Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Sex in advertising wikipedia , lookup
Sex reassignment therapy wikipedia , lookup
Ego-dystonic sexual orientation wikipedia , lookup
Sexuality after spinal cord injury wikipedia , lookup
Sexual ethics wikipedia , lookup
Sexological testing wikipedia , lookup
History of human sexuality wikipedia , lookup
Human female sexuality wikipedia , lookup
Human sexual response cycle wikipedia , lookup
Lesbian sexual practices wikipedia , lookup
Slut-shaming wikipedia , lookup
Sexual attraction wikipedia , lookup
Female promiscuity wikipedia , lookup
Rochdale child sex abuse ring wikipedia , lookup
Sexual dysfunction wikipedia , lookup
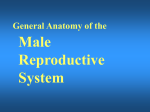
Mini Reviews TOPICAL TREATMENTS FOR PREMATURE EJACULATION MORALES et al. The three mini-reviews this month cover several areas of interest, including premature ejaculation, urological malignancies after renal transplantation and the muchvexed issue of the relevance of prostate size to prostate disease. Each of these should help to keep the readers up-to-date with each of these important topics. A review of the current status of topical treatments for premature ejaculation Alvaro Morales, James Barada* and Michael G. Wyllie† Centre for Applied Urological Research, General Hospital & Queens University, Kingston, Ontario, Canada, *Centre for Male Sexual Health, Albany, New York, USA, and †Plethora Solutions Plc, London, UK Accepted for publication 9 March 2007 We examine the progress that has been made towards the development of topical treatments for premature ejaculation (PE). Although generally regarded as one of the most common male sexual problems, the lack of approved pharmacological agents for PE means that treatment options are limited to behavioural therapy, where available, and the use of drugs ‘off-label’. There are various theories on the aetiology of PE, but it seems likely that both biological and psychological factors are important. One theory, that men with PE might have a heightened sensory response to penile stimulation, provides the rationale for using topical therapy; reducing the sensitivity of the glans penis with topical desensitizing agents (e.g. local anaesthetics) might improve ejaculatory latency without adversely affecting the sensation of ejaculation. Offlabel topical treatments are now relatively widely used, despite limited supportive efficacy data. There are also new topical treatments in various stages of development, designed specifically for use in PE. Treatments reviewed include TEMPE spray, containing a eutectic mixture of the topical anaesthetics lidocaine and prilocaine, and several creams, including one containing natural products (SS-cream), and preliminary results from another containing the local anaesthetic dylonine, with alprostadil (prostaglandin E1). Despite wide variations in the methods of © clinical trials, it is possible to conclude that all placebo-controlled studies of topical treatments have reported a significant increase in intravaginal ejaculatory latency time compared to baseline and placebo. Topical treatments for PE are appealing in that they can be applied as needed and only minimal systemic effects are likely. However, without well-controlled drug delivery there is the theoretical possibility of penile hypoaesthesia and/or transvaginal contamination. Unlike the cream formulations, the TEMPE spray has a well-controlled delivery system, making it easy to administer locally, and it appears to be well tolerated in early clinical trials. It appears that topical treatments might be able to satisfy many of the requirements of an ideal treatment for PE, and certainly have the potential for use as a first-line treatment. KEYWORDS premature ejaculation, rapid ejaculation, topical treatments, sexual dysfunction, therapy, treatment INTRODUCTION Premature ejaculation (PE; rapid or early ejaculation) is generally regarded as one of 2 0 07 T H E A U T H O R S JOURNAL COMPILATION © 2 0 0 7 B J U I N T E R N A T I O N A L | 1 0 0 , 4 9 3 – 5 0 1 | doi:10.1111/j.1464-410X.2007.07051.x 493 M O R A L E S ET AL. the most common male sexual problems experienced by men in all countries surveyed. In most studies an incidence of 20–30% of men is reported [1–4], although the actual incidence of PE depends on the definition used. Some physicians have even suggested that the prevalence might be as high as 75% [5]. It therefore appears to be a problem affecting many men some of the time and rather fewer all of the time. In practice, most cases of PE are not medically diagnosed, as few men with PE consult a physician. The reasons for this are varied, but are likely to include embarrassment and particularly the belief that there is no effective treatment [6], a view shared by many physicians. There are numerous definitions of PE but one of the most commonly accepted is from the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition [7]. This definition includes an element of self-diagnosis and does not include a set period of delay. However, in practice the intravaginal ejaculatory latency time (IELT) is commonly used as a way of quantifying treatment success and as a standardized way of comparing treatments in clinical research, mostly measured with a stopwatch. There is considerable variation as to where the threshold IELT should be set to define PE in a clinical