Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
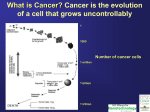
Anatomic Considerations and Patterns of Spread Rectum 12 to 15 cm in length from the rectosigmoid junction to the puborectalis ring upper third middle third (posterior border of the rectouterine pouch or rectovesical space) lowest third no serosal barrier Colonic nodal drainage consists of pericolic nodes and nodes in association with the vascular supply to the colon (i.e., mesenteric nodes rectal nodal drainage include the perirectal, presacral, and internal iliac nodes . Epidemiology, Molecular Cascade, Risk Factors, Hereditary Disease, and Clinical Presentation The median age is in the seventh decade chemical carcinogens Environmental and dietary factors Factors shown to increase the risk include increasing age, male sex, rectal cancer excessive alcohol use family history of colorectal cancer, increasing height, increasing body mass index, processed meat intake low folate consumption. consumption of fruits and vegetables ? The role of chemopreventive agents (carotenoids, aspirin, and other nonsteroidal anti-inflammatory drugs) ? Biologic and genetic pathways of development of colorectal cancer proto-oncogenes (mutations in the ras proto- oncogene.) tumor suppressor genes (inactivation adenomatous polyposis coli (APC) and P53) Biology :microsatellite “instability” The majority of HNPCCas well as a minority of sporadic colorectal cancers harbor microsatellite “instability.” mutations in genes encoding enzymes that repair DNA replication errors Studies have suggested that patients with tumors possessing a high frequency of microsatellite instability have a more favorable outcome and develop fewer metastases Colorectal cancer minimal or no symptoms Nonspecific bowel habits, weakness, intermittent abdominal pain, nausea, and vomiting. The persistence of such symptoms as well as any evidence of iron deficiency anemia should be investigated Clinical Presentation right colon exophytic ,iron deficiency anemia left colon and sigmoid colon deeply invasive, annular, and accompanied by obstruction and rectal bleeding Rectal cancer frequently results in bleeding and alterations in bowel habits. FIGURE 58.1. Idealized depiction of peritoneal relationships in the colon and rectum. The transverse and sigmoid colon are intraperitoneal, with a complete peritoneal covering (serosa) and mesentery. The ascending and descending colon are retroperitoneal, lack a true mesentery, and usually do not have a peritoneal covering posteriorly or laterally. The upper rectum begins above the peritoneal reflection and has peritoneum anteriorly and laterally. The lower half to two thirds of the rectum is below the peritoneal reflection (infraperitoneal). Prevention and Early Detection Neoplastic polyps are precursors of colon cancers Most colorectal cancers arise from pre-existing polyps Patients with neoplastic polyps should be considered at high risk for large bowel cancer, and polypectomy may reduce this risk. With the availability of the flexible colonoscope and endoscopic polypectomy, polyps can be removed at a premalignant stage and patients followed closely. The goal of screening is to detect preinvasive polyps or early invasive cancer. The presence of polyps increases the risk for cancer to approximately 15%. Data from programs in which proctoscopy is performed annually suggest that routinely scheduled polypectomy reduces the development of subsequent bowel cancer by 80% or more . The American Cancer Society has recommended screening should begin at age 50 in the average risk patient by either: Annual fecal occult blood test and/or flexible sigmoidoscopy every 5 years, Double contrast barium enema every 5 years Colonoscopy every 10 years patients at high risk adenomatous polyps history of colorectal cancer first-degree relative with colorectal cancer or adenomas inflammatory bowel disease family history or genetic testing Intensive surveillance is recommended for patients at high risk 1. Computed tomography (CT) colonography 2. genetic fecal testing are being studied Although screening methods can detect colorectal cancer at an early stage, <40% of patients are diagnosed with early disease, likely reflecting low rates of disease awareness as well as the infrequency of screening in eligible candidates Pathology (>90%) adenocarcinomas Scc, carcinoid, leiomyosarcoma, and lymphoma. Most grading systems classify adenocarcinoma as well, either moderately or poorly differentiated. Pathways of Spread invade from mucosa through the bowel wall and beyond, with involvement of lymphatic channels and lymph nodes. Hematogenous spread can occur, primarily to the lung and liver. There is little propensity for colon cancer to spread longitudinally within the bowel wall, in contrast to esophageal or gastric cancers Patient Evaluation/Staging Pretreatment evaluation 1. pathological confirmation 2. colonoscopy ( synchronous primaries occurring in 3. 