Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
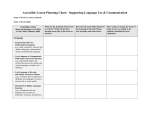
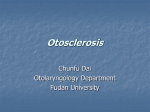
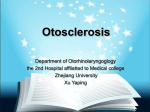
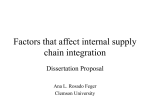
Nombre deessay Pictorial Sección Value of Multislice Computed Tomography in the evaluation of early Otosclerosis Nicolás López-Galletti, Alberto Surur, Mario Zernotti, Alberto Marangoni, Paula Tiscornia, Ignacio Simez. Resumen Abstract Introducción: La otoesclerosis (OS) es una enfermedad Introduction: Otosclerosis (OS) is a disease of unknown de etiología desconocida, que presenta una transmi- etiology. It is inherited in an autosomal dominant sión autosómica dominante. Afecta más frecuente- pattern. It affects 20-30-year-old women whose main mente a mujeres entre 20 y 30 años, que consultan clinical manifestation is conductive hearing loss with clínicamente por una hipoacusia de conducción. La OS more frequency. The OS is classified as fenestral (85%) se clasifica en fenestral (85%) y coclear (15%). La To- and cochlear (15%). Multislice Computed Tomography mografía Computada Multicorte (TCMC) es un método (MSCT) is the method of choice in the evaluation of the radiológico de elección en la valoración de la cápsula otic capsule. It can accurately show lesions at an initial ótica. Ésta puede demostrar con precisión lesiones en stage, such as millimetric hypodense areas, mainly at la etapa inicial como focos hipodensos milimétricos, the fissula ante fenestram (FAF) as a sign of “early or principalmente a nivel de la Fisula Ante Fenestram initial” OS, even when the audiometric results show a (FAF) y pueden corresponderse como un signo “pre- gap of less than 20 db. coz o inicial” de OS, aun cuando en la audiometría Case review: Even though OS is a disease of unknown aparece un gap menor a 20 db. etiology, it is known that type II collagen fibers in the Revisión del tema: La OS es una enfermedad de etio- cartilage remnant tissue of the petrosal bone can gene- logía desconocida pero se sugiere una relación con las rate an autoimmune reaction that could be responsible Contact information: Nicolás López-Galletti. 38 Sanatorio Allende – Córdoba capital. Recibido: 4 de noviembre de 2014 / Aceptado: 6 de mayo de 2015 E-mail: [email protected] Received: November 4, 2014 / Accepted: May 6, 2015 Revista Argentina de Diagnóstico por Imágenes Value of MSCT in early Otosclerosis López-Galletti N. et al. fibras de colágeno tipo II, presentes en el tejido carti- for the resorption of bone tissue. This produces focal laginoso remanente del peñasco, las cuales generarían areas of spongy bone at the oval and round window una reacción autoinmune que sería la responsable and that is why it is called otospongiosis. Other authors de la reabsorción del tejido óseo. Esto produce zonas propose that this cartilaginous remnant tissue would focales de hueso esponjoso a nivel de la ventana oval be replaced by an immature and highly vascularized y redonda, por lo que se denomina otoespongiosis. bone tissue. Histopathological studies describe three Otros autores piensan que este remanente cartilagi- phases of this condition: acute (osteoid tissue), subacute noso sería remplazado por un tejido óseo inmaduro (osteoclastic remodeling) and chronic (sclerosis). y altamente vascularizado. Los estudios histopatoló- Conclusion: Multislice Computed Tomography may gicos la dividen en tres fases: aguda (tejido osteoide), be used as an additional and effective tool for the subaguda (remodelación osteoclástica) y crónica diagnosis of early or initial OS (audiometry gap of 20 (esclerosis). db), showing millimetric hypodense areas that cannot Conclusión: La TCMC puede ser usada como una be visualized by means of conventional CT, mainly at herramienta adicional eficiente en el diagnóstico de the FAF. The findings are predominantly bilateral and OS precoz o temprana (audiometría con gap de 20 symmetrical. The thickness of the footplate provides db), mostrando focos hipodensos milimétricos, que no valuable data, particularly in patients who will undergo pueden ser visualizados por la TC convencional, prin- surgery. MSCT demonstrated a high sensitivity for the cipalmente a nivel de la FAF. Los hallazgos son pre- diagnosis of this pathology. dominantemente bilaterales y simétricos. El espesor de la platina del estribo aporta datos de valor sobre todo en pacientes que van a ser sometidos a cirugía. La TCMC demostró tener una gran sensibilidad para el diagnóstico de esta patología. Palabras clave: Otoesclerosis precoz, Otoespongio- Key words: Early Otosclerosis, Otospongiosis, Fissula sis, Fisula Ante Fenestram, Tomografía Computada ante Fenestram, Multislice Computed Tomography. Multicorte. Introduction Otosclerosis (OS) is a disease of unknown etiology. It is inherited in an autosomal dominant pattern (1, 2). Frequently, it affects women aged 20-30, with tinnitus and conductive hearing loss. The presentation of this condition is bilateral in 80% (3). Cochlear involvement is associated with neurosensory hearing loss, secondary to the action of protease that affects nerve cells. OS is classified as fenestral (85%) and cochlear (15%), causing hearing loss that can be conductive, neurosensory or a combination of both. Initially, conVol. 