setting, although the consensus of opinion seems to be that men with PE tend to have an IELT of ≤1–2 min [8–10]. The impact that PE has on quality of life is significant [3], with a similar qualitative impact on the individual as erectile dysfunction (ED) [6]. As a result, there is now general agreement that although IELT comparisons are valuable, in a well-designed clinical trial, treatments should be evaluated in terms of sexual satisfaction (by the man and his partner), and perception of control over ejaculation, in addition to IELT [9,11]. There are currently no pharmacological agents approved for use in PE and all drugs have to be administered ‘off-label’. There are several treatment options for men directed at different components of the complex mechanism of the ejaculatory process. These include behavioural therapy (such as the ‘stop-start’ and ‘squeeze’ techniques), systemic treatments and locally acting topical therapy. Behavioural therapies for PE require a high level of commitment and the involvement of the man’s sexual partner. Although such 494 therapies can be useful for some couples, they are rarely successful in the long term, as most benefits are lost within 3 years of treatment without regular follow-up therapies [12,13]. In addition, the high cost and limited availability of well-trained sex therapists means that this approach is not always a practical first-line treatment, and indeed is unsuitable for men with no steady and supportive sexual partner. Drug therapy (albeit off-label) is therefore often the preferred first-line therapy. SYSTEMIC THERAPIES The AUA currently recommends three drug treatment strategies to treat PE [14]: (i) Daily treatment with serotonergic antidepressants; (ii) as needed treatment with serotonergic antidepressants; (iii) anaesthetic topical treatment. Delayed ejaculation is a common side-effect of many psychotropic or antidepressant drugs. In particular, the selective serotonin reuptake inhibitors (SSRIs) primarily indicated for the treatment of depression can increase the level of serotonin in the brain, inhibiting the ejaculatory reflex centre, and can prolong IELT for several minutes [15,16]. Dosing levels of SSRIs are generally lower for PE than for depression, and various dosing regimens have been tested (including continuous, daily or situational). Despite this the adverse-event (AE) profile appears to be similar, including dry mouth, drowsiness, nausea and reduced libido [17]. There is also the potential for the development of a serious drug interaction that can lead to ‘serotoninergic syndrome’ which manifests as headache, nausea, sweating and dizziness in mild cases, and in hyperthermia, rigidity and delirium in severe cases [17]. Many physicians might consider the side-effects hard to ‘justify’ for the treatment of PE, where the primary outcome is patient satisfaction, although the AUA has suggested that the level of AEs is acceptable for the benefit derived in the patient with PE, and the type and rate of occurrence of side-effects also appears to be acceptable to most patients [14]. Dapoxetine, a novel SSRI, is the first oral agent specifically developed for managing PE, and it was shown to be effective, well tolerated and suitable for on-demand use [18]. Further research with this drug continues despite the US Food and Drug Administration’s apparent refusal to approve dapoxetine for treating PE [19]. RATIONALE FOR THE USE OF TOPICAL TREATMENT There are various theories on the aetiology of PE [9]. Historically, PE was considered to be a learned behaviour and as a result, behavioural therapy was the standard treatment. However, it is now generally accepted that both biological and psychological factors are important in the aetiology of PE. Men with PE appear to have a heightened sensory response to penile stimulation, with a vibration threshold significantly lower than that of normal men [20,21]. They also generally have other abnormal autonomic reflex pathways for the ejaculatory process, including shorter bulbocavernosal latency time, and higher bulbocavernosal evoked potentials [21–23]. Should this be the case, drugs which selectively produce some degree of penile desensitization or act within the afferentefferent reflex arc should be effective therapy for PE. The use of local anaesthetic treatment to delay ejaculation is indeed the oldest form of pharmacological therapy for PE, and was first described by Schapiro in 1943 [24]. The hypothesis is that reducing the sensitivity of the glans penis with topical desensitizing agents (e.g. local anaesthetics) would delay ejaculatory latency without adversely affecting the sensation of ejaculation. This has led to the ‘off-label’ use of one product marketed for another indication, as well as the development of novel topical agents specifically designed to treat PE. Within this context such off-label use of topical treatments for PE is now relatively widespread, and available in cream, ointment and spray formulations. The issue for physician and patient is whether, in the present climate of evidence-based medicine, there is adequate supportive clinical data. Comparative efficacy data for topical treatments, where available, are presented in Table 1 [25–30]. Compared to systemic treatments for PE, topical treatments are appealing in that they can be applied on an ‘as needed’ basis and systemic side-effects are likely