Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Click to edit
Master title style
Welcome
to…
Click to edit Master subtitle style
How the Meaningful Use of
Electronic Health Records
relates to the Quality of
Patient Care
Wednesday, April 18, 2012
ClickMeaningful
to edit Master
title Quality
style of Care
On
Use and
Click
to edit Master subtitle style
Agenda
Moderator, Sharon Murphy Enright of Envision Change, LLC
I. On Meaningful Use and Quality of Care
60 minutes
Allen Flynn
II. Meaningful Use – Pharmacy Update
15 minutes
Burl Beasley
III. Clinical Pharmacy Program Updates
15 minutes
Trent Beach
IV. Live! Questions & Answers
20 minutes
V. Administrative Updates
10 minutes
Bob Fink
ClickMeaningful
to edit Master
title Quality
style of Care
On
Use and
Click portion
This
to edit Master
presented
subtitle
by: style
Allen Flynn, Pharm.D., CPHIMS, CHS
Chair, 2011-12
ASHP Section on Pharmacy Informatics & Technology
Solution Designer,
Health Practice Innovators
healthpracticeinnovators.com
ClickMeaningful
to edit Master
title Quality
style of Care
On
Use and
Objectives
forsubtitle
the session
Click to edit Master
style
1.
Understand what the Meaningful Use Electronic
Health Record Incentive Program is & includes
2.
Describe how & why electronic medical record
systems (EMRs) and electronic health records (EHRs)
may help improve the quality of care for ALL patients
3.
Identify several challenges to meeting the
Meaningful Use, Stage I hospital criteria
ClickMeaningful
to edit Master
title Quality
style of Care
On
Use and
What
is the
Meaningful
Click
to edit
Master
subtitle style Use (MU) of
the Electronic Health Record (EHR)
initiative of the federal government?
• Carrot & Stick Federal Incentive
• HITECH legislation in ARRA (2009)
• Eligible Hospitals & Eligible Providers
Clickdifference
to edit Master
title ‘EMR’
style & ‘EHR’*
The
between
ELECTRONIC
MEDICAL
an Application
Click
to edit Master
subtitleRECORD:
style
environment composed of the clinical data repository, clinical decision
support, controlled medical vocabulary, computerized provider order
entry and clinical documentation, used by Caregivers to document,
monitor, and manage care within a Care Delivery Organization (CDO).
EMR data is the legal record of what happened to the patient and is
owned by the CDO.
ELECTRONIC HEALTH RECORD: A Standardized subset of
each care delivery organization’s EMR, owned by the patient and has
patient input and access that spans episodes of care across multiple
CDOs. The EHR in the US will ride on the proposed National Health
Information Network (NHIN).
*Source: http://www.himssanalytics.org/docs/wp_emr_ehr.pdf
Click to edit
title style
Sharing
EMRMaster
data creates
the patient’s EHR
EMR = electronic medical record
EHR
= electronic
record
Click
to edit health
Master
subtitle
style
EMR
CHS
Hospital.
Interoperable
systems
exchanging
information.
EMR
Oncologist
Office
EHR
of the
patient
EMR
University
Hospital
EMR
Primary
Care MD
EMR
ED at
CHS
Hospital
Click to
edit Masterrelated
title style
EMR
Components
to medications
Patient Care
Process Components
Domain Specialty Systems (OB, Opthy, etc)
Click to edit Tracking
Master Boards
subtitle
style
/ Dashboards
Online Flowsheets
electronic-MAR / Bar Coded Medication Admin.
Surgery & Anesthesia Systems
Structured Clinical Documentation
Oncology Treatment & Regimen Management
Retail Pharmacy System / Inpatient Pharmacy System
Order & Medication Reconciliation
e-Prescribing / Order Sets / CPOE
AMBULATORY
INPATIENT
EDs &
HODs
EMR
EMR
Click should
to edit Master
title style
Why
we implement
EMRs & EHRs?
Click
Masterincluding
subtitle stylemedication safety
1. to↑edit
Safety,
2.
3.
4.
5.
6.
↑ Efficiency of providing care (↓ Costs)
↓ Health Disparities
Engage patients & families in their care
Improve care coordination / transitions
Improve population and public health
Click to
edit Master
title style
Does
EMR/EHR
technology
improve safety?
