Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
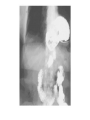
Disease of Esophagus 浙江大学附属第一医院胸外科 张翀 Disease of Esophagus 1, Gastroesophageal Reflux 2, Neoplasms ---Esophageal Cancer 3, Neuromuscular Disorders 4, Trauma Esophagus- Anatomy Location End Distance from Incisors Cervical Esophagus Below the cricopharyngeus muscle (C6) Thoracic inlet 15~20cm Upper Thoracic Thoracic inlet Inferior azygus arch 20~25cm Middle Thoracic Inferior azygus arch Inferior Pulmonary Vein 25~30cm cardia of the stomach at T11. >30cm Beginning Parts of Eso Lower Thoracic and Abdominal Inferior Pulmonary Vein Esophageal Anatomy The esophagus is a two-layered mucosa-lined muscular tube that journeys through the neck, chest, and abdomen and rests unobtrusively in the posterior mediastinum. It commences at the base of the pharynx at C6 and terminates in the abdomen, where it joins the cardia of the stomach at T11. Esophagus- Anatomy (Narrowings) Narrowing Location Clinical Diameter Superiormost Narrowing the anatomic border of the pharynx and proximal esophagus This narrowest point of the esophagus , it is the most common site of iatrogenic perforation. (M: 15cm, F: 14cm) 1.5 cm Second Narrowing crossing of the left mainstem bronchus and the aortic arch Indentation of the anterior and left lateral esophageal wall. (M: 25cm, F:23cm ) 1.6 cm Most inferior Narrowing the diaphragmatic hiatus (caused by LES) great variation of the luminal diameter (M: 30cm, F:28cm ) 1.6 to 2.5 cm Esophageal Anatomy Narrowings Esophageal Carcinoma- Anatomy (Cervical) The triangular areas of the sparse muscle cover are shown in the scheme. Zenker’s diverticulum arises from Killian’s triangle. The surgical approach to the cervical esophagus may be from either side of the neck through an incision along the medial border of the sternocleidomastoid muscle. The left-sided approach is preferred to avoid injury to the right recurrent nerve. Muscular architecture of the pharyngoesophageal junction, which is the region of the upper esophageal sphincter. Esophagus- Anatomy (Thoracic) a. The thoracic portion of the esophagus is approximately 20 cm long . b. It starts at the thoracic inlet, in the upper portion of the thorax, it is closely related to the posterior wall of the trachea. This close relationship is responsible for the early spread of cancer of the upper esophagus into the trachea.(a big limitaion!) c. The lower thoracic esophagus is buttressed only by mediastinal pleura on the left, making this portion the weakest and the most common the site of perforation in Boerhaave’s syndrome. Esophagus- Anatomy (Abdominal) a. The abdominal portion of the esophagus is approximately 2 cm long and includes a part of the LES. Squamous epithelium Columnar epithelium The distal 1 to 2 cm of esophageal mucosa transitions to cardiac mucosa or junctional columnar epithelium at a point known as the Z-line . Chapter 1 Esophageal Cancer Esophageal Cancer - Epidemiology Esophageal cancer is the fastest growing cancer in the United States. 6th most common malignancy with an incidence of 20 per 100,000 and represents 4% of newly diagnosed cancers in North America. South Africa and China: 160 / 100,000 Kazakhstan: 540 / 100,000. Iran : 165.5/100,000 (M), 195.3/100,000(F) Linxian China: 478.87/100,000 Esophageal Cancer-Etiology Carcinogens Tobacco Alcohol Nitrosamines Fungal toxins Spices Nutritional deficiencies Vitamins A, C, riboflavin Physical factors Thermal trauma Hot food or drinks Abrasive material (soil) and food Predisposing factors Tylosis (胼胝症) Plummer-Vinson syndrome Achalasia Celiac sprue (乳糜泻) Esophageal Cancer-Pathology Esophageal carcinoma is originated from the epithelium between pharynx and junctional area of esophagus and stomach. Mostly occurred in the MIDDLE segment (52.7%). Early stage: circumscribed within mucosal or sub-mucosal layer : ①occult type ②erosive ③plague ④papillary Advanced stage: invading muscular or adventitial layer ① medullary(60%) ② fungoid(15%) ③ ulcerative(10%) ④ constrictive(10%) ⑤ intra-cavity(5%) A. William Blackstcok , et al. Esophageal Cancer principle and Practice, 2009 Medullary Fungoid Ulcerative Constrictive