to be minimal. However, in applying a local anaesthetic to the penis there is of course the theoretical possibility of penile hypoaesthesia, and © JOURNAL COMPILATION © 2 0 07 T H E A U T H O R S 2 0 07 B J U I N T E R N AT I O N A L TOPICAL TREATMENTS FOR PREMATURE EJACULATION TABLE 1 Comparative efficacy and adverse event data for clinical trials of topical treatments for PE N completing study Baseline IELT, (mean age, years) mean (SD) min Follow-up IELT (mean), min Applied to glans penis and penile shaft 30 min before intercourse; covered with condom 111 (36) ND ND 5/11 excellent 4/11 better 2 no change2 1/11, numbness of penis [37] 2.5 g (placebocontrolled, dose-finding 4 groups ×10 men; 3 applying 2.5 g, covered with condoms and waiting 20, 30 or 45 min, + placebo group 403 (29.4) <1 min Placebo 1.0 20 min 6.71 (2.54) 30 min 8.7 (1.7) 45 min loss of erection in all ND 16/40 erection loss (numbness) 6/10 in 30-min 10/10 in 45-min [38] Double-blind, placebocontrolled Thin layer applied to 294 (completed glans penis and up study) placebo to 2 cm penile shaft; (32.3) covered with EMLA (33.4) condom for 10–12 min Placebo 1.67 (0.7) Placebo 1.95 (0.12) EMLA 1.49 (0.9) EMLA 8.45 (0.9) P < 0.001 (placebo vs EMLA) Great/excellent5 EMLA 11/16 Placebo 3/13 Men, all, 17% (5/29)6 Instructed to apply 3–5 113 (42) sprays (30–50 mg) direct onto glans penis – in situ for 15 min; wipe off before contact with partner 1.4 (1.1) 11.35 (10.72) P = 0.008 vs baseline 8/11 better/much better2 7/11 partners better/much better2 Men7 3/11 Women 2/11 Instructed to apply 3–5 543 sprays (30–50 mg) TEMPE (38.5) direct to glans penis, Placebo (39.3) in situ for 15 min; wipe off before contact with partner TEMPE 1.0 (1.2) Placebo 0.9 (0.7) TEMPE 4.9 (4.9) Mean change in Placebo 1.6 (1.6) SQoL points P < 0.01 vs baseline baseline to end of treatment8 Men: TEMPE 7.0 Placebo 5.5 (P = 0.48) Women TEMPE 3.3 Placebo 1.8 (P = 0.56) TEMPE 3/26 hypoasthesia 1/26 ED Women 1/26 mild burning sensation Not stated Plac 2.34 (0.34) Dyclo 3.21 (0.31) Alpro 3.75 (0.34) Dyclo/alpro 4.08 (0.31) P < 0.05 vs placebo Placebo 5% Dyclo 17.5% Alpro 20% Dyclo/alpro 17.5% Ref Treatment EMLA cream [36] 2.5 g (pilot study) Methods TEMPE spray [29] 30–50 mg (proof of concept) [30] 30–50 mg (doubleblind, placebocontrolled) Dyclonine/alprostadil cream [28] Comparison ‘to the tip of the penis’ 309 (28–62) (i) dyclonine 1%, at the meatus’ (ii) alprostadil 5–10 min before 0.4% coitus (iii) dyclonine 0.5%/ alprostadil 0.4% (placebocontrolled) All AEs local and mild to moderate © Satisfaction (man) % ‘yes’ to PSQ in diary Placebo 66.7 Dyclo 73.3 Alpro 83.3 Dyclo/alpro 86.7 AE details, incidence 2 0 07 T H E A U T H O R S JOURNAL COMPILATION © 2 0 07 B J U I N T E R N AT I O N A L 495 M O R A L E S ET AL. TABLE 1 Continued N completing study Baseline IELT, (mean age, years) mean (SD) min Follow-up IELT (mean), min Applied 1 h before sexual contact; washed off before intercourse 18610 (42.3) 1.50 (0.58) 10.89 (5.60) P < 0.001 vs baseline Satisfaction with treatment11 Not satisfied 10.8% Satisfied 89.2% Overall 5.9% (11/186) 7/186 mild local irritation 4/186 delayed ejaculation [26] 0.05 g 0.10 g 0.15 g 0.20 g (placebocontrolled) Applied 1 h before sexual contact; washed off before intercourse 503 (37) 1.35 (0.07) Plac 2.27 (0.32) 0.05 g 4.47 (0.81) 0.10 g 5.34 (0.79) 0.15 g 6.22 (0.87) 0.20 g 11.06 (1.17) SSR12 Plac 26% 0.05 g 60% 0.10 g 70% 0.15 g 78% 0.20 g 90% All test trials 14.8% (37/250), mild local burning sensation; 0.04% (1/250), mild penile pain; reports of mild local burning sensations increased in a dose-dependent fashion [27] 0.2 g (doubleblind, placebocontrolled) Applied 1 h before sexual contact; washed off before intercourse 106 (38.7) 1.37 (0.12) Plac 2.45 (0.29) SS 10.92 (0.95) P < 0.001 (between treatments) SSR13 Plac 19.81 SS 82.2% All test trials 14.7% (78/530)14, mild burning 3.8% (20/530), mild pain 18.5% (98/530) Ref Treatment SS-cream [25] 0.1 g Methods Satisfaction (man) AE details, incidence ND = not done; 1Patients with self-diagnosed PE; history of primary or secondary PE not stated. 2Satisfaction assessed on a scale of −1 for worse, 0 for no change, 1 for better than usual, 2 for excellent; 3Self-diagnosed primary PE; 4Patients with self-diagnosed primary and secondary PE; 5Level of satisfaction defined using a linear scale pf 1–10, as bad (1–4), regular (5,6), good (7), great (8,9) or excellent (10); 6Men, 2/29 retarded ejaculation, 2/29 loss of sensitivity, 2/29 penile irritation; Women 1/29 decreased vaginal sensitivity; 72/11 numbness of penis, 1/11 burning sensation on first use, 3/11 difficulty maintaining erection in 15 min wait; women 2/11 numbness of vagina; 8Study-specific male and female sexual quality-of-life questionnaires, each containing 10 statements; 9Entry criteria not stated; 10132 with primary PE and 54 with secondary PE, and including 64 patients with PE combined with mild ED; 11Patients were asked to estimate the degree of satisfaction for both their partners and themselves; 12SST, sexual satisfaction ratio; method of determining sexual satisfaction not stated; 13SSRs determined by adding the percentage of patients who reported being satisfied (effective) and very satisfied (excellent); 14total patients 3/106 ED, 4/106 delayed ejaculation, 5/106 no ejaculation. transvaginal contamination and female genital anaesthesia, unless