4. 5. 6. 7. 8. 3% to 5%) CBC with LFT and CEA abdominal and pelvic CT scan CXR (PET) scan (MRI), Ultrasound (PET) scan در مرحله بندی قبل عمل ارزشمند نیست اما در مرحله بندی بعد درمان ،عود یا شک به عود مفید است دویتا در موارد الیگومتاستاز کاندید درمان شفاء دهند ه مفید است.پرز Prognostic factors depth of tumor invasion into and beyond the bowel wall the number of involved regional lymph nodes presence or absence of distant metastases The tumor, node, metastasis (TNM) system of the American Joint Committee on Cancer can be used as a clinical (preoperative) or postoperative staging system Colorectal Tumor, Node, Metastasis Staging, 2002 Tis Carcinoma in situ: Intraepithelial or invasion of lamina propria T1 Tumor invades submucosa T2 Tumor invades muscularis propria T3 Tumor invades through the muscularis propria into the subserosa, or into non-peritonealized pericolic or perirectal tissues T4 Tumor directly invades other organs or structuresa and/or perforates visceral peritoneum (includes invasion of other segments of colon) Direct invasion in T4 includes invasion of other segments of the colorectum by way of the serosa; for example, invasion of the sigmoid by a carcinoma of the cecum. Tumor that is adherent to other organs or structures, macroscopically, is classified as T4. However, if no tumor is present in the adhesion, microscopically, the classification should be pT3 N1 Metastasis in one to three regional lymph nodes N2 Metastasis in four or more regional lymph nodes (Tumor nodules in the pericolonic adipose tissue without evidence of residual lymph node are classified as a regional lymph node metastases) Therapy of Colon Cancer Surgery based on the anatomy and mechanisms by which this disease spreads. avoid cutting across tumor in intramural lymphatics, sufficient lengths of bowel must be resected Resection results in excellent cure rates average 5-year survival o 97% for T1N0 o 85% to 90% for T2N0 o 65% to 75% for T3–T4N0 o 50% (T3N+) and 35% (T4N+) American Joint Committee on Cancer Stage Grouping T N M Dukes MAC Stage I T1 A A T2 A B1 IIA T3 B B2 IIB T4 B B3 IIIA T1-T2 N1 M0 C C1 IIIB T3-T4 N1 M0 C C2/C3 IIIC Any T N2 M0 C C1/C2/C3 IV Any T Any N M1 - D Adjuvant Chemotherapy addition of 5FU (5-fluorouacil) and leucovorin improves survival for resected stage III patients Capecitabine, an oral 5-FU prodrug, has demonstrated similar overall and disease free survival rates to 5FU/leucovorin in patients with resected stage III colon cancer 5-FU/leucororin/oxaliplatin in resected stage II or III colon cancer patients showed improved disease-free FU/LV/oxaliplatin as the new standard chemotherapeutic regimen in the adjuvant treatment of completely resected, high-risk colon cancer The efficacy of agents such as bevacizumab and cetuximab as adjuvant therapy is being investigated Adjuvant Irradiation with or without Concurrent Chemotherapy The potential indications for adjuvant radiation therapy in colon cancer are based on analyses of patterns of failure following resection local failure in colon cancer also depends on anatomic origin 1. ascending and descending colon 2. mid-sigmoid and mid-transverse colon 3. cecal, hepatic/splenic flexure, and proximal/distal sigmoid tumors are variable depending on the amount of mesentery present, tumor extension, and the adequacy of radial margins. When colon cancers adhere to or invade adjacent structures, local failure rates exceed 30% following surgery alone. In summary, local failure occurs in patients with colonic tumors where there are anatomic constraints on radial resection margins, including tumors adherent to or invading adjacent structures. To summarize, these studies have suggested that operative bed failures in high-risk patients undergoing resection alone are at least 30%, and that the risk of local failure is reduced by the administration of adjuvant radiation therapy. Irradiated patients included those with T4N0/N+, T3N+ disease (excluding