Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
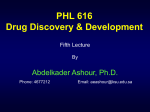
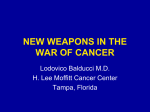
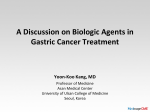
09-CE-SEPT06 8/22/06 12:52 PM Page 1 ce continuing education lesson Targeted drugs for cancer treatment 1.25 CEUs ■ Jennifer Spencer, B.Sc., B.Sc.Pharm., BCOP Sept 2006 Learning objectives Upon successful completion of this lesson, you should be able to: 1. describe new targets for drug therapy in cancer patients 2. manage side effects with these new targeted drugs 3. prevent toxicity or lack of efficacy by anticipating potential drug interactions with these therapies To successfully complete the post-test for this lesson, you may need access to the Compendium of Pharmaceuticals and Specialties (CPS). n 2006, an estimated 153,100 Canadians will be diagnosed with cancer. Approximately 791,400 Canadians are living with some form of cancer.1 Depending on the type of malignancy, traditional treatment options have included surgery, radiation, hormonal therapy and chemotherapy. The promise of increased survival has made undergoing these treatments worth the risk of their adverse effects.2 With the advent of molecular biology, a new era in cancer treatment has begun. Targeted drug therapy has created a completely novel approach to treatment. This lesson will provide pharmacists with the mechanistic background behind these newer agents and information on the management of their side effects and drug interactions. I Targeted drug therapy Traditional cytotoxic chemotherapy was developed to take advantage of the fact that tumour cells divide more rapidly than other cells. Unfortunately, many other healthy cells in the body turn over rapidly, such as the lining of the gastrointestinal tract, white blood cells and hair. This lack of specificity results in many of the side effects associated with chemotherapy, such as the development of mouth ulcers, potential for infection and hair loss. Molecular biology has allowed us to identify specific targets within tumour tissues. The ideal molecular target is one that functions differently in tumour than in nontumour tissues. In addition, through epidemiologic study, it is important that this molecular target has been identified as a predictor of poor disease outcome.3 Generally, these targets are found in cellular pathways that lead to tumour growth, survival and metastasis. Due to their specificity, drugs that target these cellular pathways do not exhibit the same toxicity profile as traditionally seen with conventional chemotherapy treatments. Three such targets include transmembrane proteins called tyrosine kinases, Instructions 1. After carefully reading this lesson, study each question and select the one answer you believe to be correct. Circle the appropriate letter on the attached reply card. 2. To pass this lesson, a grade of at least 70% (14 out of 20) is required. If you pass, your CEU(s) will be recorded with the relevant provincial authority(ies). (Note: some provinces require individual pharmacists to notify them.) Answering options A. For immediate results, answer online at www.pharmacygateway.ca. B. Mail or fax the printed answer card to (416) 764-3937. Your reply card will be marked and you will be advised of your results within six to eight weeks in a letter from Pharmacy Practice. antibody-directed therapies against cell suface proteins and antibodies directed against new vessel formation (angiogenesis). Receptor tyrosine kinases Tyrosine kinases are transmembrane proteins that have an extracellular ligand binding domain, transmembrane domain and catalytic intracellular domain (Figure 1).4-7 Normally, ligands or molecules bind to these receptors. Binding causes auto-phosphorylation of key tyrosine kinase residues found inside the cell. This then leads to activation of a series of downstream signalling events that mediate cellular proliferation, survival, differentiation, function and motility.5 In certain situations, these tyrosine kinase receptors can be overexpressed or mutated in cells. This results in the cells constantly receiving signals to proliferate. Several tyrosine kinases have been targeted. The epidermal growth factor receptor (EGFR) is a tyrosine kinase receptor that is normally activated by epidermal growth factor (EGF). It is found to be abnormal or overexpressed in many malignancies including head and neck, colorectal, breast, pancreatic, lung and brain cancer.5.8 The EGFR tyrosine kinase is an ideal target because it is involved in cell signalling, induces cancer when it is aberrant, and elevated levels have been found in cancer specimens compared to normal tissue. Overexpression of EGFR is directly related to chemotherapy resistance Supported by an unrestricted grant from 09-CE-SEPT06 8/22/06 12:52 PM Page 2 ce continuing education lesson and poor prognosis.8 Specifically, > 50% of non-small cell lung cancers overexpress EGFR and it is a negative prognostic factor.9 Pre-clinical studies demonstrated that inhibition of EGFR could impair tumour growth.10 This has lead to the development of the currently marketed tyrosine kinase inhibitor, erlotinib. A different tyrosine kinase has also been targeted. In a type of hematological malignancy called chronic myeloid leukemia (CML), a translocation occurs between chromosomes 9:22. This translocation results in a new gene called BCR-ABL, or the Philadelphia chromosome.11 The new gene produces a BCR-ABL tyrosine kinase that is abnormal and constitutively active. When it is always turned on, the leukemia cells multiply in an uncontrolled manner.12 Imatinib is a specific inhibitor of the BCR-ABL tyrosine kinase.13 Targeted drugs for cancer treatment FIGURE 1 Tyrosine kinase receptor6,7 growth factor (e.g.: epidermal growth factor, EGF) extracellular transmembrane cell membrane intracellular tyrosine kinase domain (becomes activated) Antibody-directed therapies against cell surface proteins Specific targets on the extracellular surface of cancer cells have been identified. Through biological engineering, antibodies have been developed that specifically bind to these extracellular surface proteins. When this antibody binds to the receptor, five different possible actions are thought to occur, which result in targeted elimination of the cancer cell. The suggested actions include down-regulation of the