Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
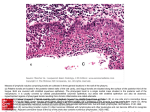
SIR WILLIAM OSLER THE PRINCIPLES AND PRACTICE OF MEDICINE, 8th EDITION New York: D. Appleton and Company, 1919 II. CHRONIC TONSILLITIS (Chronic Naso-pharyngeal Obstruction; Adenoids; Mouth-breathing; Aprosexia) Under this heading will be considered also hypertrophy of the adenoid tissue in the vault of the pharynx, sometimes known as the pharyngeal tonsil, as the affection usually involves both the tonsils proper and this tissue, and the symptoms are not to be differentiated. Chronic enlargement of the tissues of the tonsillar ring is an affection of great importance, and may influence in an extraordinary way the mental and bodily development of children. Etiology.-- "Adenoids" have become recognized as one of the most common and important affections of childhood, occurring most frequently between the fifth and tenth years. The introduction of the systematic inspection of school children has done more than anything else to force upon the profession and the public the recognition of the condition as one influencing seriously the bodily and mental growth, disturbing hearing and furnishing a focus for the development of pathogenic organisms. Few children escape altogether. In many it is a trifling affair, easily remedied; in others it is a serious and obstinate trouble, taxing the skill and judgment of the specialist. It is not easy to say why the disease has become so prevalent. In the United States it is attributed to the dry, hot air of the houses, in England to the cold, damp climate. In winter nearly all the school children in England have the "snuffles," and a considerable proportion of them adenoids. Interested in the subject ever since reading Meyer's original paper, I thought American children especially prone, but the disease seems to be even more prevalent in England. Adenoids may be associated with slight enlargement of the lymph-glands, thymus and spleen in the condition of lymphatism. Morbid Anatomy.-- The tonsils are enlarged, due to multiplication of all the constituents of the glands. The lymphoid elements may be chiefly involved without much development of the stroma. In other instances the fibrous matrix is increased, and the organ is then harder, smaller, firmer, and is cut with much greater difficulty. The adenoids, which spring from the vault of the pharynx, form masses varying in size from a small pea to an almond. They may be sessile, with broad bases, or pedunculated. They are reddish in color, of moderate firmness, and contain numerous blood-vessels. "Abundant, as a rule, over the vault, on a line with the fossa of the Eustachian tube, the growths may lie posterior to the fossa namely, in the depression known as the fossa of Rosenmuller, or upon the parts which are parallel to the posterior wall of the pharynx. The growths appear to spring in the main from the mucous membrane covering the localities where the connective tissue fills in the inequalities of the base of the skull" (Harrison Allen). The growths are most frequently papillomatous with a lymphoid parenchyma. Hypertrophy of the pharyngeal adenoid tissue may be present without great enlargement of the tonsils proper. Chronic catarrh of the nose usually coexists. Symptoms.-- The direct effect of adenoids is the establishment of mouth breathing. The indirect effects are deformation of the thorax, changes in the facial expression, sometimes marked alteration in the mental condition, in certain cases stunting of the growth, and in a great many subjects deafness. Woods Hutchinson has suggested that the embryological relation of these structures and the pituitary body may account for the interference with development. The establishment of mouth-breathing is the symptom which first attracts the attention. It is not so noticeable by day, although the child may present the vacant expression characteristic of this condition. At night the child's sleep is greatly disturbed; the respirations are loud and snorting, and there are sometimes prolonged pauses, followed by deep, noisy inspirations. The pulse may vary strangely during these attacks, and in the prolonged intervals may be slow, to increase greatly with the forced inspirations. The alae nasi should be observed during the sleep of the child, as they are sometimes much retracted during inspiration, due to a laxity of the walls, a condition readily remedied by the use of a soft wire dilator. Night terrors are common. The child may wake up in a paroxysm of shortness of breath. Sometimes these attacks are of great severity and the dyspnoea, or rather orthopnoea, may suggest pressure of enlarged glands on the trachea. Sometimes there is a nocturnal paroxysmal cough of a very troublesome character (Balne's cough), usually excited by lying down. The attacks may occur through the day. When the mouth-breathing has persisted for a long time definite changes are brought about in the face, mouth, and chest. The facies is so peculiar and distinctive that the condition may be evident at a glance. The expression is dull, heavy, and apathetic, due in part to the fact that the mouth is habitually left open. In long-standing cases the child is very stupid-looking, responds slowly to questions, and may be sullen and cross. The lips are thick, the nasal orifices small and pinchedin-looking, the superior dental arch is narrowed and the roof of the mouth considerably raised. The remarkable alterations in the shape of the chest in connection with enlarged tonsils were first carefully studied by Dupuytren (1828), who evidently fully appreciated the great importance of the condition. He noted "a lateral depression of the parietes of the chest consisting of a depression, more or less great, of the ribs on each side, and a proportionate protrusion of the sternum in front." J. Mason Warren (Medical Examiner, 1839) gave an admirable description of the constitutional symptoms and the thoracic deformities induced by enlarged tonsils. These, with the memoir of Lambron (1861), constitute the most important contributions to our knowledge on the subject. Three types of deformity may be recognized: (a) THE PIGEON OR CHICKEN BREAST, by far the most common form, in which the sternum is prominent and there is a circular depression in the lateral zone (Harrison's groove), corresponding to the attachment of the diaphragm. The ribs are prominent anteriorly and the sternum is angulated forward at the manubrio-gladiolar junction. As a mouth-breather is watched during sleep one can see the lower and lateral thoracic regions retracted during inspiration by the action of the diaphragm. (b) BARREL CHEST. Some children, the subject of chronic naso-pharyngeal obstruction, have recurring attacks of asthma, and the chest may be gradually deformed, becoming rounded and