saunders 292 Gut lumen ultrafilterability. This finding has been essentially confirmed in many other studies (for example, [20, 60-621). It is unlikely that the ultrafilterable fraction of plasma aluminium represents a single form of aluminium, since there are a number of low-M, binders of aluminium in plasma, including citrate, fluoride, phosphate, bicarbonate and silicates. Fig. 2 shows some of the effects of absorbed aluminium. Duodenal cells Aluminium 0Inorganic Organic relatively insoluble A13+ absorption t 1 1 RENAL EXCRETION OF ALUMINIUM Enhanced by: 1,12-Dihydroxyvitamin D, 1 t 1 I I Inhibited by: calcium tannin fluoride Complex with iron-binding Return to gut lumen when cells 1 , sloughed off Faecal excretion Fig. 1. Gastrointestinal absorption of aluminium. Urinary aluminium excretion increases after oral aluminium loading in subjects with normal renal function [63].The M , cut-off of the renal glomerular filter is 70 000 (e.g. [64]).Consequently, transferrin ( M , 77 000), the main aluminium-binding protein in plasma, is not filtered. Hence it is likely that only a small fraction of plasma aluminium will be filterable, although as the preceding section indicates, this fraction will be variable, depending on the plasma concentration of aluminium. The aluminium clearance is normally less than 5% of the glomerular filtration rate in individuals with normal renal function. The dangers of aluminium toxicity were initially recognized in patients with renal failure, who were receiving dialysis treatment. ‘Dialysis dementia’, an encephalopathy occurring in renal dialysis patients, was first described in 1972 [65], and was found to be associated with the accumulation of aluminium in the brain [66].The recog- Plasma aluminium protein-bound (mainly to transferrin) (alumino-silicates) Tissue uptake Inhibition of caffeine-sensitive Ca2+-channels [76] Binding to [73, 741 Disruption of Biopterin meta bolism [72, 73, 751 Gene transcription Fig. 2. Some effects of absorbed aluminium. lnterfe :nce with cell signalling Gastrointestinal absorption and renal excretion of aluminium nition of this condition led to many more reports of aluminium-related dementia in renal patients. Other pathological features, including vitamin D-resistant osteodystrophy, were also evident in such patients and the condition, first recognized in Newcastle-upon-Tyne (U.K.), was termed ‘Newcastle bone disease’. The above conditions are caused by aluminium entering the blood and being deposited in the body tissues, deposition in the brain leading to encephalopathy, and deposition in bone leading to osteodystrophy. In the renal failure patients there were two sources of this aluminium: (1)the water used for dialysis, and (2) dietary aluminium hydroxide used as a phosphate-binder in such patients. The obvious question is whether the aluminium toxicity was due to impaired excretion consequent upon the renal impairment, or to excessive amounts of aluminium entering the plasma by bypassing the gut barrier (or both). Because of the complex relationship between proteinbinding of aluminium, and the plasma aluminium concentration, it is difficult to assess quantitatively the role of the kidney in aluminium excretion. Renal aluminium clearance decreases with increasing plasma aluminium concentration [60, 62, 671. However, since plasma aluminium concentration in healthy subjects is