receptor, down-regulation of the growth signalling properties, initiation of antibody dependent cellular toxicity, complement dependent cytotoxicity and apoptosis (Figure 2).14-16 This strategy has been used in different malignancies including breast cancer and lymphoma. In breast cancer, 15–25% of patients overexpress the human epidermal growth factor receptor protein-2 (HER2) protein.17 HER2 downstream signalling cellular proliferation overexpression is correlated with higher-grade tumours, relative resistance to certain types of chemotherapy and poorer prognosis.18 A monoclonal antibody called trastuzumab was developed that specifically targets the HER2 receptor.19 The treatment of certain lymphomas has also included the use of antibody-directed therapies. Malignant and nonmalignant B lymphocytes express a cell surface protein called the CD20 antigen.20 Rituximab is a monoclonal antibody that specifically binds to the CD20 positive lymphoma cells. survival cell migration Angiogenesis and vascular endothelial growth factor Angiogenesis is the formation of new blood vessels.21 Tumours are unable to grow beyond two to three millimetres unless they create their own vascular supply.22 Angiogenesis is a multistep process that occurs through the stimulus of many cytokines including vascular endothelial growth factor (VEGF). Angiogenesis is needed for tumours to grow, invade and metastasize. Normal blood vessels are ordered and regulated, while tumour vessels are chaotic and irregular. This irregularity appears to CE Faculty This month Reviewers Targeted drugs for cancer treatment All lessons are reviewed by a minimum of six pharmacists for accuracy, currency and relevance to current pharmacy practice. Author Jennifer Spencer, B.Sc., B.Sc.Pharm, BCOP, is a board certified oncology pharmacist. She works as a clinical pharmacist in the medical oncology department of the Ottawa Hospital and teaches the oncology section of the nursing pharmacology course at the University of Ottawa. 2 Answer online at www.pharmacygateway.ca CE Co-ordinator Brenda McBean Cochran, B.S.P., M.Sc.(Phm) Pharmacist consultant, Bedford, N.S. This lesson (CCCEP file # 428-0606) has been approved for 1.25 CEUs by the Canadian Council on Continuing Education in Pharmacy. Approved for 1.25 CEUs by l’Ordre des pharmaciens du Québec. Accreditation of this program will be recognized by CCCEP until June 16, 2009. This lesson is published by Rogers Publishing Limited, One Mount Pleasant Rd., Toronto, ON M4Y 2Y5. Editorial office: Tel: (416) 764-3927 Fax: (416) 764-3931. CE queries: Tel: (416) 764-3879 Fax: (416) 764-3937 [email protected]. No part of this CE lesson may be reproduced, in whole or in part, without the written permission of the publisher. The authors, expert reviewers and provider state that they have no real or potential conflict to disclose. This lesson is supported by an unrestricted grant from Genpharm Inc. Pharmacy Practice | September 2006 09-CE-SEPT06 8/22/06 12:52 PM Page 3 ce continuing education lesson FIGURE 2 Targeted drugs for cancer treatment Monoclonal antibody targeting a cancer cell14,16 antibody dependent cellular toxicity (phagocytosis) macrophage Erlotinib monoclonal antibody complement binding resulting in cell lysis antigen receptor (i.e., HER-2 protein or CD20) cancer cell intracellular events • down regulation of growth signals • down regulation of receptor • apoptosis FIGURE 3 A. Normal tumour growth. When a growing tumour reaches a certain critical size (0.5–2 mm), it can no longer supply itself with nutrients and oxygen from nearby small blood vessels. In response, the tumour secretes vascular endothelial growth factor (VEGF), which attaches to nearby blood vessels and stimulates growth toward the tumour, allowing it to thrive. B. Effect of bevacizumab on tumour growth. Possible mechanism of action of antibody to vascular endothelial growth factor (VEGF). Antibody to VEGF blocks the signals from the tumour that prompt blood vessel growth. Without nutrients and oxygen, the tumour stops growing. *Reprinted with permission from Hoffmann-La Roche. decrease the ability of chemotherapy to be effectively delivered to the entire tumour.23 Several cancers overexpress VEGF. Elevated levels are associated with a poorer prognosis and higher risk of metastatic disease.23 Bevacizumab is a monoclonal antibody that specifically binds to VEGF (Figure 3). When Pharmacy Practice | September 2006 Specific targeted drug therapies Many targeted therapies are currently available on the Canadian market. The more commonly administered drugs are reviewed in this section. bound to VEGF, it prevents binding of VEGF to the receptor on the endothelial cells, and thus blocks the stimulus for endothelial cell growth and angiogenesis.24 VEGF is an excellent target as angiogenesis is usually dormant in adults except during wound healing, inflammation and female reproductive cycles.25 Erlotinib is approved in Canada for patients with non-small cell lung cancer who have failed at least one prior chemotherapy regimen. It inhibits the EGFR tyrosine kinase (Figure 1). Most patients with non-small cell lung cancer are diagnosed with advanced disease. Median survival is eight to 10 months. There has been little progress in improving the efficacy of treatment options in the last 20 years.26 Second-line chemotherapy provides a response rate of 20% and prolongs survival by two to four months.27 Newer treatment options were desperately needed. Erlotinib was studied as a second- or thirdline treatment. The BR-21 trial included 731 patients randomized in a 2:1 ratio to erlotinib 150 mg po daily or placebo.28 Overall response rates were nine per cent in the erlotinib group and < 1% in the placebo arm. Erlotinib provided a significantly longer overall survival of two months as compared to placebo (6.7 vs. 4.7 months). This was the first trial showing a survival advantage of a tyrosine kinase inhibitor after second- or third-line chemotherapy in non-small cell lung cancer.28 Of interest, higher response rates were correlated with female, nonsmoker and Asian groups, and those tumours with adenocarcinoma histology (a subset of non-small cell cancer patients). Erlotinib is also being studied in other malignancies including colorectal cancer, cancer of the pancreas and renal carcinoma. Dosing Erlotinib is given as a 150 mg tablet orally daily