Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
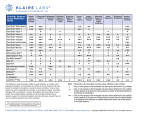
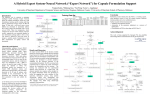
Poster number: W5279 Assessment of the safety, tolerability and pharmacokinetics of single doses of oral dexanabinol in healthy subjects, using an adaptive protocol A Connor1, P Evans1, C Doherty1, P Scholes1, C Flanagan1, S Lavin2, A Saunders2, D. Hynes2, P. McKeown2 1. Quotient Clinical Limited, Nottingham, UK; 2. E-Therapeutics plc, Oxfordshire, UK BACKGROUND Dexanabinol is a synthetic analogue of tetrahydrocannabinol (THC) in development as a potential anti-cancer therapy. Dexanabinol binds only weakly to cannabinoid receptors 1 and 2 (CB1 and CB2), reducing its psychotropic potential in comparison to other molecules in the cannabinoid class. It has been shown to impact signalling of the protein complex, nuclear factor kappalight-chain-enhancer of activated B cells (NFκB), to block the action of TNFα at the post-transcriptional level in the rat closed head injury model and reduce the secretion of prostaglandin E2 produced by the enzyme cyclooxygenase-2 (COX-2). The multivalent nature of dexanabinol’s inhibitory activity is likely to play a role in its observed tumouricidal activity, rendering dexanabinol an effective novel anti-cancer therapy [1-5]. Dexanabinol has previously been investigated in traumatic brain injury and e-Therapeutics have identified, through its Network Pharmacology platform, that there was a potential anti-tumour activity. To date, no clinical studies have been conducted via the oral route, however, dexanabinol formulated for intravenous (IV) infusion is currently undergoing clinical trials in patients in both the UK and in the US. PURPOSE The purpose of this programe was to select a liquid formulation, and administer in an adaptive first-in-human (FIH) study to assess the safety, tolerability and pharmacokinetics (PK) of dexanabinol via the oral route METHODS Translational Pharmaceutics • Translational Pharmaceutics is a platform that combines “real-time” manufacturing with immediate clinical dosing, achieved by the co-location of GMP manufacturing suites and a clinical unit [6]. • Drug product formulation development and analytical facilities are also housed at the same site. • Within the clinical program, the use of real-time manufacturing reduces the shelf life requirements to support the FIH study and therefore significantly reduces the timelines to generate the submission data package. • This platform supported an adaptive clinical protocol, enabling the determination of dose and number of cohorts in real-time, based on emerging data. +44 115 9749000 (UK) Formulation selection • A program of solubility screening was performed with a range of lipophilic solvents to identify a suitable formulation. Nine lipophilic vehicles were screened. • Miglyol 812N was identified as the most appropriate formulation for the clinical study. • A matched placebo was developed and taste masking achieved by pre-rinsing with Bitrex. • Batch release and short-term stability data (4 hrs) on the formulation strengths bracketing the planned dose range were filed. FIH Clinical study design • Healthy males, aged 18-45 participated in a doubleblind, placebo-controlled single ascending dose study. • Three cohorts were initially planned (6 active:2 placebo), with the option for a further 3 cohorts. • Two optional cohorts were invoked, resulting in single oral doses of dexanabinol administered over 5 dose levels. • Subjects were on-site from 08:00 on Day -1 until 48 h post-dose and returned to the clinic for a follow-up visit between 5 to 10 days post-dose. • Safety was evaluated through assessment of clinical laboratory tests, ECG, and vital signs. • Blood samples for dexanabinol PK were withdrawn at regular intervals and standard PK parameters were estimated. • Blood samples for future analysis of potential bloodborne PD biomarkers were also withdrawn and retained. • Dose escalation was based on safety and PK review. • GMP manufacture of the selected formulation was conducted at the clinical site immediately prior to dosing. This enabled real-time, within-study adjustments in drug product dose based on emerging safety, and PK data (Figure 1). RESULTS Formulation selection • Solubility screening, formulation selection and generation of data for the regulatory submission were completed in 6 weeks. • The selected product for dosing was drug in bottle, resuspended with Miglyol 812N. • Approval from MHRA was provided in 7 days. Subjects and safety findings • 40 subjects were enrolled • • Age (mean (SD)): 31 (8) years BMI (mean (SD)): 26.7 (3.07) kg/m2 • Dexanabinol was well tolerated. There were no serious adverse events and no clinically significant abnormalities considered related to the study drug. Pharmacokinetics • Quantifiable plasma concentrations sufficient for parameter estimation were measured at Cohort 2 and above (Table 1, Figure 2). Cohort N Tmax1 (h) Cmax (ng/mL) AUC(0-24) (ng.h/mL) 3 6 (2-6) 3.69 (62.3) NC2 6 6 (2-8) 7.99 (48.7) 106 (21.9) [n=3] 3 6 6 (2-8) 13.7 (104.3) 167 (118.2) [n=3] 4 6 6 (1-6) 26.3 (71.3) 252 (46.6) [n=5] 5 6 2 (1-6) 24.5 (67.2) 192 (68.8) 1 2 1) Median (range) 2) Not calculated Table 1: GMP manufacture Clinical dosing Data review Decision step 7 - 14 day cycle time Figure 1: Translational Pharmaceutics enabled study construct +1 800 769 3518 (USA) Geometric Mean (CV%) Values for Key PK Parameters for Dexanabinol • Dose proportional increases in Cmax and AUC with increasing dose were confirmed up to and including Cohort 4. • At Cohort 5, the PK profiles were highly variable and on average Cmax and AUC reduced in comparison with Cohort 4. • Plasma concentration values for dexanabinol were variable, indicating evidence of low solubility and absorption-limited PK. AAPS 2014 [email protected] Figure 2: Geometric Mean Plasma Concentration Time Profiles for Dexanabinol CONCLUSION A liquid formulation was selected to conduct this preliminary investigation into the PK of dexanabinol following single oral doses to healthy volunteers. Clinical assessment was performed using an adaptive FIH design. Doses were selected based on emerging safety and PK data, and formulations only manufactured ‘on demand’, thereby conserving drug substance. Oral dexanabinol was safe and well tolerated at the doses tested, and approximately dose proportional systemic exposure confirmed up to Cohort 4. Further investigations and optimisation regarding the opportunities for an oral formulation of dexanabinol are ongoing at e-Therapeutics. REFERENCES 1. Basseres DS and Baldwin AS. Nuclear factor-кB and inhibitor of кB kinase pathways in oncogenic initiation and progression. Oncogene. 2006; 25: 6817-6830. 2. Moore R, Owens D, Stamp G, et al. Mice deficient in tumor necrosis factor α are resistant to skin carcinogenesis. Nature Medicine. 1999; 5: 828–831. 3. Warzocha K, Ribeiro P, Bienvenu J, et al. Genetic polymorphisms in the tumor necrosis factor locus influence Non-Hodgkin’s lymphoma outcome. Blood. 1998; 91: 3574-3581. 4. Shohami E, Gallily R, Mechoulam R et al. Cytokine production in the brain following closed head injury: dexanabinol (HU-211) is a novel TNF-α inhibitor and an effective neuroprotectant. J Neuroimmunol. 1997; 72: 169– 177. 5. Garzon A, Avraham A, and Fink G. Dexanabinol and dexanabinol analogs regulate inflammation related genes. United States Patent Application 2005; Appl. No. 10/942,504. 6. Connor A, Scholes P, Stevens L, et al. Flexible Approaches to Incorporate Formulation Assessments and Selection into First-in-Human (FIH) Safety and Tolerability Studies. AAPS 2013, Poster R6305. www.quotientclinical.com