drug delivery is well-controlled; comparative data on such AE, where available, are also presented in Table 1. ‘SEVERANCE SECRET-CREAM’ (SS-CREAM) Severance Hospital in Korea, is made with extracts from nine natural products. Some of these products have local anaesthetic as well as vasoactive properties. Several studies using SS-cream on men with PE were conducted in Korea, but the cream is not approved for use in Europe or the USA, and is not legally available outside Korea. SS-cream (Cheil Jedan Corporation, Seoul, Korea), developed at the Yong-Dong SS-cream is applied to the glans penis 1 h before intercourse and washed off 496 immediately before coitus. Both the latency and amplitude of somatosensory evoked potentials measured at the glans penis were increased over baseline after applying SScream [31], which has also been shown to increase the penile vibratory thresholds at the glans penis in a dose-dependent fashion [32]. Xin et al. [25] reported significantly prolonged ejaculatory latency in 89.2% of patients treated with SS-cream. AEs were noted in 5.9% of patients, which included mild local © JOURNAL COMPILATION © 2 0 07 T H E A U T H O R S 2 0 07 B J U I N T E R N AT I O N A L TOPICAL TREATMENTS FOR PREMATURE EJACULATION irritation (local burning or pain) and delayed ejaculation. The prolongation of IELT was shown to be dose-dependent [26], with an optimal dose of 0.2 g cream. In a multicentre double-blind study involving 106 patients, the use of 0.2 g of SS-cream was reported to increase the mean stopwatchmeasured IELT from a baseline of 1.37 min to 10.92 min, compared to 2.45 min with placebo (P < 0.001), and was 27 times more effective than placebo in increasing sexual satisfaction (P < 0.001). However, almost 19% of episodes of use were associated with mild localized irritation, including pain and burning, and 12 patients reported negative sexual side-effects such as delayed ejaculation, anejaculation and ED [27]. Despite these promising results, SS-cream has an unpleasant smell and colour, which makes it unacceptable to many patients. A reformulation has resulted in ‘renewed SS-cream’ which is a new topical agent composed of the two main components of the original SS-cream, i.e. Korean ginseng and bufonis venenum in a hydrobase and enhancer with no smell or colour [33]. So far, only the results of animal studies have been published. The authors claim that renewed SS-cream delays the latencies of the spinal somatosensory evoked potentials in rabbits more effectively than the original SS-cream. However, the ingredient Bufonis venenum has been shown to produce contact dermatitis [34] and the likelihood of this cream gaining regulatory approval outside Korea appears to be remote. DYCLONINE/ALPROSTADIL CREAM Dyclonine, a local anaesthetic used most commonly in dentistry, has been combined in a cream formulation with alprostadil (prostaglandin E1; a vasodilator used in treating ED), and is under development (NexMed Inc, USA) as a topical treatment for PE. So far only one pilot study has been published (in abstract form) in which creams containing dyclonine alone, alprostadil alone or dyclonine/alprostadil combined, with two different drug concentrations, were compared in a double-blind cross-over trial [28]. This pilot study involved 30 patients who applied the cream 5–20 min before intercourse. There was a significant synergistic effect with the cream containing 0.5% dyclonine/0.4% alprostadil compared with creams containing © 1% dyclonine alone or 0.4% alprostadil alone (P < 0.05; Table 1). Baseline IELTs were unfortunately not reported, but the mean IELTs after dosing were 2.34 and 4.08 min in the placebo and dyclonine/alprostadil combination groups, respectively (P < 0.05). AEs were reported by 17.5% of men and were described as local, mild to moderate and with a mean duration of 18.2 min. Details of the AEs and whether or not any of the patients’ partners had AEs were also not provided. The most frequently reported AE in patients using alprostadil cream to treat ED are application site-related, e.g. penile burning, genital pain and genital erythema, mostly resolving within 2 h [35]. LIDOCAINE-PRILOCAINE CREAM Separately, lidocaine and prilocaine are crystalline solids, but when mixed together in equal quantities by weight they form a liquid eutectic mixture which can be formulated into preparations without the use of a non-aqueous solvent. This allows higher concentrations of anaesthetic to be formulated into the preparation and maintained during application. The eutectic mixture of local anaesthetic (EMLA, AstraZeneca, UK) is a local anaesthetic cream containing 2.5% each of lidocaine/ prilocaine for topical application. Developed to anaesthetize intact skin, it is available as an ‘over-the-counter’ product in some countries. The first pilot study evaluating lidocaineprilocaine cream for treating PE included 11 men [36]; the cream (2.5 g) was applied to the whole glans and shaft of the penis 30 min before intercourse and covered with a condom, which could be removed before intercourse (and the cream wiped off) if desired. Nine of the 11 patients rated their performance as ‘excellent’ or ‘better’ and all 11 partners were satisfied with the treatment results [36]. To determine the optimum time that the anaesthetic cream should be on the penis before intercourse, Atikeler et al. [37] carried out a