on an empty stomach. Food increases the bioavailability from 59% to 100%. The higher bioavailability when taken with food may result in more side effects without an increase in efficacy.27 Metabolism of erlotinib is primarily through the cytochrome P450 CYP3A4. Potent inducers (i.e., rifampin, phenobarbital, carbamazepine, phenytoin, St John’s wort) may decrease erlotinib levels and may compromise its efficacy. Inhibitors (i.e., itraconazole, ketoconazole, fluconazole, diltiazem, verapamil, erythromycin, clarithromycin, grapefruit juice) may increase levels, which could result in increased side effects. Erlotinib can also interact with warfarin. Patients who are being initiated on erlotinib should have their INRs followed closely.29 Answer online at www.pharmacygateway.ca 3 09-CE-SEPT06 8/22/06 12:52 PM Page 4 ce continuing education lesson Adverse effects Common side effects with erlotinib include rash (43–85%) and low-grade diarrhea (55%). Of interest, rash has been highly correlated with response.10,30,31 Most cases of rash are mild. It is described as acneiform-like and appears as inflammatory follicular papules and pustules. Acneiform rash is not usually associated with comedones and therefore is not like true acne. The T zone of the facial area, labial folds, forehead and chin are often first affected. The rash can also develop on the upper chest and back. The onset is usually within seven to 10 days of starting therapy. The intensity and severity fluctuates and many lesions will improve on their own, even while continuing on erlotinib.30 If the rash is mild, treatment may not be necessary. If bothersome, anti-acne or antirosacea agents can be tried such as topical metronidazole, erythromycin or clindamycin. Drying agents such as benzoyl peroxide should be avoided. If the lesions become symptomatic and cover < 50% of the body, the topical antiacne treatments, such as those just mentioned above, can be used, as well as an oral antihistamine if the lesions are itchy.10 An oral tetracycline, such as minocycline or doxycyline 100 mg orally daily, can be attempted. Topical steroids can be offered, but should be used sparingly.30 If the rash progresses to > 50% of the body surface and is painful, ulcerative or desquamating, interruption of erlotinib should be seriously considered.10 All previously mentioned treatments can be used, as well as increasing the minocycline or doxycycline dose to 200 mg per day, and then tapered when the acute inflammation has subsided.10 Total treatment duration of the minocycline/doxycycline is three to six weeks.30 Mild diarrhea occurs in 48% of patients, with only six per cent experiencing severe diarrhea.3 Most patients are well-controlled with loperamide. If severe, or the patient develops nausea, anorexia or vomiting associated with dehydration, therapy should be dose reduced or temporarily interrupted.29 Finally, interstitial lung disease can be a rare (0.8%) but serious complication from erlotinib. Therapy should be interrupted at any signs of acute onset or worsening of dyspnea/cough.3,29 Imatinib Imatinib revolutionized the treatment of chronic myelogenous leukemia (CML). It is currently approved for the treatment of adults with Philadelphia chromosome positive CML and a rare tumour called gastrointestinal stromal 4 Answer online at www.pharmacygateway.ca Targeted drugs for cancer treatment tumour (GIST). In CML, imatinib inhibits the abnormal tyrosine kinase that is produced by the genetic translocation that results in the Philadelphia chromosome.32 In a multicentre trial, 1,106 patients with chronic phase CML were randomized to imatinib or to interferon alpha (INF α) and low-dose cytarabine. A major cytogenetic response was seen in 85.2% of patients on imatinib compared to 22.1% in the INF α and cytarabine group (p < 0.001).11 A major cytogenetic response is both a complete or partial response, where 0– < 35% of Philadelphia positive cells are found in the bone marrow.12 Normal bone would not contain any Philadelphia positive cells. Imatinib has also been studied in the accelerated form of CML and provided significant response rates.13 In GIST tumours, a gain of function mutation occurs at the KIT or platelet-derived growth factor alpha (PDGFRA) gene. Imatinib inhibits the resultant abnormal KIT and PDGRFA tyrosine kinases produced from these abnormal genes.33 Dosing Dosing of imatinib for CML is 400 mg orally in the chronic phase and 600 mg orally daily in the accelerated and blast phases. Doses can be increased in both situations by 200 mg, if inadequate response is seen with the initial dose. In GIST, most patients receive 400 mg per day. To decrease the incidence of nausea, imatinib should be taken after a meal with a large glass of water.34 Significant drug interactions can occur with imatinib. A major metabolic pathway for its clearance is through CYP3A4, and it is an inhibitor of CYP2D6. Elevated imatinib levels, due to enzyme inhibition, could result in a higher incidence of adverse effects, including rash. Imatinib levels could be increased by the following substances that inhibit CYP3A4: ketoconazole, erythromycin, clarithromycin, itraconazole, voriconazole and grapefruit juice.34,35 Enzyme induction could lead to decreased imatinib blood concentrations and possibly result in decreased effectiveness. Medications that may decrease imatinib levels are inducers of CYP3A4 including dexamethasone, phenytoin, carbamazepine, rifampin, phenobarbital and St John’s wort.34 Imatinib has also been shown in vitro to inhibit CYP2D6. Substrates for 2D6 include beta-blockers, serotonin H3 antagonists, morphine, oxycodone and cyclophosphamide. Caution is also advised when co-administering medications that are metabolized by CYP2C9, including warfarin. Careful monitoring of INRs is recommended when imatinib is initiated, or with any dose adjustments. Changing to a low-molecular weight heparin or unfractionated heparin should be considered.34 Adverse effects Imatinib is generally well-tolerated. The more frequently reported adverse effects include mild nausea, vomiting, diarrhea, myalgias and muscle cramps. Superficial edema primarily evident as periorbital edema and lower limb edema, is commonly seen (> 50% of patients).34 It is rarely severe and can be managed with diuretics or lowering the dose of imatinib. Pleural effusions, ascites, pulmonary