low, 10 pg/l o r less, it seems likely that the kidneys play an important role in aluminium excretion. Little is known of the renal tubular handling of aluminium, and this is a question we are currently investigating. Work by Galle [68] has indicated that, after filtration, aluminium is reabsorbed by the renal tubule cells and is bound intracellularly to phosphates and proteins [60, 691. There is also evidence of distal tubular secretion [70]. From time to time, incidents of high aluminium exposure occur (e.g. in Camelford, Cornwall, U.K., where aluminium sulphate was added in high concentration to drinking water in July 1988). Clearly, if we had greater understanding of the renal mechanisms involved in aluminium excretion, this might increase the possibility of improving aluminium clearance. If renal transport mechanisms for aluminium resemble those in the gut, then drugs or procedures which mod@ for example calcium absorption (see, for example, [71]) might be useful in modifying aluminium absorption. Clearly, this is an area in which more research is needed. ACKNOWLEDGMENTS Work by C.J.L. on renal aluminium handling is currently supported by the Wellcome Trust and the Sandoz Foundation for Gerontological Research. REFERENCES 1. De Broe, M.E. & Van de Vyver, EL. (eds.) Aluminium: a clinical problem in nephrology. Clin. Nephrol. 1985; 24, Suppl. 1. 2. Lione, A. Aluminium toxicity and the aluminium containing medications. Pharmacol. Ther. 1985; 29,255-85. 293 3. Savory, J., Bertholf, R.L. & Wills, M.R. Aluminium toxicity in chronic renal failure. Clin. Endocrinol. Metab. 1985; 14, 681-702. 4. Alfrey, A.C. Aluminium metabolism. Kidney Int. 1986; 29 (Suppl. 18),S.8-11. 5. Wilhelm, M., Jager, D.E. & Ohnesorge, F.K. Aluminium toxicokinetics. Pharmacol. Toxicol. 1990; 66,4-9. 6. Sorensen, J.R.J., Campbell, I.R., Tepper, L.B. & Lingg, R.D. Aluminium in the environment and human health. Environ. Health Perspect. 1974; 8,3-95. 7. Pennington, J.A.T. Aluminium content of foods and diets. Food Addit. Contam. 1987; 5, 161-232. 8. Lione, A. The prophylactic reduction of aluminium intake. Food Chem. Toxicol. 1983; 21,103-9. 9. Prescott, A. What’s the harm in aluminium. New Sci. 1989; 1648,58-62. 10. Koch, K.R., Pougnet, B., de Villiers, M.A. & Monteagudo, F. Increased urinary excretion of aluminium after drinking tea. Nature(London) 1988; 333, 122. 10a. Farrar, G. & Blair, J.A. Aluminium and Alzheimer’s disease. Lancet 1989: i. 269. 11. Freundlich, M., Zilleruelo, G., Abitbol, C., Straws, J., Faugere, M.C. & Malluche, H.H. Infant formula as a cause of aluminium toxicity in neonatal uraemia. Lancet 1985; ii, 527-9. 12. Koo, W.W.K., Kaplan, L.A. & Krug Wispe, S.K. Aluminium contamination of infant formulas. J. Parenter. Enteral Nutr. 1988; 12,170. 13. Braithwaite, R.A. & Cowtan, P.R. Experience in the provision of a water aluminium monitoring service for home dialysis patients in the West Midlands. In: Taylor, A., ed. Aluminium and other trace elements in renal disease. London: Bailliere Tindall, 1986: 156-66. 14. Winney, R.J., Cowie, J.F. & Robson, J.S. Role of plasma aluminium in the detection and prevention of aluminium toxicity. Kidney Int. 1986; 29 (Suppl. IS), S.91-5. 15. Parkinson, L.S., Ward, M.K., Feest, T.G., Fawcett, R.W.P. & Kerr, D.N.S. Fracturing dialysis osteodystrophy and dialysis encephalopathy - an epidemiological survey. Lancet 1979; i, 406-9. 