placebo-controlled trial with 10 patients in each treatment group, varying the application time from 20 to 45 min, with a condom. In the 20- and 30- min groups the IELT increased compared with placebo, but all men in the 45-min group had penile numbness and loss of erection. The optimum application time was considered to be 20 min. The largest double-blind clinical trial of lidocaine-prilocaine cream to date involved 42 patients, 21 in each group [38]. Patients were asked to apply a thin layer of cream to the glans penis, extending the coverage for up to 2 cm on the penile shaft. They were then asked to cover the cream with a condom for 10–20 min before intercourse and to use this treatment each time they had intercourse over 30–60 days. The treatment resulted in a 5.6-fold increase in IELT. However, only 29 of the initial 42 participants completed the study. Of the patients completing the study, 11 of 16 reported ‘great’ or ‘excellent’ sexual satisfaction. Loss of penile sensation, retarded ejaculation and penile irritation were a problem for five men, and one female partner reported decreased vaginal sensitivity. It can be concluded that lidocaine-prilocaine cream has some efficacy in the treatment of PE but is cumbersome and slow-acting. Genital hypoaesthesia in both partners has been reported. LIDOCAINE SPRAY Lidocaine 9.6% spray, marketed as ‘Studd 100’ or ‘Premjact’, has been available over the counter for over 25 years in some countries, and as their names suggest, are marketed as products for delaying ejaculation. However, the absence of reliable data from clinical trials means that the validity of the claims by the manufacturers cannot be assessed. PRILOCAINE-LIDOCAINE SPRAY TEMPE (Topical Eutectic Mixture for Premature Ejaculation, Plethora Solutions Plc, London, UK) is a proprietary formulation of lidocaine and prilocaine in a metered-dose aerosol-delivery system specifically designed for use in PE, delivering 7.5 mg lidocaine base plus 2.5 mg prilocaine base per actuation. The mixture is alcohol-free so there is little risk of stinging on application, and although oil-free, the mixture forms a clear, slightly oily, odourless solution that remains adherent to the application site. It can easily be wiped off if necessary with a damp cloth, so no condom is required [29]. 2 0 07 T H E A U T H O R S JOURNAL COMPILATION © 2 0 07 B J U I N T E R N AT I O N A L 497 M O R A L E S ET AL. The metered-dose spray-delivery system allows the desensitizing agents to be deposited in a dose-controlled, concentrated film on the glans penis, which can then penetrate the glans within 5–10 min [29] (Fig. 1). The eutectic mixture is less capable of penetrating intact keratinized skin and as such is less likely to anaesthetise the shaft of the penis or the hands [30]. FIG. 1. The mode of action of TEMPE. TEMPE aerosol spray contains purely base (uncharged) forms of local anaesthetics whilst creams contain a mixture of base and ionised forms. Only the uncharged base forms are able to penetrate skin or mucous membranes. Local anaesthetics produce localized reversible inhibition of nerve conduction by reducing the permeability of the neuronal membranes to sodium ions, the movement of which is necessary for the transmission of nerve impulses. Effective delivery = layer of pure LA base at a pH close to the pKa of the drug Aerosol spray Cream/ointment In the first open-label pilot study, 11 patients recorded stopwatch-timed IELTs at baseline and on five subsequent encounters when using the spray 15 min before intercourse. The average IELT increased from 1.4 min to 11.35 min (P = 0.008), representing a mean eight-fold increase over baseline. In addition, eight of the 11 patients and seven of 11 partners rated their sexual satisfaction as ‘better’ or ‘much better’. LA un-ionised LA ionised Proton axon 10 8 6 4 2 7] [2 g [2 0.2 g SS –c re am 0.2 SS –c re am 0.1 SS –c re am re am –c SS 6] 6] g 5 g 0.1 5 0.0 re am –c sp ra SS [2 [2 6] 6] g in m 15 g m 50 0– y3 [2 [3 [3 in m 12 0– r1 lay e in EM TE M PE th 498 0] 8] 0 LA Whilst phosphodiesterase-5 inhibitors such as sildenafil are highly effective in treating ED, their use for treating PE is limited to patients with ED and coexisting PE, and none of the current guidelines for managing PE include these inhibitors as first-line agents. A study comparing the use of lidocaine-prilocaine cream in PE to lidocaine-prilocaine combined Improvement over placebo Placebo Baseline 12 A summary of the potential of topical agents as monotherapy is shown in Fig. 2 [26,27,30,38]. All placebo-controlled studies reviewed here reported a significant increase in IELT for topical treatments compared to baseline or placebo. Figure 2 shows the mean increase in IELT over baseline and placebo for placebo-controlled trials, but differences between studies should be interpreted cautiously due to differences in methods, as detailed in Table 1. TOPICAL TREATMENTS AS AN ADJUNCT TO ORAL THERAPY Na+ channel FIG. 2. Improvements in IELT over baseline/placebo in placebo-controlled trials of topical agents to treat PE. IELT min In a recently published phase II, placebocontrolled trial [30], 54 patients using TEMPE were able to prolong their IELT from a baseline of 1.0 min to 4.9 min. The treatment was also well tolerated, with only three patients (12%) experiencing hypoaesthesia (numbness of the penis) and a fourth having