edema and rapid weight gain are usually managed by temporarily withholding the dose and treating with a diuretic. Patients should be weighed regularly and monitored for weight gain. The likelihood of edema is more likely in patients on a higher dose or who are over the age of 65. Only 0.9% of newly diagnosed CML patients and 1–2% of other CML patients had severe fluid retention.34 Hepatotoxicity can occur and occasionally can be severe (< 4% of patients). Liver function tests should be done before starting treatment and then monthly, as clinically indicated. In patients in the accelerated or blast phases of CML, neutropenia or thrombocytopenia can commonly occur. Complete blood counts should be monitored weekly for the first month, then every second week for the second month, and every two to three months thereafter.34 Trastuzumab The epidermal growth factor receptor, HER2, is overexpressed in 15–25% of breast cancers. Trastuzumab is a monoclonal antibody that binds specifically to the HER2 receptor and is indicated for the treatment of metastatic breast cancer patients whose tumours significantly overexpress the HER2 protein.36 As a single agent, objective response rates of 15% have been seen in extensively pre-treated metastatic breast cancer patients who are positive for HER2 overexpression.19 In untreated metastatic breast cancer patients, objective response rates of up to 26% have been seen. When trastuzumab is added to chemotherapy, objective response rates climb to 50%, compared to 32%, when chemotherapy is given alone.19 Recently, trastuzumab has demonstrated significant reduction in the risk of disease progression when given as adjuvant therapy for early breast cancer. When the treatment is labelled adjuvant, the goal is cure.37 Three groundbreaking trials, HERA, NSABP B-31 and NCCTG-N9831, assessed trastuzumab in the adjuvant setting. In the HERA trial, after Pharmacy Practice | September 2006 09-CE-SEPT06 8/22/06 12:52 PM Page 5 ce continuing education lesson their initial chemotherapy treatment, 3,387 women were randomized to receive either trastuzumab every three weeks for one year or just observation.17 All the women overexpressed the HER2 protein or had amplification of the HER2 gene. Disease-free survival was the primary end point. With a median followup of one year post-trastuzumab or post-observation, disease-free survival was less in the women who had received trastuzumab (127 disease-free survival events compared to 220 in the observation group). This represents an unadjusted hazard ratio of 0.54 (95% confidence interval [CI] 0.43–0.61, p < 0.001). Of note, more cardiac dysfunction was seen in the trastuzumab group.17 Similar results were replicated in the NSABP B31 and NCCTG-N9831 trials. The results of these two trials were pooled in a joint analysis approved by the FDA. The combination trial had 3,351 HER2 positive women receiving their initial chemotherapy, who were then randomized to either one year of trastuzumab given on a weekly basis or to observation only.38 The primary end point was again disease-free survival. At the first planned interim analysis, the study was terminated early due to a significant difference in disease-free survival between the two groups. The median followup was two years. There were only 133 events (recurrent, second primary cancer or death before recurrence) in the trastuzumab arm compared to 261 events in the observation group. The hazard ratio was 0.48 (95% CI 0.39–0.55, p < 0.0001). At three years, 87.1% of patients were alive in the trastuzumab group versus 75.4% in the control group. This was an absolute difference of 11.7%, which is highly significant. Of note, grades III and IV (patients experiencing symptoms of congestive heart failure [CHF] with less than ordinary activity or at rest) New York Heart Association CHF, or death was higher in the trastuzumab group (4.1% compared to 0.8% in the control group in the B31 trial and in the N9831 trial; 2.9% in the trastuzumab group and 0% in the N9831 group).39,40 These three trials have revolutionized the treatment of early breast cancer for HER2 positive women. Dosing Trastuzumab is given intravenously (IV), either weekly as a loading dose of 4 mg/kg over 90 minutes followed by a maintenance dosing of 2 mg/kg over 30 minutes, or every three weeks as a loading dose of 8 mg/kg over 90 minutes, followed by maintenance dosing of 6 mg/kg also over 90 minutes. Trastuzumab should not be given concurrently with an anthracycline Pharmacy Practice | September 2006 Targeted drugs for cancer treatment (e.g., doxorubicin or epirubicin) due to increased risk of cardiotoxicity.36 Adverse effects Generally, trastuzumab is very well-tolerated. The most significant side effect is infusionrelated reactions, which occur in 40% of patients.19 Most reactions are mild to moderate in severity and are associated with fever and chills. In some centres, patients are premedicated with acetaminophen to prevent these reactions, although this is not generally recommended by the manufacturer. Usually, the reactions will occur during the first infusion or up to six hours afterwards and respond to acetaminophen or diphenhydramine; occasionally meperidine is required.36 Less than three per cent of patients have further problems with future infusions.19 The other potentially significant side effect is symptomatic or asymptomatic cardiac dysfunction, the cause of which is unclear. It has been suggested that there is uptake of trastuzumab in the myocardium and it may cross-react with an antigen in the myocardium.39,41,42 It is known that myocardial cells express the HER2 antigen. Significant cardiotoxicity is seen when trastuzumab is given concurrently with an anthracycline (e.g., doxorubicin or epirubicin). Quantified lowering of ejection fraction of at least 10% was seen in 27% of patients who had received trastuzumab and chemotherapy (doxorubicin and cyclophosphamide) versus eight per cent who received chemotherapy alone. On its own, trastuzumab has an incidence of cardiac dysfunction of 4.7%.19 Careful monitoring of left ventricular function should be done prior to, and during treatment. If there is clinically significant cardiac failure, trastuzumab should be stopped and medication should be initiated to treat the cardiac failure. Signs and symptoms to monitor include dyspnea, increased cough, peripheral edema