mid-sigmoid and midtransverse colon) and T3N0 patients with margins of <1 cm. ( surgery alone compared with CHRT (T3–4N0/N+ tumors radiation, with concurrent chemotherapy, usually with bolus 5- FU (500 mg/m2/d) for 3 consecutive days during the first and last weeks of radiation therapy. Radiation treatment to treat the tumor bed with an approximate 3- to 5-cm margin to a total dose of 45 Gy, Draining nodes were included if thought to be at high risk for involvement. Local control rates in T4N0 and T4N+ patients treated with radiation therapy were 93% and 72%, respectively versus 69% and 47%, respectively in patients undergoing surgery alone. Similarly, relapse-free survivals were 79% and 53%, respectively in T4N0/T4N+ patients undergoing adjuvant radiation, versus 63% and 38%, respectively undergoing surgery alone. No significant outcome differences were observed in patients with T3N0 and T3N+ lesions; however, there may be an element of selection bias in the radiation group given most patients were referred because of concerns of adequacy of local control following surgery alone. در کنسر کولونCHRT The rate of acute enteritis in patients receiving irradiation and 5-FU was 16% versus 4% in patients undergoing irradiation only. 2. Late bowel complication rates were not increased by concomitant 5-FU administration. 3. with increasing numbers of nodes involved, survival steadily decreased 4. There was a trend toward improved local control in patientsreceiving 5-FU 1. در کنسر کولونCHRT اندیکاسیون T4 tumors margin positive resection abscess/fistula formation FIGURE 58.2. Idealized postoperative anteroposterior-posteroanterior irradiation fields of extrapelvic colon cancer (tumor bed and nodal regions). If treated preoperatively, lateral fields could be added based on imaging with computed tomography of the abdomen and colon radiograph. A: Para-aortic nodes are at risk, in addition to tumor bed, due to tumor adherence to posterior abdominal wall with descending colon cancer. B: External and common iliac nodes are at risk, in addition to tumor bed, from proximal ascending colon cancer. local control rates in patients undergoing intraoperative boost were 89% compared to 18% undergoing external irradiation alone 5-year survival margin negative resection (66%) microscopic residual (47%) gross residual (23%). patients undergoing intraoperative boost demonstrated improved survival (76% vs. 26%). A study from the University of Florida of patients with locally advanced but completely resected colon cancers receiving adjuvant radiation reported a local control rate of 88%, similar to the 90% reported at the Mayo Clinic in patients who had completely resected tumors. there appeared to be a dose-response relationship to local control. The 5-year rate of local control was 96% for patients receiving 50 to 55 Gy versus 76% for patients receiving <50 Gy To assess whether the addition of radiation therapy to adjuvant chemotherapy would result in superior survival and local regional failure rates in resected, high-risk colon cancer pat No definitive conclusions can be made regarding the efficacy of postoperative irradiation with 5-FU and levamisole based on this underpowered study with many flaws; however, this study provides no data supporting its routine use. IOERT local failure 11% receiving IOERT plus EBRT versus 82% EBRT only 5-year survival 76% for patients receiving IOERT 26% for patients receiving EBRT alone] metastatic disease 5-FU–based chemo-therapy is usually administered. Recent prospective randomized trials have shown that multiple agents improve survival in patients with metastatic colorectal cancer. irinotecan, 5-FU, leucovorin, oxaliplatin Varying combinations of these drugs as well as other novel agents remain the focus of ongoing investigation in both the metastatic and nonmetastatic setting. Palliative CHRT Palliative irradiation, sometimes in combination with 5-FU–based chemotherapy, is considered for patients with specific symptoms referable to metastatic disease—brain, bone, and other sites. The combination of radiation therapy and newer agents (capecitabine, irinotecan, oxaliplatin, bevacizumab, cetuximab) remains investigational Techniques of Irradiation Field arrangement will vary depending on the site of the primary disease as well as areas judged to be at high risk for local recurrence Patient positioning (supine, prone, decubitus) should be considered in planning. the right or left