ED, none resulting in treatment discontinuation. TEMPE was also well tolerated by the female partners, with only one partner experiencing a mild burning sensation during intercourse each time her partner used the spray, which did not result in discontinuation. Mucous Membrane with oral sildenafil, in which patients selfassessed their improvement, showed that there was no statistical advantage in adding sildenafil to topical prilocaine-lidocaine treatment [39]. Similarly, lidocaine ointment has been used in combination with the SSRI fluoxetine taken daily [40] or ‘as needed’ [41]. Although the authors claim that the combined treatment is more effective than the SSRI alone, neither study included either lidocaine-only or placebo groups, meaning that the results are of limited value. It appears that it is generally unnecessary to think of topical treatments as an adjunct to oral therapy for PE, as they tend to be effective when used alone. © JOURNAL COMPILATION © 2 0 07 T H E A U T H O R S 2 0 07 B J U I N T E R N AT I O N A L TOPICAL TREATMENTS FOR PREMATURE EJACULATION FIG. 3. Management algorithm for PE, modified from McMahon et al. [9] Patient complaining of premature ejaculation (PE) Patient/Partner History • • • • • • • • Establish presenting complaint Intravaginal Ejaculatory Latency Time Perceived degree of ejaculatory control Degree of patient/partner distress Onset and duration of PE Psychosocial history Medical history Physical examination requires a 20-min application of the cream, covered with a condom [37]. In comparison, TEMPE spray is easy to administer locally, remains adherent to the glans penis after application, and by exploiting the properties of a eutectic mixture, the local anaesthetic is less likely to penetrate intact keratinized skin and will not anaesthetize the shaft of the penis [30]. Importantly, with TEMPE spray no condom is required, as long as it is wiped off before the penis comes into contact with the partner. TREATMENT ALGORITHM Manage primary cause PE secondary to ED or other sexual dysfunction Yes No Acquired Lifelong PE Treatment First Line Pharmacotherapy • SSRI agents • Topical agents Second Line Behavioural Therapy • Stop/start • Squeeze technique • Sensate Focus Relationship counselling OR Combination Treatment Attempt graduated withdrawal of pharmacotherapy after 6 to 8 weeks ADVANTAGES AND DRAWBACKS OF TOPICAL TREATMENT Compared to systemic treatments for PE, topical treatment can be applied when needed and systemic side-effects are unlikely, although they have several potential drawbacks; they can be messy, interfere with spontaneity and can possibly cause hypoaesthesia in the man and/or his partner. Depending on the formulation, they also require a period of time between application and maximum effect, and need to either be used with a condom or for the product to be washed or wiped off before intercourse, which might decrease arousal and reduce spontaneity. However, there are differences among the products. The lidocaine-prilocaine cream © Current recommendations from the AUA [14] and the Second International Consultation on Sexual Dysfunctions (ICSD) [9] recognize that PE is a self-reported diagnosis and emphasize the important role of obtaining a comprehensive sexual history when making a diagnosis, i.e. no laboratory or physiological tests are usually required. It is recommended that clinicians also determine if there is concomitant ED and, if present, it should be treated first [9,14]. The management algorithm for PE produced by the ICSD recommends pharmacotherapy with SSRI or topical anaesthetics as the first-line treatment in patients with lifelong PE, and second-line, after behavioural therapy, in patients with acquired PE [9]. In reality, pharmacotherapy is likely to be used as the first line in both cases, due to the limited availability of skilled behavioural therapists and relationship councillors. The choice between oral therapy with SSRI (daily or ‘asneeded’), or the use of a topical agent is a decision to be made jointly by the patient/ couple and physician, after ascertaining their desires and expectations. If acceptable to the patient/couple, a trial of a topical agent could be a prudent first step due to the favourable risk/benefit ratio of these products. This is reflected in the proposed treatment algorithm shown in Fig. 3. DISCUSSION Historically, the first-line treatment for PE has been behavioural, as was originally the case with ED, but the last decade has seen an increase in the pharmacological treatment of PE, coupled with an increase in the number of published studies on PE. As would be expected for a condition where there has traditionally been considerable debate over the definition, there is also considerable variation in the methods used in these studies. A critical review of the methods of studies in PE [42] showed the scale of the differences and the resultant difficulties in comparing results from these studies. It is therefore important to exercise some caution when comparing ‘headline’ results. Recommendations for standards for clinical trials in PE [9,11,42] include: the use of a precise definition of PE (e.g. ‘ejaculation that occurs within 1 min after vaginal penetration in >90% of attempts’); a randomized double-blind prospective design; the use of validated outcome measures (such as IELT and patient reported outcomes); and the use