and nocturnal dyspnea.37 Patients who experienced cardiotoxicity while on trastuzumab will generally regain cardiac function once the trastuzumab is stopped. Improvement is usually seen within a few months.39,41 Rituximab Lymphoma is a malignancy that originates in the lymphoid tissue. Of all types of lymphomas, 90% are B-cell in origin. Both malignant and nonmalignant B-cells have a CD20 antigen found on their cell surface.20 Rituximab is a monoclonal antibody that specifically binds to this CD20 receptor. Indolent lymphomas, which express CD20, have a median survival of approximately 10 years, and response to initial therapy is excellent (80–90%). Unfortunately, this response is usually not maintained. Initially, patients can be followed through watchful waiting or they can be treated with chemotherapy. For patients who relapse after initial therapy, there is no standard treatment. Rituximab, given as 375 mg/m2 IV weekly for four weeks, provided a median time-to-progression of 13 months, which is comparable to chemotherapy with significantly fewer side effects.20 In Canada, rituximab is officially indicated for relapsed or refractory low grade or follicular CD20 positive B-cell non-Hodgkin’s lymphoma (NHL). For more aggressive forms of NHL, rituximab has been studied as initial treatment. In patients who are > 60 years old, the addition of rituximab to chemotherapy increased the event-free survival at five years from 28%, in patients who only received chemotherapy, to 47.5%, in those who received both chemotherapy and rituximab. Benefit was seen in younger populations, as well.43 For this reason, rituximab is also indicated for CD20 positive diffuse large B-cell NHL in combination with cyclophosphamide-doxorubicin-vincristineprednisone (CHOP) chemotherapy. Dosing The dosing of rituximab depends on the indication. As a single agent, the dose is 375 mg/m2 IV weekly for four weeks. If it is being given in combination with chemotherapy, it is 375 mg/m2 IV with chemotherapy every three weeks. This combination is given for six to eight cycles. Adverse effects Rituximab is generally well-tolerated. Infusionrelated reactions are usually mild to moderate in severity, but approximately 10% of patients will experience severe reactions. Mild to moderate reactions are typically seen within one to two hours after starting the rituximab infusion and are brief in duration. Patients may experience fever, chills and rigors. The incidence of reactions decreases with subsequent infusions. Severe infusion-related reactions involve fever, chills and rigors, but also bronchospasm, hypotension, angioedema and hypoxia. The infusion should be stopped immediately and corticosteroids, diphenhydramine, acetaminophen, IV fluids, oxygen and/or bronchodilators should be added. Fatalities are rare and are reported in 0.04–0.07% of patients. Close monitoring during the infusion is critical, as well as premedicating with acetaminophen and diphenhydramine. In most situations, Answer online at www.pharmacygateway.ca 5 09-CE-SEPT06 8/22/06 12:52 PM Page 6 ce continuing education lesson rituximab can be resumed using a slower infusion rate (50%) when symptoms have completely resolved.20,44 Pulmonary events such as hypoxia, pulmonary infiltrates and acute respiratory failure have occurred and are usually preceded by severe bronchospasm and dyspnea. Patients at risk are those with pulmonary insufficiency or with pulmonary tumour infiltration, and rituximab should be used with caution in these patients. Transient hypotension may occur with rituximab infusion, and withholding antihypertensive medications 12 hours prior to, and throughout the rituximab infusion, should be considered.44 Other serious side effects include tumour lysis syndrome, where significant cell death can result in hyperuricemia leading to acute renal failure and, in rare cases, death. Those at most risk of tumour lysis syndrome are persons with high tumour burden.44 Bevacizumab Bevacizumab is the first anti-angiogenesis inhibitor marketed in Canada. It is a recombinant humanized monoclonal antibody that specifically binds to vascular endothelial growth factor (VEGF). In a multicentre trial, 813 patients with metastatic colorectal cancer were randomized to receive either irinotecan-fluorouracil-leucovorin (IFL) chemotherapy or IFL with bevacizumab. This was first-line therapy for these patients. The usual first-line therapy in this population is a combination of irinotecan, fluorouracil and leucovorin. The primary end point was duration of overall survival. Response rates were 34.8% in the IFL group compared to 44.8% in the IFL/bevacizumab patients (p = 0.004). Median progression-free survival increased from 6.2 months to 10.6 months (hazard ratio for progression 0.54, p < 0.001).45 Impressively, the overall median survival increased from 15.4 months to 20.3 months (hazard ratio for death 0.55, p < 0.001). Results such as these have not previously been seen in the metastatic colorectal setting.45 Bevacizumab is indicated for the first-line treatment of patients with metastatic colon and rectal cancer in combination with fluoropyrimidine-based (e.g. fluorouracil) chemotherapy.46 Dosing The dose is 5 mg/kg IV every two weeks in combination with chemotherapy. Pre-medication is not specifically recommended before the infusion.47 It is contraindicated in patients with untreated brain metastases due to its 6 Answer online at www.pharmacygateway.ca Targeted drugs for cancer treatment potential for developing a central nervous system (CNS) hemorrhage. There are no known drug interactions with bevacizumab.47 Adverse effects Twenty-two to 32% of patients will develop hypertension and 11–16% of patients will have grades III–IV hypertension. Most will have grade III hypertension, which is defined as an increase in blood pressure that will require the initiation of oral antihypertensive therapy.48 Angiotensin converting enzyme (ACE) inhibitors or calcium channel blockers are effective. Only 0.7% of patients develop grade IV hypertension where bevacizumab needs to be discontinued. Onset can occur at any time. It is believed the elevation in blood pressure is due to VEGF inhibition. When VEGF is inhibited, less nitric oxide is produced. Nitric oxide is a vasodilator and when inhibited by anti-VEGF agents (e.g., bevacizumab), would result in vasoconstriction and