Common symptoms of esophgeal cancer presentation Symptom onset is late Progressive dysphagia is most common. Initially with meat, then soft foods and liquids. Pain develops late. (Substernal, epigastric, or back areas). Increases with swallowing, may radiate. Weight loss Regurgitation of blood-flecked esophageal contents Anorexia (poor appetite) Fatigue If tumor is in upper third of esophagus( Sore throat, Choking, Hoarseness) Metastasis In the advanced pathologic stages of the disease, direct extension through the wall of the esophagus is common, as are lymphatic metastases. Lymphatic metastases were found in about 60% of patients undergoing esophagectomy. 1. Intraesophageal Spread: a. proximal resection margin: Submucosal lymphatic spread occurs often and may result in tumor emboli producing satellite nodules 2. Direct Extension a. tumor may invade adjacent structures, including the pleura, trachea, left mainstem bronchus, pericardium, great vessels, thoracic duct, and the anterior ligaments of the vertebral column. b. Upper esophagus: the recurrent laryngeal nerves , Lowe esophagus: diaphragm, stomach, and liver. 3. Lymphatic Spread: a. upper third of the esophagus drains primarily to the upper mediastinum and neck b. lower esophagus flows to the abdomen. 4. Distant Metastatic Disease: a. Visceral metastases may be present in up to 30% of patients at the time of diagnosis and are manifestations of advanced disease. b. Metastases were found in the lungs, liver, pleura, bone, kidneys, and adrenal glands. Esophageal Cancer – Diagnostic Workup Endoscopy with biopsy: Necessary for definitive diagnosis, the location of the lesion, degree of obstruction, and longitudinal as well as circumferential extent of the lesion can be determined. Endoscopic ultrasonography (EUS): Important tool to staging, is important in the evaluation of possible tracheal or bronchial invasion by a carcinoma in the cervical and the upper or middle thirds of the thoracic esophagus. Barium swallow with fluoroscopy: is the MOST commonly used contrast agent for fluoroscopic examination of the esophagus and the gastrointestinal tract. It permits a safe, expedient study of the esophageal mucosa, luminal distensibility, motility, and any anatomic pathology. Bronchoscopic examination: Detect involvement of lung Computed tomography (chest + upper abdominal CT): is used to determine the local extent of the tumor, the relationship to adjacent structures, and distant metastases. Magnetic resonance imaging (MRI): The capability of MRI to demonstrate a tumor in the coronal and sagittal planes is superior in the estimation of the tumor length, but this information has only limited clinical value. Esophageal Cancer - Treatment Endoscopic mucosal resection (EMR) Types of Esophageal Resection: (maybe Open or minimally invasive) -Sweet Esophagectomy (Left Thoracic or Left Thoracoabdominal Esophagectomy) -Ivor Lewis Esophagectomy Laparotomy and preparation of gastric or colon conduit + Right thoracotomy for esophageal mobilization and resection with mediastinal lymph node dissection) -Mcown Esophagectomy (Ivor Lewis Esophagectomy + Neck ) -Transhiatal Esophagectomy (THE) Dr. Frank Torek. Credited with the first transthoracic esophageal resection, performed in 1913. Dr. Richard Sweet. Developed the basis for the modern approach to transthoracic esophagectomies with Dr. Churchill at the Massachusetts General Hospital in the 1940s and 1950s. Ivor Lewis. A British surgeon who performed the two-stage esophagectomy via an abdominal approach and subsequent right thoracotomy that bears his name today. Abdominal exposure in an Ivor Lewis esophagectomy. A pyloric drainage procedure is now performed. Choices include pyloromyotomy, pyloroplasty, and more recently botox injection. Some perform no drainage procedure. Pyloromyotomy was the author’s preferred procedure, but recent experience with botox injection has been satisfactory. Two hundred units of botox is mixed in 5 mL of normal saline and approximately 1.25mL is injected into the pyloricmuscle at the one o’clock, 3 o’clock, 6 o’clock, and 9 o’clock positions. To aid in the resection of the proximal stomach when drawn into the