of a stopwatch at each coitus, both during baseline and during drug treatment. Use of such standardized variables in all future trials would enable a meaningful meta-analysis. CHARACTERISTICS OF AN IDEAL TREATMENT As the frequency of sexual intercourse is highly variable, and spontaneity in sexual intercourse is usually an important factor, the ideal treatment for PE would be a discrete and ‘on-demand’ therapy with rapid action, effective from the first dose and with high efficacy on IELT and patient-reported outcomes, a low incidence of side-effects, and have no unwanted effects on the partner [15]. It was also suggested that medication could be used to restore confidence together with behavioural treatment, where available, to help men learn to overcome PE on their own [43,44]. PE is of course not a life-threatening condition; therefore safety should be a primary consideration when deciding on a course of treatment [14]. PE is a self-diagnosed condition and most men with the condition do not seek treatment from a physician, for reasons of embarrassment, shame or the belief that no effective treatment exists, but they might try self-help techniques or self-medication. In a large multinational survey of >11 500 men in the USA, Italy and Germany, <12% of men who self-reported PE had sought professional treatment [45]. In a small survey involving indepth interviews with 28 men with selfdiagnosed PE, 89% had tried some form of treatment (including behavioural, pharmaceutical, over-the-counter remedies, herbal remedies, creams and condoms), regardless of whether or not they had consulted a healthcare professional [6]. Such 2 0 07 T H E A U T H O R S JOURNAL COMPILATION © 2 0 07 B J U I N T E R N AT I O N A L 499 M O R A L E S ET AL. a high figure clearly indicates that men with PE are highly motivated to seek a solution or treatment, and that most men/couples at present self-diagnose and therefore self-treat their PE. Unfortunately, the interest and understanding of the condition by physicians in general and specialists in particular is erratic at best and superficial to non-existent at worst. This in part is due to the lack of large, welldesigned studies showing reliable values for safety and efficacy of many of the treatments available. The demand for treatment for PE is growing, perhaps due to changes in expectation of sexual fulfilment by both sexual partners. Until effective products are licensed for treating PE, patients (or indeed any man wanting to extend his IELT) will continue to turn to over-the-counter products of questionable efficacy and safety, and solely based on the manufacturers’ claims but with limited supporting evidence. 7 8 9 10 11 CONFLICT OF INTEREST 12 James Barada and Alvaro Morales are Consultants to, and Study Investigators, for Plethora Solutions. Michael Wyllie is a Board Member of Plethora Solutions. 13 REFERENCES 1 2 3 4 5 6 Reading A, Weist W. An analysis of selfreported sexual behaviour in a sample of normal males. Arch Sex Behav 1984; 13: 69–74 Frank E, Anderson C, Rubinstein D. Frequency of sexual dysfunction in ‘normal’ couples. N Eng J Med 1978; 299: 1111–5 Rowland D, Perelman M, Althof S et al. Self-reported premature ejaculation and aspects of sexual functioning and satisfaction J Sex Med 2004; 1: 225–32 Dunn KM, Croft PR, Hackett GI. Sexual problems: a study of the prevalence and need for health care in the general population. Family Pract 1998; 15: 519–24 McMahon CG. Treatment of premature ejaculation with sertraline hydrochloride: a single-blind placebo-controlled crossover study. J Urol 1998; 159: 1935–8 Symonds T, Roblin D, Hart K. How does premature ejaculation impact a man’s life? J Sex Marital Ther 2003; 29: 361–70 500 14 15 16 17 18 American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 4th edn. Text Revision. Washington DC: American Psychiatric Association, 2000 Waldinger MD, Quin P, Dileen M, Mundayat R, Schweitzer DH, Boolell M. A multinational population survey of intravaginal ejaculatory latency time. J Sex Med 2004; 2: 492–7 McMahon CG, Abdo C, Incrocci L et al. Disorders of orgasm and ejaculation in men. In Lue TF, Basson R, Rosen R, Guiliano R, Khoury S, Montorsi F eds. Sexual Medicine: Sexual Dysfunctions in Men and Women. Edition 21. Paris: 2005: 411–68 Patrick D, Althof S, Pryour J et al. Premature ejaculation. an observational study of men and their partners. J Sex Med 2005; 2: 358–68 Hirsch M, Donatucci C, Glina S, Montague D, Motorsi F, Wyllie M. Standards for clinical trials in male sexual dysfunction. Erectile dysfunction and rapid ejaculation. J Sex Med 2004; 1: 87– 91 De Amicus LA, Goldberg DC, Lo Piccolo J, Friedman J, Davies L. Clinical followup of couples treated for sexual dysfunction. Arch Sex Behav 1985; 14: 467–89 Metz M, McCarthy B. Coping with Premature Ejaculation: How to Overcome PE, Please Your Partner & Have Great Sex. Oakland, CA: New Harbinger, 2003 Montague D, Jarrow J, Broderick GA et al. The AUA Erectile Dysfunction Guideline Update Panel. AUA guideline on the pharmacologic management of premature ejaculation. J Urol 2004; 172: 290–4 Hellstrom W. Current and future pharmacotherapies of premature ejaculation. J Sex Med 2006; 3 (Suppl. 4): 332–41 Girgis S, El-Haggar S, El-Hermouzy S. A double-blind trial of clomipramine in premature ejaculation. Andrologia 1982; 14: 364–9 Sharlip ID. Guidelines for the diagnosis and management of premature ejaculation. J Sex Med 2006; 3 (Suppl. 