4 / Nº 11 - Agosto 2015 ductive hearing loss, which is the most frequent, has an air-bone gap equal or greater than 20 db, with a tympanometric rigid curve (Type A Jerger curve). In these cases, imaging studies can be useful to reach an early and accurate diagnosis. They play an important role in the diagnosis and clinical management of OS. Multislice Computed Tomography (MSCT) is the radiologic method of choice to assess the labyrinthine windows and the otic capsule. It can show the active or spongiotic lesions of OS at an early stage with precision. The lesions are millimetric lytic or hypodense areas that cannot be detected with conventio39 Value of MSCT in early Otosclerosis nal tomography and that can be seen predominantly in the otic capsule, mainly at the level of fissula ante fenestram (FAF) as an “early” sign of OS (1-4). When we talk about early signs of OS we refer to the radiological findings mentioned above, even when the audiometry shows a slight loss in hearing, whether they are conductive, neurosensory or a combination of both. These lesions can be unique or multiple, confluent or non-confluent, bilateral or unilateral and can be the cause of a process of bone demineralization (5, 6) or of a thickening of the footplate to a size greater than 0.6 mm. MSCT performs narrower views with a greater spatial definition, which helps characterize lesions better. Case review OS is a disease of unknown etiology and it is inherited in an autosomal dominant or recessive pattern. This condition is also related to fibrillary collagen type II present in the cartilage remnant from the petrosal bone, which would generate the autoimmune reaction of reabsorbing bone tissue. This produces focal areas of spongy bone at the level of the oval and rounded window and that is why it receives the name of otospongiosis (1, 2). Other authors think that this cartilaginous remnant would be replaced by an immature and highly vascularized bone tissue (7). Histopathological studies describe three phases of this condition: acute (osteoid tissue), subacute (osteoclastic remodeling) and chronic (sclerosis). An advanced cochlear OS often has hypodense areas producing an image of a halo around the bony labyrinth, frequently at the level of the basal cochlear turn, which is called “double-ring sign”. In addition, in a chronic stage there are calcification areas in those regions that appear as “plate-like bones”. The complete obliteration of the oval window in 2% of the cases is called obliterative fenestral OS. Among differential diagnoses there is tympanosclerosis, Paget’s disease, fibrous dysplasia and osteogenesis imperfecta (1). Paget’s disease: It affects people older than 60 and it is part of the diseases of bone metabolism. Initially, it generates a lytic diffuse process affecting the bony labyrinth, and in an advanced stage it produces an increase in bone density. It starts in the vertex of the 40 López-Galletti N. et al. petrosal bone and progresses laterally. It differs from OS in that Paget’s disease starts in the peripheral region and progresses in a centripetal way affecting the otic capsule in a later stage, whereas OS progresses in reverse. Paget’s disease also affects the calvaria. Fibrous dysplasia: It affects people younger than 30 years of age. It produces a ground-glass density that expands the bone preserving the cortex. Commonly, it affects the mastoid and presents slight involvement of the bony labyrinth, facial nerve canal and internal auditory canal. Lytic lesions are less common. Osteogenesis imperfecta: It affects children with brittle bones and blue sclerae. It can be hard to differentiate it from advanced cochlear OS. Tympanosclerosis: It is a post-inflammatory deposit of new bone tissue that is not limited to the oval window and can affect all of the middle ear structures, tympanic membrane and mastoid. The bone tissue deposit has an irregular morphology (8-10). The primary objective of MSCT in this type of pathology is to prove the existence and distribution of the early focal area of otosclerosis (FAOS) since these findings were not visible through conventional or basic helical tomography. According to international literature, the sensitivity of MSCT or computed conventional tomography for the diagnosis of OS ranges from 34% to 90%. However, recent studies have shown that