elevations in blood pressure. Hypertension will resolve in most patients when bevacizumab is discontinued.48 Arterial thrombosis is rare (3.8% in bevacizumab vs. 1.7% in placebo group). It can manifest as a stroke, transient ischemic attack, subarachnoid hemorrhage, myocardial infarction and angina. Patients at increased risk for arterial thrombosis from bevacizumab therapy are those who have a prior history of an arterial thromboembolic event and are older than 65. Wound healing complications can also occur. Angiogenesis is critical in this normally occurring process. In trials, the risk of wound complications increased from 0 to 10% in the bevacizumab group.48 The manufacturer recommends that bevacizumab should not be initiated in any patient until at least 28 days post-surgery to prevent wound dehiscence.46 Bleeding is also a possible side effect. Most hemorrhagic complications have been minor nosebleeds and occur in 20–40% of patients. Duration is usually less than five minutes and resolves without medical treatment.48 Concomitant use of low-dose aspirin TABLE 1 does not appear to increase bleeding risk, nor does the use of warfarin in patients who have developed a thrombosis. The risk of bleeding with known CNS metastases has not been studied and bevacizumab is contraindicated in this patient population. A small risk of gastrointestinal perforation also exists; 1.6% of 1,367 patients in the metastatic colorectal cancer trials developed gastrointestinal perforations. More than half of these patients had some risk factor including acute diverticulitis, tumour at the site of perforation, obstruction, abdominal carcinomatosis or radiation in the area. Patients should be warned to report any signs of abdominal pain associated with constipation or vomiting.48 Cost considerations Targeted therapies provide a novel approach in the fight against cancer. They have increased overall survival and time-to-disease progression in many different tumour types. In some situations, these targeted agents are the only available treatment option. Their additional benefit is that they have fewer side effects and are better tolerated by patients. Certain patients are not candidates for traditional therapy, but would be able to tolerate these targeted therapies. As these are relatively newly marketed therapies, the cost of these agents is substantial (Table 1). However, it is important to place their cost into perspective. There is the cost of managing the side effects of conventional therapies, which includes hospital admissions, and short- and long-term toxicities. As an example, docetaxel is second-line therapy in non-small cell lung cancer and costs approximately $1,690 to $1,950 for three weeks of treatment. The side effects are significant including myelosuppression (which may require hospital admission), neuropathies, hair loss and mucositis. Erlotinib, which can also be used as second-line therapy, is approximately $2,464 per month (not including pharmacy fees). The main side effects of erlotinib are rash and mild diarrhea. Approximate cost of the targeted agents49 Targeted agent Cost (treating a 70 kg patient for one month-acquisition drug) erlotinib $ 2,464 imatinib $ 4,442 (600 mg po daily x 30 days) trastuzumab $ 3,433 (price normalized to 28 days) rituximab $ 2,887 (for 1 infusion that would be given every 3 weeks along with chemotherapy) bevacizumab $ 2,757 (2 infusions, as dosing is q2weeks) Pharmacy Practice | September 2006 09-CE-SEPT06 8/22/06 12:52 PM Page 7 ce continuing education lesson With the rising cost of pharmaceutical agents in the healthcare system, difficult decisions need to be made by hospital pharmacy and therapeutic committees, as well as governments. Traditional therapies and these newer targeted agents need to be compared for both their efficacy and toxicity. Although there is a scattering of pharmacoeconomic studies done for some of these agents, more of these studies will be necessary to make informed decisions in this very difficult and emotionally charged setting.50-52 Targeted drugs for cancer treatment References 1. Canadian Cancer Society/National Cancer Institute of Canada. Canadian Cancer Statistics 2006. Toronto, Canada, 2006. 2. Green MR. Targeting targeted therapy. N Engl J Med 2005;350:2191-2. 3. Belvedere O, Grossi F. Lung cancer highlights from ASCO 2005. The Oncologist 2006;11:39-50. 4. Pao W, Miller VA. Epidermal growth factor receptor mutations, small-molecular kinase inhibitors, and non-small-cell lung cancer: current knowledge and future directions. J Clin Oncol 2005;23:2556-68. 5. Krause DS, Van Etten RA. Tyrosine kinases as targets for cancer therapy. N Engl J Med 2005;353:172-87. 6. Sridhar SS, Seymour L, Shepherd FA. Inhibitors of epi- Future directions Currently, many new targeted agents are being developed and evaluated in clinical trials. The hypothesis is that a single pathway is unlikely to be solely responsible for the uncontrolled cell division that occurs in cancer cells. By targeting multiple pathways within the cell, a higher likelihood of response might be possible. Trials combining targeted agents with different mechanisms of action are being conducted.17 Newer agents that inhibit more than one receptor, such as sunitinib, are being developed. This drug inhibits KIT, PDGFRA and VEGF and fms-related tyrosine kinase 3. Sunitinib has been studied in metastatic renal cell carcinoma and in GIST after failure with imatinib.17,33 The potential in this field is unlimited and exciting. dermal-growth-factor receptors: a review of clinical research with a focus on non-small-cell lung cancer. Lancet Oncol 2003;4: 397-406. 7. Hamid O. Emerging treatments in oncology: focus on tyrosine kinase (erbB) receptor inhibitors. J Am Pharm Assoc 2004;52-8. 