decubitus position for at least a portion of their treatment, allowing displacement of the small bowel away from the treatment field. Immobilization devices may improve reproducibility. It may be useful to compare films in both the decubitus and supine positions to determine the actual amount of small bowel displacement. CT-based planning may facilitate defining the tumor bed, determining beam orientation, as well as estimating the volume of small bowel included within the treatment fields. Techniques of Irradiation total radiation dose 45 Gy in 25 fractions of 1.8 Gy per fraction (primary tumor and at-risk tissues) Reduced fields to 50 Gy T4 tumors( a total dose of 54 to 60 Gy) Any treatment beyond 50 Gy mandates exclusion of all small bowel from the field. Spinal cord dose should be limited to 45 Gy. at least two thirds of one functional kidney should receive no more than 18 to 20 Gy at least two thirds of the total liver volume should not receive more than 30 Gy. In a Mayo Clinic analysis, small bowel obstruction rates were lower when more than two treatment fields were used, and attempts should be made to implement multifield techniques, which may be aided by CT-based planning primary tumor site :with a 4- to 5-cm margin proximally and distally with 3- to 4-cm margin medially and laterally to cover areas of potential residual disease. The nodal basins in the mesentery beyond surgical margins are usually not treated as satisfactory margin clearance is obtained in these sites. An exception to this may be right colon tumors where both small bowel and right colon are supplied by ileocolic vessels, limiting the extent of resection. In some instances, treatment of the para-aortic nodes may be indicated, particularly with extensive retroperitoneal involvement by tumor. Treatment of proximal mesenteric nodes may be appropriate if nodes adjacent to the surgical or resection margin are involved. FIGURE 58.3. Idealized multiple-field preoperative or postoperative irradiation technique for a sigmoid colon cancer adherent to the bladder. Solid lines, large field; interrupted lines, boost field. A: Anteroposterior-posteroanterior. B: Paired laterals Conclusion value of adjuvant postop CHRT for patients at high risk for local relapse is unlikely to ever be addressed in a definitive randomized trial. Treatment recommendations should be made on a case-by-case basis with existing data in the setting of an informed consent. CHRT should be considered for patients with tumors (a) invading adjoining structures, (b) those complicated by perforation or fistula. and (c) where incomplete resection is performed. IOERT The use of intraoperative irradiation as a supplement to EBRT in certain T4 tumors (i.e., those with uncertain margins) may also be appropriate. For patients with tumors adherent to or invading adjacent structures, the preferred treatment sequence would be preoperative EBRT plus 5FU–based chemotherapy followed by resection with or without IOERT and postoperative systemic therapy, based on excellent results in preliminary IOERT reports from both U.S. and European institutions. CHRT →S± IOERT+CHT A similar approach would be reasonable for patients with locally recurrent cancers or with regional nodal relapse Therapy of Rectal Cancer surgery had remained the primary treatment modality, local recurrence of disease (20% to 50%) Recent results of national cooperative group studies and several European randomized trials indicate that a multimodality treatment approach results in a significantly better outcome than surgery alone. Defining the True Rectum and Impact of Tumor Location 12 to 15 cm from the anal verge. The true surgical rectum begins at the anorectal ring, just proximal to the dentate line . Tumors arising above the anorectal ring tend to metastasize along the distribution of the middle rectal vessels to the internal iliac lymph nodes as compared to tumors that may extend into the anal canal, which spread via nodes along the inferior rectal and external iliac pathways Cancers that arise in the anal canal generally metastasize to the lungs rather than the liver, .The prognosis of patients worsens with more distal location of cancer, and these differences persist even with the addition of adjunctive therapy The proximal and distal rectum have historically been defined by the level at which the peritoneum is reflected along the anterior surface of the rectum (usually at the level of S3) The middle valve