MSCT has a positivity of 90% to detect fenestral focal areas in an early stage of the disease (5, 6, 11). It is not possible to detect these early little changes with conventional computed tomography. Figure 1 shows one of the most relevant tomographic views that require a detailed analysis of the anatomy to obtain as much information as possible. Marx et al. identified a sensitivity of 95% and a specificity of 99,1% in the diagnosis of OS (12). Our samples consisted of 58 MSCT performed on patients with a clinical auditory diagnosis of OS, i. e., they had an air gap of 20 db to 25 db in low and middle pitch frequencies and a tympanometry with a rigid Type A Jerger curve. Some of the patients had absent stapedial reflex. MSCT demonstrated a sensitivity of 95% in the detection of focal areas of otospongiosis. Oliveira et al. (4) identified focal areas of OS in 47 patients (87%). Shin et al. (5) observed that 84.7% of patients with focal areas of OS in MSCT had positive Revista Argentina de Diagnóstico por Imágenes Value of MSCT in early Otosclerosis López-Galletti N. et al. clinical results. In 70% to 95% of cases, otodystrophic lesions of otospongiosis are located at the fenestral level in the FAF. This topography must be considered as the most important in the radiologic diagnosis of this entity (3, 4). In our study there were 55% to 60% cases of focal areas of OS at the level of the FAF, in both the right ear and the left ear. Oliveira et al. (4) identified focal areas of OS at the same level in 83.3% of patients. Shin et al. (5) in 69.8%, and Veillon et al. (13) in 68.2%. Wycherly et al. (7) identified lesions at the level of FAF in 21 out of 24 patients (87.5%). This is an area with great radiologic relevance for the early diagnosis of patients suspected of having OS that should be analyzed in detail during a tomographic examination. Shin et al. (5) identified bilateral focal areas of OS in 78.7% and bilateral and symmetrical focal areas in 38% of patients. Oliveira et al. (4) identified these findings in 70% and 48.38% of the cases, respectively. In patients studied for this research paper, 70.68% presented bilateral focal areas of OS, and 68.96% presented symmetrical focal areas. In 1.72% of the cases the presentation was symmetrical. A study conducted by Wycherly et al. (7) showed that 10 patients (56%) had bilateral OS, 4 (22%) had unilateral OS, and 4 (22%) did not present focal areas of OS. 8 out of 10 patients presented bilateral and symmetrical OS (80%). In our cases, 14 patients (24.13%) had unilateral focal areas of OS. Based on histopathological findings of patients who underwent surgery reported in literature, the round window is the second most commonly affected region with an incidence that ranges from 20% to 50% (14). Evidence of the involvement of the footplate provides valuable information, especially in cases of patients selected to undergo stapedectomy. Veillon et al. (10) defined an abnormal thickening of the footplate greater than 0.6 mm, which was found in 12.7% of their patients. Shin et al. (5) observed this in 23% of the cases. Other series presented similar percentages of pericochlear region involvement of around 19.4% and 24.13% of the cases. Wycherly et al. (7) visualized focal areas at the post fenestram level in 10% of the tomographic exams Vol. 4 / Nº 11 - Agosto 2015 analyzed. Children usually present hypodense areas in the otic capsule that suggest the differential diagnosis of early OS and are attributed to an incomplete bone mineralization or to the presence of cartilage at the level of the FAF. These areas represent a normal pattern of growth of the anterior otic capsule and they should not be confused with pathological conditions. However, in older patients, these hypodense areas in the FAF can be considered as potential signs of early OS (2). Not all patients undergo surgery and, therefore, histopathological confirmation of these alterations is not always possible. That is why MSCT is actually used to confirm clinical findings and findings from the most precise results of otorhinolaryngological examinations and tests available. Findings in MSCT MSCT can show active or spongiotic lesions of OS in an early stage with precision. They appear as small hypodense o millimetric lytic areas at the level of the FAF or at a pericochlear level. In addition, a thickening of the footplate greater than 0.6 mm is considered an early sign of OS. In relation to the location, focal areas of OS have a bilateral and symmetrical distribution in around 70% of the cases (Figure 2 and 3), a unilateral and symmetrical location in 2% of the cases, and a unilateral location in 25% of the patients (Figure 4). In 5% of the cases, they can be negative. Based on our observations and in relation to other series of patients, focal areas of OS are located most commonly at the level of FAF (around 65% of the cases) (Figure 5) followed by a cochlear location, with an approximate percentage of 35%, both in the right and left ears (Table 1). The sensitivity of MSCT to detect the presence of focal areas in patients with OS was 95%, which means that every 100 patients with a clinical and auditory suspicion of OS, MSCT could detect focal areas in 95 patients. 