barrel-shaped, the neck short, and the shoulders and back bowed. A child of ten or eleven may have the thoracic conformation of an old man with emphysema. (C) THE FUNNEL BREAST (Trichterbrust). This remarkable deformity, in which there is a deep depression at the lower sternum, has excited much controversy as to its mode of origin. In some instances, at least, it is due to the obstructed breathing in connection with adenoid vegetations. I have seen two cases in children, in which the condition was in process of formation. During inspiration the lower sternum was forcibly retracted, so much so that at the height the depression corresponded to that of a well-marked "Trichterbrust." While in repose, the lower sternal region was distinctly excavated. The voice is altered and acquires a nasal quality. The pronunciation of certain letters is changed, and there is inability to pronounce the nasal consonants n and m. Bloch lays great stress upon the association of mouth-breathing with stuttering. The hearing is impaired, usually owing to the extension of inflammation along the Eustachian tubes and the obstruction with mucus or the narrowing of their orifices by pressure of the adenoid vegetations. In some instances it may be due to retraction of the drums, as the upper pharynx is insufficiently supplied with air. Naturally the senses of taste and smell are much impaired. With these symptoms there may be little or no nasal catarrh or discharge, but the pharyngeal secretion of mucus is always increased. Children, however do not notice this, as the mucus is usually swallowed, but older persons expectorate it with difficulty. Among other symptoms may be mentioned headache, which is by no means uncommon, general listlessness, and an indisposition for physical or mental exertion. Habit-spasm of the face has been described in connection with it. I have known several instances in which permanent relief has been afforded by the removal of the adenoid vegetations. Enuresis is occasionally an associated symptom. The influence upon the mental development is striking. Mouth-breathers are usually dull, stupid, and backward. It is impossible for them to fix the attention for long at a time, and to this impairment of the mental function Guye, of Amsterdam, has given the name aprosexia. Headaches, forgetfulness, inability to study without discomfort are frequent symptoms of this condition in students. There is more than a grain of truth in the aphorism shut your mouth and save your life, which is found on the title page of Captain Catlin's celebrated pamphlet on mouth-breathing (1861), to which cause he attributed all the ills of civilization. A symptom specially associated with enlarged tonsils is fetor of the breath. In the tonsillar crypts the inspissated secretion undergoes decomposition and an odor not unlike that of Limburger cheese is produced. The little cheesy masses may sometimes be squeezed from the crypts of the tonsils. Though the odor may not apparently be very strong, yet if the mass be squeezed between the fingers its intensity will at once be appreciated. In some cases of chronic enlargement the cheesy masses may be deep in the tonsillar crypts; and if they remain for a prolonged period time salts are deposited and a tonsillar calculus is in this way produced. Children with adenoids are especially prone to take cold and to recurring attacks of follicular disease. They are also more liable to diphtheria, and in them the anginal features in scarlet fever are always more serious. The ultimate results of untreated adenoid hypertrophy are important. In some cases the vegetations disappear, leaving an atrophic condition of the vault of the pharynx. Neglect may also lead to the so-called Thornwaldt's disease, in which there is a cystic condition of the pharyngeal tonsil and constant secretion of muco-pus. Diagnosis.-- The facial aspect is usually distinctive. Enlarged tonsils are readily seen on inspection of the pharynx. There may be no great enlargement of the tonsils and nothing apparent at the back of the throat even when the naso-pharynx is completely blocked with adenoid vegetations. In children the rhinoscopic examination is rarely practicable. Digital examination is the most satisfactory. The growths can then be felt either as small, flat bodies or, if extensive, as velvety, grape-like papillomata. Treatment.-- If the tonsils are large and the general state is evidently influenced by them they should be at once removed. Applications of iodine and iron, or penciling the crypts with nitrate of silver, are of service in the milder grades, but it is waste of time to apply them to very enlarged glands. There is a condition in which the tonsils are not much enlarged, but the crypts are constantly filled with cheesy secretions and cause a very bad odor in the breath. In such instances the removal of the secretion and thorough penciling of the crypts with chromic acid may be practiced. The galvano-cautery is of great service in many eases of enlarged tonsils when there is any objection to the more radical surgical procedure. The treatment of the adenoid growths in the pharynx is of the greatest importance, and should be thoroughly carried out. Parents should be frankly told that the affection is serious, one which impairs the mental not less than the bodily development of the child. In spite of the thorough ventilation of this subject by specialists, practitioners do not appear to have grasped as yet the full importance of this disease. They are far too apt to temporize and unnecessarily to postpone radical measures. The child must be anaesthetized. Severe haemorrhage has followed in a few cases. Special examination should be made of the thymus and lymph glands, as if they are enlarged the operation should be postponed. In this state of lymphatism death during anaesthesia has occurred. The good effects of the operation are often apparent within a few days, and the child begins to breathe through the nose. In some instances the habit of mouth-breathing persists. As soon as the child goes to sleep the lower jaw drops and the air is drawn into the mouth. In these cases a chin strap can be readily adjusted, which the child may wear at night. In severe eases it may take months of careful training before the child can speak properly. An all-important point in the treatment of lesions of the naso-pharynx (and, indeed, in the prevention of this unfortunate condition) is to increase the breathing capacity of the chest by making the child perform systematic exercises, which cause the air to be driven freely and forcibly in and out through the naso-pharynx. I cannot too strongly recommend this suggestion of Mr. Arbuthnot Lane. Throughout the entire treatment attention should be paid to hygiene and diet, and cod-liver oil and the iodide of iron may be administered with benefit.