4): 309–17 Pryor J, Althof S, Steidle C, Miloslavsky M. Efficacy and tolerability of dapoxetine in the treatment of premature ejaculation. J Urol 2005; 173: 201 19 AZLA Corporation: press release. Available at http://www.jnj.com/news/ jnj_news/20051026_164127.htm. Accessed April 2007 20 Rowland DL, Haensel SM, Blom JH, Slob AK. Penile sensitivity in men with premature ejaculation and erectile dysfunction. J Sex Marital Ther 1993; 19: 189–97 21 Xin ZC, Chung WS, Choi YD, Seong DH, Choi YJ, Choi HK. Penile sensitivity in patients with primary premature ejaculation. J Urol 1996; 156: 979–81 22 Vignoli GC. Premature ejaculation: New electrophysiologic approach. Urology 1978; 11: 81–2 23 Xin ZC, Choi YD, Rha KH, Choi HK. Somatosensory evoked potentials in patients with primary premature ejaculation. J Urol 1997; 158: 451–5 24 Schapiro B. Premature ejaculation, a review of 1130 cases. J Urol 1943; 50: 374 25 Xin ZC, Choi YD, Lee SH, Choi HK. Efficacy of a topical agent SS-cream in the treatment of premature ejaculation: preliminary clinical studies. Yonsei Med J 1997; 38: 91–5 26 Choi HK, Xin ZC, Choi YD et al. Safety and efficacy study with various doses of SS-cream in patients with premature ejaculation in a doubleblind, randomized, placebo controlled clinical study. Int J Impot Res 1999; 11: 261–4 27 Choi HK, Jung GW, Moon KH et al. Clinical study of SS-cream in patients with lifelong premature ejaculation. Urology 2000; 55: 257–61 28 Gittleman MC, Mo J, Lu M. Synergistic effect of meatal application of dyclonine/ alprostadil cream for the treatment of early ejaculation (EE) in a double-blind and crossover study. Presented at the 8th Congress of the European Society for Sexual Medicine, Copenhagen, Denmark December 4–7, 2005. J Sex Med 2006; 3 (Suppl 3): 176 29 Henry R, Morales A. Topical lidocaineprilocaine spray for the treatment of premature ejaculation: a proof of concept study. Int J Imp Res 2003; 15: 277–81 30 Dinsmore WW, Hackett G, Goldmeier D et al. Topical eutectic mixture for premature ejaculation (TEMPE): a novel aerosol-delivery form of lidocaineprilocaine for treating premature ejaculation. BJU Int 2007; 99: 369–75 © JOURNAL COMPILATION © 2 0 07 T H E A U T H O R S 2 0 07 B J U I N T E R N AT I O N A L TOPICAL TREATMENTS FOR PREMATURE EJACULATION 31 Xin ZC, Choi YD, Seong DH, Choi HK. Sensory evoked potential and the effect of SS-cream in premature ejaculation. Yonsei Med J 1995; 36: 397–401 32 Xin ZC, Choi YD, Lee WH et al. Changes in ejaculatory latency and penile vibratory threshold with SS-cream in patients with primary premature ejaculation. Sex Dyfunction 1998; 1: 89–93 33 Tian L, Xin ZC, Xin H et al. Effect of renewed SS-cream on spinal somatosensory evoked potentials in rabbits. Asian J Androl 2004; 6: 15–8 34 Lee TY, Lam TH. Irritant contact dermatitis due to a Chinese herbal medicine lu-shen-wan. Contact Dermatitis 1988; 18: 213–8 35 Padma-Nathan H, Yeager JL. An integrated analysis of alprostadil topical cream for the treatment of erectile dysfunction in 1732 patients. Urology 2006; 68: 386–91 36 Berkovitch M, Kerestechi AG, Koren G. Efficacy of prilocaine-lidocaine cream in the treatment of premature ejaculation. J Urol 1995; 154: 1360–1 37 Atikeler MK, Gecit I, Senol FA. Optimum usage of prilocaine-lidocaine cream in premature ejaculation. Androlog 2002; 34: 356–9 © 38 Busato W, Galindo CC. Topical anaesthetic use for treating premature ejaculation: a double-blind, randomized, placebo-controlled study. BJU Int 2004; 93: 1018–21 39 Atan A, Basar MM, Tuncel A, Ferhat M, Agras K, Tekdogan U. Comparison of efficacy of sildenafil-only, sildenafil plus topical EMLA cream, and topical EMLA-cream-only in treatment of premature ejaculation. Urology 2006; 67: 388–91 40 Atan A, Basar MM, Aydoganli L. Comparison of the efficacy of fluoxetine alone vs fluoxetine plus lidocaine ointment in the treatment of premature ejaculation. Arch Esp Urol 2000; 53: 856– 8 41 Metin A, Kayigil Ö, Ahmed SI. Does lidocaine ointment increase fluoxetine efficacy in the same group of patients with premature ejaculation? Urolog Int 2005; 75: 231–4 42 Waldinger MD. Towards evidence-based drug treatment research on premature ejaculation: a critical evaluation of methodology. Int J Imp Res 2003; 15: 309–13 43 Altof SE. Prevalence, characteristics and implications of premature ejaculation/ rapid ejaculation. J Urol 2006; 175: 842–8 44 Perelman MA. A new combination treatment for premature ejaculation: a sex therapist’s perspective. J Sex Med 2006; 3: 1004–12 45 Porst H. Factors related to seeking treatment for premature ejaculation. results from the Premature Ejaculation Prevalence and Attitudes (PEPA) Survey. Presented at the 7th Congress of the European Society for Sexual Medicine, London, UK, December 5–8, 2004. J Sex Med 2005; 2 (Suppl. 1): 1–87 Correspondence: Mike Wyllie, Plethora Solutions Plc, London, UK. e-mail: [email protected] Abbreviations: PE, premature ejaculation; IELT, intravaginal ejaculatory latency time; ED, erectile dysfunction; SSRI, selective serotonin re-uptake inhibitor; AE, adverse event; SS-cream, ‘Severance Secret-Cream’; EMLA, eutectic mixture of local anaesthetic; TEMPE, topical eutectic mixture for PE; ICSD, International Consultation on Sexual Dysfunctions. 2 0 07 T H E A U T H O R S JOURNAL COMPILATION © 2 0 07 B J U I N T E R N AT I O N A L 501