41 Value of MSCT in early Otosclerosis López-Galletti N. et al. Figure 1. Ear MSCT with high-definition axial view. Normal anatomy. COC: Cochlea, FAF: Fissula ante fenestram, VES: Vestibule, CSP: Posterior semicircular canal, PLE: Footplate, CPE: Posterior crura of stape, CAE: Anterior crura of stape, YUN: Incus, MAR: Hammer. Figure 2. Ear MSCT with high-definition axial view. Millimetric hypodense areas at the level of the FAF bilateral and symmetrically (white arrows). Figure 3. Ear MSCT with high-definition coronal view. Presence of bilateral and symmetrical focal OS at the level of the FAF (arrowheads). 42 Revista Argentina de Diagnóstico por Imágenes Value of MSCT in early Otosclerosis López-Galletti N. et al. Figure 4. MSCT with high-definition axial view of right and left ear. Patient with unilateral focal OS at the level of the FAF on the left side (black box). Figure 5. MSCT with high-definition axial view of the left ear at the level of the petrosal bone. Hypodense area of OS (white circle) between the vestibule and the cochlea in the topography of the fissula ante fenestram (FAF). Graphic 1. Location of the focal area. Common spots of early focal areas of OS. Black: FAF; Dark gray: Pericochlear; Light gray: Fissula Post Fenestram; Gray line: Thickening of the footplate. Vol. 4 / Nº 11 - Agosto 2015 43 Value of MSCT in early Otosclerosis López-Galletti N. et al. Table 1. Conclusion MSCT may be used as an additional and effective tool to diagnose early OS even when auditory findings present a small gap ranging from 20 to 25 db and millimetric hypodense areas that cannot be visualized by conventional CT, mainly at the FAF. The findings are predominantly bilateral and symmetrical. The thickness of the footplate provides valuable data 44 particularly in patients who will undergo surgery. MSCT demonstrated a high sensitivity for the early diagnosis of this pathology. Revista Argentina de Diagnóstico por Imágenes López-Galletti N. et al. Value of MSCT in early Otosclerosis Bibliography 1- Miranda G, Orellana P, Matus C, Pulgar H, Torres A, Prieto J. Otosclerosis: Análisis Imagenológico con tomografía computada multicorte. Revista HCUCh 2006; 17:356-359. 2- Moser T, Veillon F, Sick H, Reihm S. The hypodense focus in the petrous apex: a potencial pit-fall on multidetector CT imaging of the temporal bone. AJNR Am J Neuroradiol Jan 2008; 29:35-39. 3- Lee T, Aviv R, Chen J, Nedzelski J, Fox A, Symons S. CT Grading of Otosclerosis. AJNR Am J Neuroradiol Aug 2009; 30:1435-39. 4- Oliveira A, Yamashita H, Manguabeira P, Oliveira N. Computed Tomography in the diagnosis of otosclerosis. Otolaryngology Head and Neck Surgery 2006; 134:685-692. 5- Shin Y, Fraysse B, Deguine O, et al. Sensorineural hearing loss and otosclerosis: a clinical and radiologic survey of 437 cases. Acta Otolaryngol 2001a; 121:200-4. 6- Berrettini S, Ravecca F, Volterrani D, et al. Single photon emission computed tomography in otosclerosis: diagnostic accuracy and correlation with age, sex, and sensorineural involvement. Otol Neurotol, 2002; 23:431-8. 7- Wycherly B, Berkowitz F, Noone A, Kim J. Computed Tomography and Otosclerosis: A Practical Method to Correlate the Site Affected to Hearing Loss. Annals of Otology, Rhinology and Laryngology, 2010; 119(12):789-794. 8- Wolfgang Dähnert. Ear, nose and throat. In: Lippincott Williams and Williams, ed. Radiology Review Manual. 6ta ed. Philadelphia, Pa: 19106 USA, 2007; 355-403. 9- Grosman R, Yousem D. Hueso Tempral. En: Marbán ed. Neurorradiologia. 2da ed. España, Madrid, 2007; 565-608. 10- Alvarado Rosas J, García Vázquez D, Villar Blanco I, Martínez San Millán J. Diagnóstico Diferencial de las Lesiones líticas de la Cápsula Otica. EPOSTM. DOI: 10.1594/seram2012/S-0282. Poster Educativo Congreso SERAM, 2012. 11- Shin Y, Calvas P, Deguine O, et al. Correlation between computed tomography findings and family history in otosclerotic patients. Otol Neurotol, 2001b; 22:461-4. 12- Marx M, Lagleyre S, Escude B, Demeslay J, Elhadi T, Deguine O, Fraysse B. Correlations between CT scan findings and hearing thresholds in otosclerosis. Acta Oto-Laryngológica, 2011; 131:351-357. 13- Veillon F, Rieh S. Imaging of the windows of the temporal bone. Seminars in Ultrasound, CT, and MRI. 2001; 22(3):271-80. 14- Niedermeyer H, Arnold W. Etiopathogenesis of otosclerosis. ORL J. 2002; 64:114-9. Vol. 4 / Nº 11 - Agosto 2015 45