16. Martyn, C.N., Osmond, C., Edwardson, J.A., Barker, D.H.P., Harris, E.C. & Lacey, R.F. Geographical relation between Alzheimer’s disease and aluminium in drinking water. Lancet 1989; i, 59-62. 17. Mauras, Y., Allain, P. & Riberi, P. Etude de I’absorption digestive de I’hydrocarbonate d’aluminium chez I’individu sain. Therapie 1982; 37,593. 18. Brown, S., Mendoza, N., Bertholf, R.L. et al. Absorption of aluminium from aceglutamide aluminium in healthy adult males. Res. Commun. Chem. Pathol. Pharmacol. 1986; 53, 105-16. 19. Haram, E.M., Weberg, R. & Berstad, A. Urinary excretion of aluminium after ingestion of sucralfate and an aluminium-containing antacid in man. Scand. J. Gastroenterol. 1987; 22,615-18. 20. Yokel, R.A. & McNamara, P.J. Influence of renal impairment, chemical form, and serum protein concentration on intravenous and oral aluminium kinetics in the rabbit. Toxicol. Appl. Pharmacol. 1988; 95,32-43. 21. Molitoris, B.A., Froment, D.H., MacKenzie, T.A., Huffer, W.H. & Alfrey, A.C. Citrate: a major factor in the toxicity of orally administered aluminium compounds. Kidney Int. 1989; 36,949-53. 22. Van der Voet, G.B. & de Wolff, F.A. A method of studying the intestinal absorption of aluminium in the rat. Arch. Toxicol. 1984; 55,168. 23. Gorsky, J.E., Dietz, A.A., Spencer, H. & Osis, D. Metabolic balance of aluminium studied in six men. Clin. Chem. 1979; 25,1739-43. 24. Williams, J.W., Vera, S.R., Peters, T.G. et al. Biliary excretion of aluminium in aluminium osteodystrophy with liver disease. Ann. Intern. Med. 1986; 104,782-5. 294 C.J. Lote and H. Saunders 25. Kovalchik, M.T., Kaehny, W.D., Jackson, T. & Alfrey, A.C. Aluminium kinetics during haemodialysis. J. Lab. Clin. Med. 1978; 92,712-6. 26. Martin, R.B. The chemistry of aluminium as related to biology and medicine. Clin. Chem. 1986; 32,1797-806. 27. Trapp, G.A. Interactions of aluminium with cofactors, enzymes and other proteins. Kidney Int. 1986; 29 (Suppl. __ 18); S.12-16. 28. Reference deleted. 29. Slanina, P., Frech, W., Gkstrom, L.G., Loof, L., Slorach, S. & Cedergren, A. Dietary citric acid enhances absorption of aluminium in antacids. Clin. Chem. 1986; 32,539-41. 30. Slanina, P., Falkeborn, Y., Frech, W. & Cedergren, A. Aluminium concentration in the brain and bone of rats fed citric acid, aluminium citrate or aluminium hydroxide. Food Chem. Toxicol. 1984; 22, 391-7. 31. Weberg, R. & Berstad, A. Gastrointestinal absorption of aluminium from single doses of aluminium-containing antacids in man. Eur. J. Clin. Invest. 1986; 16,428-32. 32. Slanina, P., Frech, W., Bernhardson, A., Cedergren, A. & Mattsson, P. Influence of dietary factors on aluminium absorption and retention in the brain and bones of rats. Acta Pharmacol. Toxicol. 1985; 56,331-6. 33. Froment, D.H., Buddington, B., Miller, N.L. & Alfrey, A.C. Effect of solubility on the gastrointestinal absorption of aluminium for various aluminium compounds in the rat. J. Lab. Clin. Med. 1989; 114,237-42. 34. Martinez Paloma, A,, Meza, I., Beaty, G. & Cereijido, M. Experimental modulation of occluding junctions in a cultured transporting epithelium. J. Cell Biol. 1980; 87, 736-45. 35. Adler, A J . & Berlyne, G.M. Duodenal aluminium absorption in the rat. Effect of vitamin D. Am. J. Physiol. 1987; 249, F209-13. 36. Provan, S.D. & Yokel, R.A. Aluminium uptake by the in sific rat gut preparation. J. Pharmacol. Exper. Ther. 1988; 245, 928-31. 