of Hoston is a useful landmark that can often be identified endoscopically (usually about 6 cm from the anorectal ring), and can be used to differentiate proximal tumors from more distal lesions. All tumors that can be digitally palpated are generally considered distal cancers. Prognostic Factors Location TNM Histopathological grade LVI Circumferential tumors ulceration Mobility Obstaction age, gender, and ethnicity(may be little) Prognostic Factors Tumor extent as defined by the American Joint Committee on Cancer (AJCC) staging clearly remains the dominant determinant of survival age, gender, and ethnicity have little association with outcome but may affect choice of therapy Histopathological grade is of borderline significance, however, and signet cell cancers have a particularly poor outcome LVI has been shown on univariate analysis to have a negative impact on survival Circumferential tumors or those with total or near total obstruction (lumen <1 cm) respond very poorly, and tumors with deep central ulceration are associated with a high incidence of lymph node involvement Tumor mobility remains a key factor in both choice and outcome of treatment Mobile cancers have a much more favorable outcome as compared to tethered or fixed cancers. Tumor fixation is much more problematic in the distal rectum as the confines of the bony pelvis inhibits the surgeons ability to achieve adequate Distal rectal cancers require a more vigorous approach to adjuvant therapy than proximal cancers. FIGURE 58.4. Lymphatics of the rectum Imaging CTS EUS MRI CTS CT appears to be much more useful in identifying enlarged pelvic lymph nodes and metastasis outside the pelvis than the extent or stage of the primary tumor Standard CT does not permit the visualization of the layers of the rectal wall, and, therefore, its utility in the assessment of small primary cancers is limited The sensitivity of CT scan is reported as 50% to 80% accurate, with a 30% to 80% specificity (65% to 75% accurate for tumor staging and 55% to 65% accurate in mesorectal lymph node staging) The ability of CT scans for detecting distant metastasis, including pelvic and para-aortic lymph nodes, is higher than for detecting perirectal nodal involvement (75% to 87% vs. 45%) Any lymphadenopathy near the rectum seen on a CT scan should be considered abnormal. EUS more helpful in clinically stage rectal cancers 80% to 95% accurate in tumor staging and 70% to 75% accurate in mesorectal lymph node staging very good at T Its use is limited to lesions <14 cm from the anus and not applicable for the upper rectum or for stenosing tumors. EUS can also identify enlarged perirectal lymph nodes but is not effective outside of the perirectum (76). One area where EUS can be very useful is in determining extension of disease into the anal canal, which is an area that is poorly visualized on CT but of critical importance for planning sphincter preserving surgical procedures MRI greater accuracy in defining the extent of rectal cancer extension and also determining the location and stage of tumor . Different approaches to MRI have been explored including the use of body coils, endorectal MRI and phased array techniques. Although MRI appears to have greater accuracy, it requires a significant learning curve but is becoming a greater part of the standard presurgical work-up for rectal cancer. MRI فوائد less operator dependent a larger field of view than EUS allows assessment for proximal tumors and stenotic lesions detect involved lymph nodes on the basis of characteristics other than size extent of lateral extension of disease They are all less accurate in predicting response after neoadjuvant therapy with high rates of false positivity and should be interpreted with caution in this setting Treatment Rectum Surgery mainstay of curative treatment for carcinoma of the rectum 1. limited surgery 2. LAR 3. APR approach General principles of a surgical Removal of all gross and microscopic disease with negative proximal, distal, and circumferential margins. Radical resection, this means removal of the adjacent mesorectal tissue containing the regional lymphatics and the superior hemorrhoidal artery pedicle. The surgeon's experience with resection of colorectal cancer is an independent variable in the outcome of treatment . Distal intramural spread of tumor is rare beyond 1.5 cm, and, therefore, a 2-cm distal margin is currently considered acceptable, except in lesions that