Health
(HIT)
and Patient
Click to IT
edit
Master
subtitle Safety:
style
Building Safer Systems for Better Care
Institute of Medicine, 2011
> Implementation methods vary (“big bang” or unit-by-unit)
> Configurability varies & configurations of the same system differ
> Clinician training approaches vary
> Workflow integration (front-line adaptations) vary
KAUSHAL et al. 2003 – AIM | “CPOE can substantially reduce med error rates”
POON, BATES et al. 2010 – NEJM | “BCMA ↓ serious admin. med errors 51%”
DORR et al. 2007 – JAMIA | “67% of reviewed HIT experiments positive”
BLACK et al. 2011 – PLOS MED | “limited evidence of benefits” and “some
evidence of new risks from these technologies”
Click to
edit Master
title style
Does
EMR/EHR
technology
save costs?
Costs
and
Benefits
Healthstyle
Click to
edit
Masterof
subtitle
Information Technology
Agency for Healthcare Research and Quality (AHRQ), 2006
“In summary … all five cost-benefit analyses predicted substantial savings from
EHR (and health care information exchange and interoperability) implementation. In
other words, the quantifiable benefits are projected to outweigh the investment costs.
However, the predicted time
needed to break even varied from three to
six to perhaps as long as 13 years.
Our evidence review found consistent predictions from five cost-benefit studies that
implementation of an EHR
system can be financially viable at the individual
organization level or through a nationwide implementation with high levels of
health care information exchange and interoperability.”
Click to
edit Master
title style
Does
EMR/EHR
technology
reduce disparity?
Impact
Electronic
Health style
Records
Click to of
edit
Master subtitle
on Racial and Ethnic Disparities in
Blood Pressure Control at US Primary Care Visits
Samal, L et al. Archives of Internal Medicine, 2012, 172(1), 75-76.
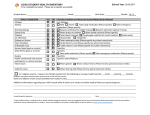
TABLE: % of patients with blood pressure relatively under control
Paper records
EMR/EHR
Blacks
69%
75%
Whites
75%
78%
Click to
edit Master
title style
Does
EMR/EHR
technology
↑ engagement?
1.
Thetorise
fall of
Googlestyle
Health
Click
editand
Master
subtitle
2. VA lessons learned, the use of KP.org by Kaiser
patients and other examples appear somewhat
positive
3. Hilton et al., PLOS ONE, paper on PHR barriers
demonstrated levels of computer literacy are an issue
4. It may be too early to understand the real value to
patients of personal health records, disease & health
management systems (a LOT is happening here!)
Click
to edit
Master
stylecoordination?
Do
EMRs
& the
EHR title
improve
Click to edit Master subtitle style
1. Can EHRs help ↓readmissions?
Predictive analysis of readmission *may* help…
2. Hysong et al., Implementation Science, 2011
“Despite facilitating information transfer between
PCPs and subspecialists, e-referrals remain prone to
coordination breakdowns.”
Click
to edit
Master
stylepublic health?
Do
EMRs
& the
EHR title
improve
Click to edit Master subtitle style
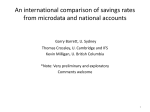
Improving Quality
Fihn, S. Circulation: Cardiovascular Quality and Outcomes. 2009; 2: 294-296
Indicator
VA
2008
VA
2007
Commercial
2007
Medicare
2007
Medicaid
2007
Diabetic retinal eye exams
86%
85%
55%
63%
50%
Diabetic microalbuminuria screening
93%
91%
81%
86%
74%
BP < 140/90, diabetic patients
78%
77%
64%
59%
56%
BP < 140/90, hypertension patients
75%
76%
62%
58%
53%
Click to
edit Master
titleuse
style
What
makes
EMR/EHR
MEANINGFUL?
meaningful,
(a)style
having a purpose,
Click
to edit Masteradj.,
subtitle
(b) full of meaning; significant
- Merriam-Webster, 2012
• Quality of EHR Use is to be measured
• Overall Quality of Use is hard to define
• Criteria-based approach is being used
Click to edit Use
Master
title
Meaningful
Stage
I –style
Eligible Hospitals
1. to
Computerized
Provider
Click
edit Master subtitle
style Order Entry (CPOE)
2.