8. Perez-Soler R, Chachoua A, Hammond LA, et al. Determinants of tumor response and survival with erlotinib in patients with non-small-cell lung cancer. J Clin Oncol 2004;22: 3238-47. As treatment regimens become more complex, our patients will require counselling on the nontraditional side effects of these novel agents. Some side effects are rare, but potentially life threatening. Patients will need to know what to do in the event that they do arise. Traditional chemotherapeutic agents generally do not have many drug interactions, but these newer agents do. Prescribers may not always be aware of these interactions and may not have access to the patient’s complete list of medications. The pharmacist will play a key role intercepting these potential interactions. The cure for cancer is complex and ever evolving. We have reached somewhat of a plateau with our conventional therapies and newer options are needed. Targeted therapies offer us a completely novel approach to cancer treatment, with the benefits of fewer side effects. The challenge will be to determine how our healthcare system will be able to incorporate these new therapies into patient care. Pharmacy Practice | September 2006 28. Shepherd FA, Pereira JR, Ciuleanu T, et al. Erlotinib in previously treated non-small-cell lung cancer. N Engl J Med 2005;353:123-32. 29. Hoffmann-La Roche Ltd. Tarceva product monograph. Mississauga, Ont. June 28, 2005. 30. Robert C, Soria J-C, Spatz A, et al. Cutaneous sideeffects of kinase inhibitors and blocking antibodies. Lancet Oncol 2005;6:491-500. 31. Perez-Soler R, Saltz L. Cutaneous adverse effects with HER1/EGFR-targeted agents: is there a silver lining? J Clin Oncol 2005;23:5235-46. 32. Cortes J, Kantarjian H. New targeted approaches in chronic myeloid leukemia. J Clin Oncol 2005;23:6316-24. 33. Van der Zwan SM, De Matteo RP. Gastrointestinal stromal tumour: 5 years later. Cancer 2005;104:1781-8. 34. Novartis. Gleevec product monograph. April 27, 2005. New monograph for February 27, 2006. 35. Gambillara E, Laffitte E, Widmer N, et al. Severe pustular eruption associated with imatinib and voriconazole in a patient with chronic myeloid leukemia. Dermatology 2005;211: 363-5. 36. Hoffmann-La Roche Ltd. Herceptin product monograph. Mississauga, Ont.;July 20, 2005. 9. Giaccone G. Epidermal growth factor receptor inhibitors 37. Devita VT, Rosenberg SA, eds. Cancer: principles and practice of oncology. Baltimore, MD: Lippincott, Williams & 2005;23:3235-42. Wilkins; 2005. 10. Segaert S, Van Cutsem E. Clinical signs, pathophysiology 38. Romond EH, Perez EA, Bryant J, et al. Trastuzumab and management of skin toxicity during therapy with epidermal plus adjuvant chemotherapy for operable HER2-positive breast growth factor receptor inhibitors. Ann Oncol 2005;16:1425-33. cancer. N Engl J Med 2005;353:1673-84. 11. O’Brien SG, Guilhot F, Larson RA, et al. Imatinib com- 39. Tan-Chiu E, Yothers, G, Romond E, et al. Assessment of pared with interferon and low-dose cytarabine for newly diag- cardiac dysfunction in a randomized trial comparing doxorubicin nosed chronic-phase chronic myeloid leukemia. N Engl J Med and cyclophosphamide as adjuvant therapy in node-positive, 2003;348:994-1004. human epidermal growth factor receptor 2-overexpressing 12. Lyseng-Williamson K, Jarvis B. Imatinib. Drugs 2001;61: 1765-74. 13. AHFS First Fax. New drug overview, imatinib. Am J 14. Harris M. Monoclonal antibodies as therapeutic agents for cancer. Lancet Oncol 2004;5:292-302. 15. Leyland-Jones B. Trastuzumab: hopes and realities. Lancet Oncol 2002;3:137-44. 16. Hennessy BT, O Hanrahan EO, Daly PA. Non-Hodgkin lymphoma: an update. Lancet Oncol 2004;5:341-53. 17. Piccart-Gebhart MJ, Procter M, Leyland-Jones B, et al. Trastuzumab after adjuvant chemotherapy in HER2-positive breast cancer. N Engl J Med 2005;353:1659-72. 18. Burnstein MJ. The distinctive nature of HER2-positive breast cancers. N Engl J Med 2005;353:1652-4. breast cancer: NSABP B-31. J Clin Oncol 2005;23:7811-9. 40. Arnold JMO, Liu P, Demers C, et al. Canadian Cardiovascular Society consensus conference recommendations on heart failure 2006: diagnosis and management. Can J Cardiol 2006;22:23-45. 41. Ewer MS, Vooletich MT, Durand JB, et al. Reversibility of trastuzumab-related cardiotoxicity: new insights based on clinical course and response to medical treatment. J Clin Oncol 2005;23:7820-6. 42. Levine MN. Trastuzumab cardiac side effects: only time will tell. J Clin Oncol 2005;31:7775-6. 43. Coiffier B. State-of-the-art therapeutics: diffuse large Bcell lymphoma. J Clin Oncol 2005;23:6387-93. 44. Genentech Inc. Rituxan product monograph. South San Francisco, CA; March 9, 2006. 19. McKeage K, Perry CM. Trastuzumab: a review of its use 45. Hurwitz H, Fehrenbacher L, Novotny W, et al. in the treatment of metastatic breast cancer overexpressing Bevacizumab plus irinotecan, fluorouracil, and leucovorin for HER2. Drugs 2002;62:209-43. metastatic colorectal cancer. N Engl J Med 2004;350:2335-42. 20. Plosker GL, Figgitt DP. Rituximab: a review of its use in non-Hodgkin’s lymphoma and chronic lymphocytic leukaemia. Drugs 2003;63:803-43. 21. Marshall J. The role of bevacizumab as first-line therapy for colon cancer. Semin Oncol 2005;32 Suppl 9:S43-S47. 22. Zakarija A, Soff G. Update on angiogenesis inhibitors. Conclusion 2005;65:7525-9. in the treatment of non-small-cell lung cancer. J Clin Oncol Health-Syst Pharm 2001;58:2241-2. The pharmacist’s role 27. Johnson BE, Janne PA. Epidermal growth factor receptor mutations in patients with non-small cell cancer. Cancer Res Curr Opin Oncol 2005;17:578-83. 23. Zondor SD, Medina PJ. Bevacizumab: an angiogenesis inhibitor with efficacy in colorectal and other malignancies. Ann Pharmacother 2004;38:1258-64. 46. Hoffmann-La Roche Ltd. Avastin product monograph. Mississauga, Ont.; April 12, 2006. 47. Motl S. Bevacizumab in combination chemotherapy for colorectal and other cancers. Am J Health-Syst Pharm 2005;62:1021-32. 48. Gordon MS, Cunningham D. Managing patients treated with bevacizumab combination therapy. Oncology 2005;69 Suppl 3:25-33. 49. http://www.cancercare.on.ca/index_chemoRegimensby Disease.htm (accessed February 27, 2006). 24. Ignoffo RJ. Overview of bevacizumab: a new cancer 50. Neyt M, Albrecht J, Cocquyt V. An economic evaluation therapeutic strategy targeting vascular endothelial growth factor. of Herceptin in adjuvant setting: the Breast Cancer International Am J Health-Syst Pharm 2004;61 Suppl 5:S21-S26. Research Group 006 trial. Ann Oncol 2006;17:381-90. 