are poorly differentiated or widely metastatic Radial Margin 86% local regional recurrence (with positive margins) only 3% local regional recurrence (without lateral resection margin involvement). The mean surgical margin of resection has been shown to decrease with increasing stage of disease ranging from 14 mm for T1 cancers to 3 mm for T4 cancers, with a corresponding increase in local recurrence from 0% to 75% . Total Mesorectal Excision standard for all radical resections Sharp 12 to 15 perirectal and pelvic lymph nodes Careful nerve sparring dissection more difficult with APR than LAR( higher anastomotic leak rate) especially for low rectal lesions (15% to 17%) low rates of local recurrence (4% to 7%) and an improvement in survival approaching 80% to 85% for stage II and 65% to 70% for stage III disease Abdominoperineal Resection gold standard for surgical resection of distal rectal cancer and requires removal of the primary tumor along with a complete proctectomy slightly higher morbidity and mortality than LAR a worse quality of life higher risk of positive margins Low Anterior Resection performed not just for cancers of the upper third of the rectum but also for middle and lower third cancers good anal sphincter continence prior to considering sphincter-preserving options. LAR to APR have similar outcomes for local and distant recurrence rates and survival as long as all surgical margins are negative. The absence of a colostomy, while offering a better quality of life with LAR, can be compromised with bowel urgency and frequency or poor sphincter control Local Excision tumors to be located <8 cm from the anal verge full thickness into the fat tumor be removed in one piece with at least a 1-cm margin A primary closure to restrict local excision to patients with low-risk tumors where the risk of recurrence is <10% (i.e., T1 or favorable T2 cancers) T2 cancers need for further adjuvant therapy RTOG) Protocol 89-02 margins ≥3 mm, no LVI, no regional LN ≥2 cm by CT scan, and be grade 1 or 2 to be eligible for observation. T2 tumors with margins ≤3 mm received 59.4 to 65 Gy with 5-FU (1,000 mg for meter squared on days 1 to 3 and 29 to 31) The risk of perirectal nodal metastasis and high incidence of reported local failure rates for T2 cancers following local excision alone indicate the need for further adjuvant therapy The Cancer and Leukemia Group B (CALGB) Although this study supports the use of adjuvant radiation and chemotherapy for adverse T1 and favorable T2 tumors, one should proceed with caution given the high local failure rate. local excision should be limited to tumors: (<4 cm clinically T1 or T2, well to moderately differentiated involve <40% of the circumference of the rectum. These tumors are usually mobile, polypoid, not ulcerated, and have favorable pathology including no lymphovascular or blood-vascular invasion Adjuvant Therapy Postoperative surgery alone for T3 or T4 or node-positive patients : a 25% local failure rate 40% to 50% overall survival, CHRT : local failure rate of 10% to 15% overall survival rate of 50% to 60%. 5-FU/LV showed better relapse-free survival and disease-free survival but not overall survival as compared to MOF. The conclusions of the two NSABP trials were that while postoperative radiation treatment did not appear to improve overall survival, there was an improvement in local control Two trials GITSG this trial concluded a significant overall survival advantage of nearly double for patients who had combined modality treatment after surgical resection. the combined use of radiation and chemotherapy is more effective than postoperative radiation alone, with a greater potential for improved survival, and is recommended. The bolus 5FU dose was 500 mg/m2 on day 1 to 5 during weeks 1 and 5, whereas the continuous infusion 5-FU was 225 mg/m2 per day Favorable T3N0 Sharp mesorectal excision with LAR or APR for T3N0 rectal cancers results in low local recurrences of <10% without the use of adjuvant therapy. A limited subset of patients with T3N0 rectal cancer may have an excellent outcome with surgery alone, but there are no randomized data to support the omission of adjuvant therapy for this group of patients at the present time Side Effects of Combined Chemoradiation acute side effects nausea, vomiting, diarrhea , stomatitis with mucosal ulceration , hematological toxicity Severe late toxicity diarrhea, hand/foot syndrome ,Chronic bowel injury (25% ) rectal