3.
4.
5.
6.
7.
Drug-Drug Interaction & Drug-Allergy Checks
Maintain updated medical problem (DX) lists
Maintain ACTIVE medication lists
Maintain ACTIVE medication allergy lists
Record a STANDARD set of demographics
Record and track vital signs (ht, wt, bp, bmi)
ClickStage
to edit
style cont.
MU
I –Master
Eligibletitle
Hospitals,
8. to
Record
Smoking
Status
Click
edit Master
subtitle
style (>= 13 yo)
9.
10.
11.
12.
13.
14.
Report clinical quality measures to CMS
Implement ONE clinical decision support rule
Provide patients with an e-copy of their info.
Provide e-copies of discharge instructions
Be capable of exchanging clinical information
Protect and secure patient information
ClickStage
to edit
title
style
MU
I –Master
CPOE for
medication
orders
Objective
Click
to edit Master subtitle style
Use computerized provider order entry (CPOE) for medication
orders directly entered by any licensed healthcare professional who
can enter orders into the medical record per state, local and professional
guidelines.
Measure
More than 30 percent of all unique patients with at least one
medication in their medication list admitted to the eligible hospital’s or Critical
Access Hospital’s inpatient or emergency department have at
medication order entered using CPOE.
least one
ClickStage
to edit
title style Checks
MU
I –Master
DDI & Drug-Allergy
Click
to edit Master subtitle style
Objective
Implement drug-drug and drug-allergy interaction checks.
Measure
The eligible hospital or Critical Access Hospital has enabled this
functionality for the entire EHR reporting period.
ClickStage
to edit
title
style Problem Lists
MU
I –Master
Updated
Medical
Click
to edit Master subtitle style
Objective
Maintain an up-to-date problem list of current and active
diagnoses.
Measure
More than 80 percent of all unique patients admitted to
the eligible hospital’s or Critical Access Hospital’s inpatient or
emergency department have at least one
entry or
an indication that no problems are known for the
patient recorded as structured data (ICD-10 code!)
ClickStage
to edit
title style
MU
I –Master
Keep ACTIVE
Medication Lists
Click
to edit Master subtitle style
Objective
Maintain active medication list.
Measure
More than 80 percent of all unique patients admitted to the
eligible hospital’s or Critical Access Hospital’s inpatient or
emergency department have at least one entry (or
an indication that the patient is not currently prescribed any
medication) recorded as structured data.
ClickStage
to edit
title style
MU
I –Master
Keep ACTIVE
Allergy Lists
Click
to edit Master subtitle style
Objective
Maintain active medication allergy list.
Measure
More than 80 percent of all unique patients admitted to
the eligible hospital’s or Critical Access Hospital’s inpatient or
emergency department have at least one entry (or
an indication that the patient has no known medication allergies)
recorded as structured data.
ClickStage
to edit
title style
MU
I –Master
Send Clinical
Quality Measures
Click to edit Master subtitle style
Objective
Report hospital clinical quality measures to Center for Medicare
and Medicaid Services (CMS).
Measure
Successfully report to CMS hospital clinical quality measures
selected by CMS in the manner specified by CMS
ClickStage
to edit
title
style Support Rule
MU
I –Master
1 Clinical
Decision
Objective
Click
to edit Master subtitle style
Implement one clinical decision support rule related to a high
priority hospital condition along with the ability to track
compliance with that rule.
Measure
Implement one clinical decision support rule
•
•
•
•
VTE prophylaxis monitoring rules
Empiric antibiotic re-evaluation rules
Catheter-Associated UTI rules
Restraint Reminder rules
ClickStage
to edit
stylefor Patients
MU
I –Master
e-Charttitle
Copies
Objective
Click to edit Master subtitle style
Provide patients with an electronic copy of their health information
(including diagnostic test results, problem list, medication lists,
medication allergies, discharge summary, procedures) upon
request.
Measure
More than 50 percent of all patients of the inpatient or
emergency departments of the eligible hospital or Critical Access
Hospital who request an electronic copy of their health
information are provided it within 3 business days.
ClickStage
to edit
title style
MU
I –Master
e-Discharge
Instructions
Click
to edit Master subtitle style
Objective
Provide patients with an electronic copy of their discharge
instructions at time of discharge, upon request.