37. Provan, S.D. & Yokel, R.A. Influence of calcium on aluminium uptake by the rat jejunal slice. Res. Commun. Chem. Pathol. Pharmacol. 1988; 59,79-92. 38. Barac-Neto, M. Effects of pH, calcium, and succinate on sodium-citrate cotransport in renal microvilli. Am. J. Physiol. 1984; 247, F282-90. 39. Spencer, H., Kramer, L., Norris, C. & Wiatrowski, E. Effect of aluminium hydroxide on fluoride metabolism. Clin. Pharmacol. Ther. 1980; 28,529-35. 40. Platts, M.M., Goode, G.C. & Hislop, J.S. Composition of the domestic water supply and the incidence of fractures and encephalopathy in patients on home dialysis. Br. Med. J. 1977; ii, 657-60. 41. Still, G.N. & Kelley, P. On the incidence of primary degenerative dementia vs water fluoride content in South Carolina. Neurotoxicology 1980; 4, 125-3 1 . 42. Birchall, J.D. & Chappell, J.S. Aluminium, chemical physiology and Alzheimer’s disease. Lancet 1988; ii, 1008-10. 43. Birchall, J.D., Exley, C., Chappell, J.S. & Phillips, M.J. Acute toxicity of aluminium to fish eliminated in silicon-rich acid waters. Nature (London) 1989; 338, 146-8. 44. Trapp, G.A. Plasma aluminium is bound to transferrin. Life Sci. 1983; 33,311-16. 45. Touam, M., Martinez, F., Lacour, B. et al. Aluminium induced reversible microcytic anaemia in chronic renal failure. Clin. Nephrol. 1983; 19,295-8. 46. Van der Voet, G.B. & de Wolff, F.A. Intestinal absorption of aluminium in rats: effect of intraluminal pH and aluminium concentration. J. Appl. Toxicol. 1986; 6,37-41. 47. Cannata, J.B., Suarez, C., Cuesta, V. et al. Gastrointestinal aluminium absorption: is it modulated by the iron absorptive mechanism? Proc. EDTA-ERA 1984; 21,354-9. 48. Blaehr, H., Madsen, S. & Rud Anderson, J. Effect of iron loading on intestinal aluminium absorption in chronic renal insufficiency. In: Taylor, A., ed. Aluminium and other trace elements in renal disease. London: Bailliere Tindall, 1986: 71-5. 49. Van der Voet, G.B. & de Wolff, F.A. Intestinal absorption of aluminium in rats. Effect of sodium mechanisms and models in toxicology. Arch. Toxicol. 1987; 11,231-5. 50. Mayor, G.H., Sprague, S.M., Hourani, M.R. & Sanchez, T.V. Parathyroid-hormone mediated aluminium deposition and egress in the rat. Kidney Int. 1980; 17,40-4. 51. Mayor, G.H. & Burnatowska-Hledin, M.A. Impaired renal function and aluminium metabolism. Fed. Proc. Fed. Am. SOC.Exp. Biol. 1983; 42,2979-83. 52. O’Brien, A.A., Moore, D.P. & Keogh, J.A. Aluminium osteomalacia in chronic renal failure patients neither on dialysis nor taking aluminium-containing phosphate binders. Ir. J. Med. Sci. 1990; 1 5 9 , 7 4 4 . 53. Hell, T.H., Hofstadter, F., Gladziwa, U. & Sieberth, H.G. Reduced deposition of aluminium in trabecular bone of uraemic rats treated with dihydroxylated vitamin D metabolites. Nephrol. Dial. Transplant. 1989; 4,957-65. 54. Cannata, J.B., de Francisco, A.M., Amado, J.A. et al. Parathyroid hormone release under the influence of aluminiumdesferrioxamine complex. In: ’Taylor, A., ed. Aluminium and other trace elements in renal disease. London: Bailliere Tindall, 1986: 38-44. 55. Burnatowska-Hledin, M.A., Doyle, T.M., Eadie, M. & Mayor, G.H. 1,12-Dihydroxyvitamin D, increases gastrointestinal absorption and serum and tissue concentration of aluminium in rats. Fed. Proc. Fed. Am. SOC.Exp. Biol. 1984; 43,338. 