25. Bergsland EK. Vascular endothelial growth factor as a 51. Norum J, Risberg T, Olsen JA. A monoclonal antibody therapeutic target in cancer. Am J Health-Syst Pharm 2004; 61 against HER-2 (trastuzumab) for metastatic breast cancer: a Suppl 5:S4-S11. model-based cost-effectiveness analysis. Ann Oncol 2005;16: 26. Janne PA, Engelman JA, Johnson BE. Epidermal growth 909-14. factor receptor mutations in non-small-cell lung cancer: implica- 52. Uyl-de Grott CA, Giaccone G. Health economics: can tions for treatment and tumor biology. J Clin Oncol 2005;23: we afford an unrestricted use of new biological agents in gas- 3227-34. trointestinal oncology? Curr Opin Oncol 2005;17:392-6. Answer online at www.pharmacygateway.ca 7 09-CE-SEPT06 8/22/06 12:52 PM Page 8 ce continuing education lesson Targeted drugs for cancer treatment Questions 1 Which one of the following statements is true about targeted therapy? a) Preferably the target functions exactly the same in tumour and healthy tissue. b) The target has been validated as a negative prognostic factor. c) Generally they are less expensive treatment options than other therapies. d) Hair loss is a common side effect. 2 Which of the following is true regarding tyrosine kinases? a) They are usually found on the extracellular surface of cells. b) The BCR-ABL tyrosine kinase is usually in its inactive form. c) EGFR overexpression is common in non-small cell lung cancer. d) The EGFR and BCR-ABL tyrosine kinase are the same tyrosine kinase. 3 Antibody-derived therapy is best described by: a) It requires the use of a specific antibody for a selected target. b) Rituximab and trastuzumab have the potential to cause infusion-related reactions. c) It has specificity for intracellular targets. d) a and b are correct e) a, b and c are correct 4 Which of the following statements are false regarding angiogenesis? a) It is stimulated by VEGF. b) It typically produces irregular and convoluted vessels in tumour tissue. c) It is a process that is usually very active in adults on a daily basis. d) It is necessary for tumours to grow greater than two millimetres. CASE A CM is a 68-year-old women with non-small cell lung cancer and a nonsmoker. 5 Which one of the following statements about erlotinib is true? a) She will likely receive it as first-line therapy. b) Drowsiness is its main side effect. c) Her likelihood of a response is lower because she is a woman and a nonsmoker. d) Survival benefit has been demonstrated when it was compared to placebo. 6 It will be important to counsel CM on her new erlotinib prescription. Which of the following is a side effect common to erlotinib? a) There is a significant risk of nosebleeds. b) It is preferable to take the dose with food. c) There is a potential for rash. d) Significant hair loss is likely. 7 CM also has a prescription for the following medications. Which one would not be a problem, if taken concurrently with erlotinib? 8 Answer online at www.pharmacygateway.ca a) b) c) d) St. John’s wort trimethoprim/sulfamethoxazole itraconazole warfarin 8 Eight days after starting her erlotinib, CM notices an acne-like, nonpruritic rash on her forehead and chin. What is the best management option? a) Stop therapy immediately. b) Apply some benzoyl peroxide acne gel to the lesions. c) Use doxycycline 200 mg po daily x 6 weeks. d) No treatment—rash may improve on its own. 9 Three weeks after starting therapy, CM notices that her rash is now found on more than 50% of her body, and is itchy. Which approach to treatment is inappropriate? a) doxycycline 200 mg po daily b) topical steroids to cover all of the rash c) diphenhydramine prn d) interruption in therapy should be considered 10 Rash with erlotinib is often a predictor of positive response. a) true b) false 11 Regarding the diarrhea that can develop while a patient is on erlotinib, which answer is the most correct? a) Loperamide is rarely potent enough to treat this type of diarrhea. b) Dose reductions can be attempted if the diarrhea is significant. c) Erlotinib must be abandoned. d) Diarrhea is correlated with response to erlotinib. CASE B BN is a 56-year-old male with a diagnosis of chronic phase CML who will be starting therapy with imatinib. 12 Which of the following is true? a) He can continue to take the St. John’s wort that he has been using for mild depression. b) He should take imatinib on an empty stomach. c) The risk of developing thrombocytopenia in his case is very high. d) Liver function tests should be done before starting therapy. 13 After a few weeks of treatment, BN notices his ankles and lower legs are swollen, but not red or warm. What is the best treatment approach? a) Lowering his dose would be helpful. b) He was at a high risk of developing peripheral edema due to his age. c) Symptomatic relief may be obtained with a diuretic. d) a and c are correct e) a, b and c are correct 14 BN has returned from a trip to Australia and developed a deep vein thrombosis during the flight. Warfarin treatment will be easily managed while on imatinib. a) true b) false 15 When speaking to a patient before her first trastuzumab infusion, which risk is it important she be aware of? a) Hair loss may occur. b) Cardiac dysfunction occurs in > 50% of patients. c) She might develop a fever and chills that are easily treated with acetaminophen and diphenhydramine. d) The risk of developing an infusion-related reaction is just as likely with the second infusion. 16 Which of the following is false regarding cardiotoxicity with trastuzumab? a) It is irreversible in most cases. b) It is exacerbated when trastuzumab is given concurrently with a chemotherapy in the anthracycline family (e.g., doxorubicin). c) Nocturnal dyspnea and peripheral edema are potential symptoms of cardiac dysfunction. d) It can be managed with medications used to treat congestive heart failure. 17 Which is true regarding infusion-related reactions with rituximab? a) Severe infusion-related reactions are common. b) The risk is higher on the second infusion. c) Fatalities are common. d) Premedication with acetaminophen and diphenhydramine are essential. 18 Angiogenesis is only stimulated by VEGF. a) true b) false 19 Which of the following statements is true regarding bevacizumab? a) It can cause significant nausea. b) Nosebleeds are common and can be treated conservatively. c) Hair loss is common. d) > 50% of patients develop sore ulcerated mouths. 20 When counselling a patient on bevacizumab, it is important to mention all of the following except : a) Blood pressure monitoring is important. b) Any signs of abdominal pain with constipation or vomiting should be reported to a physician. c) Regular heart scans are required during therapy. d) It is important to let the oncologist know if there are any surgical procedures pending. Pharmacy Practice | September 2006