urgency with frequent bowel movements Treatment Technique for Postop Adjuvant Treatment areas at risk The presacral space, the primary tumor site, and (for post-APR cases) the perineum. the internal iliac and distal common iliac nodes The external iliac nodes should be covered for lesions extending to the dentate line. Treatment Technique prone position full bladder the use of bowel-displacement techniques such as a belly board (foam board table with a cutout to allow the upper-abdominal contents to fall forward) or a foam board mound designed to push the full bladder posteriorly and cephalad The use of shaped lateral fields 2D, a four-field [AP/PA]/right/left [R/L] lateral) or three-field (PA/R/L lateral) AP/PA superior port edge :L4/L5 (mid-L5 ) distal port edge :5 cm below palpable tumor or 5 cm below the best estimate of the preoperative tumor bed and (if an APR has been performed) below the perineum Lat :least a 1.5-cm margin on the pelvic brim Lateral treatment portals entire sacrum posteriorly. A radiopaque marker should be placed at the posterior aspect of the anus to make certain that blocks in the posterior-inferior aspect of the portal do not impinge on targeted portions of anorectum. Ant at least 4 cm anterior to the rectum or all macroscopic disease (determined by CT scan) Dose 4,500 cGy in 25 fractions of 180 cGy each An additional boost for patients receiving postoperative radiation Small bowel must be excluded from the boost volume after about 5,000 cGy. Typically, if small bowel cannot be excluded, the boost dose is 540 cGy. If it can be excluded, the usual boost dose is 900 cGy. (3D) treatment planning The initial CTV should include macroscopic disease with an approximately 2-cm margin in mesentery and within the course of the large bowel(the initial CTV should include rectal mesentery and nodal regions at risk) RT 3 to 6 weeks after surgery. Neoadjuvant Therapy Tumor down staging, 2. improved resectability 3. potential for expanded sphincter preservation options in the distal rectum preoperative radiation results in improvement of both local control and survival 1. Neoadjuvant Chemoradiation 45-50 Gy( 1.8 Gy)+ concurrent bolus 5-FU (350 mg/m2) plus leucovorin on days 1 to 5 during weeks 1 to 5 After surgery, four cycles of adjuvant chemotherapy Capecitabine Capecitabine requires the presence of thymidine phosphorylase (TP) for conversion to the active form of 5-FU within the cells. Studies of capecitabine in combination with radiation have shown similar response rates to 5FU, 825 mg twice a day during the course of radiation treatment. Acute toxicity of diarrhea, stomatitis, nausea, and neutropenia are also somewhat less with capecitabine than with 5-FU/leucovorin, however, the incidence of hand/foot syndrome is higher with capecitabine . Ongoing phase III trials in the United States and Europe are evaluating capecitabine and oxaliplatin delivered neoadjuvantly with radiation therapy Doses of 46 Gy or 50 Gy were more effective than 40 Gy, but there was no difference between 46 or 50 Gy. Similar results have been reported from other studies as well. Preoperative Versus Postoperative preoperative combined preoperative chemotherapy and radiation therapy resulted in significantly less local failures in the pelvis by half and also provided twice the sphincter preservation. Importantly, there was no difference in overall survival or disease-free survival between the two arms FIGURE 58.5. A: AP portal of patient with T4 rectal cancer. B: Lateral portal of a patient with T4 rectal cancer. Locally Advanced Rectal Cancer Clinical T4 tumors may not be resected completely due to tumor fixation. Preoperative radiation treatment is recommended to facilitate curative resections. IORT No IORT metastases less than T4 disease adequate margins >1 cm IORT Ten to 12.5 Gy for complete resection 12.5 to 15 Gy for microscopic residual 17.5 to 20 Gy for gross residual disease. The risk of peripheral neuropathy was 20% for doses >15 Gy. IORT improves local control, especially with a gross total resection, but not survival for locally advanced rectal cancer. Reirradiation Recurrent rectal cancer is often approached the same way as T4 disease with an aggressive treatment plan of CHRTby surgery and then adjuvant CHT. IORT is considered The 5-year overall survival is approximately 20% .The local control is about 40% in patients with no prior radiation to 10% to 20% in patients who had prior radiation.