56. Alfrey, A.C., Hegg, A. & Craswell, P. Metabolism and toxicity of aluminium in renal failure. Am. J. Clin. Nutr. 1980; 33,1509-16. 57. Ittel, T.H., Buddington, B., Miller, N.L. & Alfrey, A.C. Enhanced gastrointestinal absorption of aluminium in uremic rats. Kidney Int. 1987; 32,821-6. 58. Santos, F., Massie, M.D. & Chan, J.M.C. Risk factors in aluminium toxicity in children with chronic renal failure. Nephron 1986; 42, 189-95. 59. Gidden, H., Holland, F.F. & Klien, E. Trace metal protein binding in normal and dialysed uremic serum. Trans. Am. SOC.Artif. Intern. Organs 1980; 26, 133-8. GO. Burnatowska-Hledin, M.A., Mayor, G.H. & Lau, K. Renal handling of aluminium in the rat: clearance and micropuncture studies. Am. J. Physiol. 1985; 249, F192-7. 61. Rahman, H., Skillen, A.W., Channon, S.M., Ward, M.K. & Kerr, D.N.S. Methods for studying the binding of aluminium by serum protein. Clin. Chem. 1985; 31, 1969-73. 62. Hohr, D., Abel, J. & Wilhelm, M. Renal clearance of aluminium. Studies in the isolated perfused rat kidney. Toxicol. Lett. 1989; 45, 165-74. 63. Keahny, W.D., Hegg, A.P. & Alfrey, A.C. Gastrointestinal absorption of aluminium from aluminium-containing antacids. N. Engl. J. Med. 1977; 296, 1389-90. 64. Ryan, G.B. The glomerular filtration barrier. In: Lote, C.J., ed. Advances in Renal Physiology. London: Croom Helm, 1986: 1-32. 65. Alfrey, A.C., Mishell, J.M., Burks, J. et al. Syndrome of dyspraxia and multifocal seizures associated with chronic haemodialysis. Trans. ASAlO 1972; 18,257-61. 66. Alfrey, A.C., LeGendre, G.R. & Kaehny, W.D. The dialysis encephalopathy syndrome. Possible aluminium intoxication. N. Engl. J. Med. 1976; 294, 184-8. 67. Pai, S.M. & Melethil, S. Kinetics of aluminium in rats. I. Dose-dependent elimination from blood after intravenous administration. J. Pharm. Sci. 1989; 78,200-2. 68. Galle, P. In: Hamburger, J., ed. Advances in Nephrology. London: Year Book Medical Publications, 1983: vol. 12, 85-9. 69. Gupta, S.K., Waters, D.H. & Gwilt, P.R. Absorption and disposition of aluminium in the rat. J. Pharm. Sci. 1986; 75, 586-9. Gastrointestinal absorption and renal excretion of aluminium 70. Monteagudo, F.S.E., Isaacson, L.C., Wilson, G., Hickman, R. & Folb, P.I. Aluminium excretion by the distal tubule of the pig kidney. Nephron 1988; 49,245-50. 71. Buck, A.C. & Lote, C J . The renal handling of calcium. In: Wickham, J.E.A. & Buck, A.C., eds. Renal tract stone. Edinburgh: Churchill Livingstone, 1990: 165-82. 72. Altmann, P., Al-Salihi, F., Butter, K. et al. Serum aluminium levels of erythrocyte dihydropteridine reductase activity in patients on haemodialysis. N. Engl. J. Med. 1987; 317, 80-4. 73. Johnson, G.V.W. & Jope, R.S. Aluminium alters cyclic AMP and cyclic GMP levels but not presynaptic cholinergic markers in rat brain in vivo.Brain Res. 1987; 403, 1-6. 295 74. Johnson, G.V.W., Li, X. & Jope, R.S. Aluminium increased agonist-stimulated cyclic AMP production in rat cerebral cortical slices. J. Neurochem. 1989; 53,258-63. 75. Leeming, R.J. & Blair, J.A. Dialysis dementia, aluminium and tetrahydrobiopterin metabolism. Lancet 1979; i, 556. 76. Wakui, M., Itaya, K., Birchall, D. & Petersen, O.H. Intracellular aluminium inhibits acetycholine- and caffeineevoked Ca2+mobilisation. FEBS Lett. 1990; 267,301-4. 77. McDonald, L.J. & Mamrack, M.D. Aluminium affects phosphoinositide hydrolysis by phosphoinositide C. Biochem. Biophys. Res. Commun. 1988; 155,203-8.