right chest, the gastrohepatic tissue at the point of resection of the distal lesser curvature is cleared. This point is about six vascular arcades distal to the esophagogastric junction. The celiac axis is marked with a long stitch to aid pathologic examination. A jejunostomy tube is then placed 30 to 40 cm beyond the ligament of Treitz. The abdomen is closed. The patient is placed in the left lateral decubitus position, prepped, and draped. A right posterolateral thoracotomy incision is made, and the fifth intercostal space is entered. The lung is deflated using the double lumen endobronchial tube placed at the beginning of anesthesia. The azygos vein is divided using the endo GIA 30, 2.5 stapler (Endo GI Universal, US Surgical, Norwalk, CT). The pleura is scored with the electrocautery from posterior to the azygos down to the hiatus. The inferior ligament is incised and the pleura scored back to the cut azygos vein. Boundaries of dissection are now marked. The esophagus is then dissected and encircled with a large penrose drain at the level of the arching azygos vein. Care must be taken with this maneuver to avoid entering the esophageal muscularis propria as the posterior muscle fibers are often “splayed” deep into the mediastinum. v. =vein. Using the penrose as a traction device, the esophagus and the attached lymphoareolar tissue aremobilized from the mediastinal bed. Aortic branches are clipped. The dissection includes mobilization of the subcarinal lymph node packet, which is kept intact with the specimen and marked with a double stitch. The pericardium is “bared.” The vagal nerve trunks are cut as the esophagus is mobilized from the lower superior mediastinum. Once the hiatus is reached, final attachments are released. Level 15 (diaphragmatic) lymph nodes are carefully identified and resected. The thoracic duct is purposely ligated at this level by mass ligature of all tissue between the aorta, spine, and azygos vein using a 0-silk tie. The nasogastric tube that was placed after the endoscopy is withdrawn to the thoracic inlet. The esophagus is stapled above the azygos vein using a GI stapler with a “green load” (such as PI 30 mm stapler; US Surgical). With care to preserve proper orientation, the stomach is delivered through the hiatus into the chest. The gastric conduit is formed by several applications of the ILA 100-mm stapler (US Surgical) or use of the 60-mm endostapler (Endo GIA Universal, US Surgical). The previously cleared portion of the distal lesser curvature serves as a distal marker. The highest point of the fundus is easily identified when the stomach is put on “stretch.” If the tumor is at the gastroesophageal junction, a more “V-shaped” staple line will increase the radial gastric margin. The highest point of the staple line is oversewn with a 3-0 silk horizontal mattress suture as well as where staple lines have crossed each other. Transdiaphragmatic approach through a circumferential incision. McKeown modification Perioperative complications - Esophageal Cancer 1. Anastomotic Leak The incidence of intrathoracic leak following Ivor Lewis esophagectomy is typically 5–10%. An intrathoracic leak is a life-threatening event that usually requires immediate operative intervention. 2. Anastomotic Stricture Anastomotic stricture is never life threatening, A large retrospective meta-analysis concluded that the incidence of symptomatic stricture was somewhat higher following anastomosis in the cervical position (28%) than after Ivor Lewis resection (16%). 3.Recurrent Laryngeal Nerve Injury 4. Respiratory Complications (Pneumonia, atelectasis, and respiratory failure) The incidence of pneumonia following esophagectomy ranges from 2% to 47%. Respiratory failure following esophagectomy occurs in 4% of patients. 5. Bleeding 6. Chyle Leak 7. Postresection Reflux 8. Impaired Conduit Emptying 9. Local Recurrence Chapter 2 Gastroesophageal Reflux Chapter 3 Benign tumor of Esophagus Leiomyoma Leiomyoma Duplication Polyp and Squamous Papilloma Chapter 4 Neuromuscular Disorders Diverticulum Achalasia Achalasia Achalasia Chapter 5 Trauma Caustic injury Foreign Body Peforation and Boerhaave Peforation and Boerhaave