Measure
More than 50 percent of all patients who are discharged
from an eligible hospital or Critical Access Hospital’s inpatient or
emergency department and who
request an electronic
copy of their discharge instructions are provided it.
ClickStage
to edit
title
style
MU
I –Master
Capable
of e-exchange
of PHI
Objective
Click
to edit Master subtitle style
Capability to exchange key clinical information (for example,
problem list, medication list, medication allergies, and diagnostic
test results), among providers of care and patient authorized
entities electronically.
Measure
Performed at least one test of certified EHR technology’s
capacity to electronically exchange key clinical information
ClickStage
to edit
title style
MU
I –Master
That MUST
be all, right?
14topieces
Click
edit Master subtitle style
of the
EMR
so far…
what is
Meaningful
Use again?
CPOE
Allergies
Vital Signs
Meds
ClickStage
to edit
style cont.
MU
I –Master
Eligibletitle
Hospitals,
MENU SET – must *also* meet 5 out of 10!
Click to edit Master subtitle style
1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
Drug-Formulary Checks
Record Advance Directives
Incorporate clinical lab results as structured data
Generate lists of patients with specific conditions
Identify patient-specific educational resources
Medication reconciliation online
Provide a summary of the care record at transitions
Capable to submit immunization data electronically
Capable to report certain lab results to public health agencies
Capable to submit syndromic surveillance data to agencies
ClickStage
to edit
Master–title
style
MU
I Option
Drug-Formulary
Checks
Objective
Click
to edit Master subtitle style
Implement drug formulary checks.
Measure
The eligible hospital or Critical Access Hospital has enabled this
functionality and has access to at least one internal or external
formulary for the entire EHR reporting period.
This formulary-checking may seem mysterious yet the testing
is straight-forward. Most CPOE systems reflect the formulary
and offer a non-formulary ordering pathway. Many CPOE
systems can point users to therapeutic substitutions.
ClickStage
to edit
Master–title
style
MU
I Option
Criteria-Based
Lists
Click to edit Master subtitle style
Objective
Generate lists of patients by specific conditions to use for quality
improvement, reduction of disparities, research, or outreach.
Measure
Generate at least one report listing patients of the eligible hospital
or Critical Access Hospital with a specific condition
ClickStage
to edit
Master title
style
MU
I Option–
Individualized
Education
Objective
Click
to edit Master subtitle style
Use certified EHR technology to identify patient-specific education
resources and provide those resources to the patient if
appropriate.
Measure
More than 10 percent of all unique patients admitted to the
eligible hospital’s or Critical Access Hospital’s inpatient or
emergency department are provided patient specific education
resources.
•
New starts on Warfarin
•
FDA’s ‘REMS drugs’
ClickStage
to edit
Master–title
style
MU
I Option
Meds
Reconciliation
Objective
Click
to edithospital
Master
style Hospital who receives a
The eligible
orsubtitle
Critical Access
patient from another setting of care or provider of care or
believes an encounter is relevant should perform medication
reconciliation.
Measure
The eligible hospital or Critical Access Hospital performs
medication reconciliation for more than 50 percent
of transitions of care in which the patient is admitted to the
eligible hospital’s or CAH’s inpatient or emergency department.
ClickStage
to edit
Master–title
styleSummaries
MU
I Option
Handoff
Objective
Click
to edit Master subtitle style
The eligible hospital or Critical Access Hospital that transitions
their patient to another setting of care or provider of care or refers
their patient to another provider of care should provide
summary care record for each transition of care or referral.
Measure
The eligible hospital or Critical Access Hospital that transitions or
refers their patient to another setting of care or provider of care
provides a summary of care record for more than 50
percent of transitions of care and referrals
Click
to edit
Master title
style
So
THAT’s
Meaningful
Use
for Hospitals!
Click14
to edit Master subtitle style
Required
Criteria
> CPOE
> Allergies
> e-Copies
etc.
+
5 out of 10
Menu Set
Criteria
> Meds Rec.
> Handoff Info.
> Education
etc.
Click
to edit
Master
title style
An
EMR
-> EHR
platform
is the only way.
Click to edit Master subtitle style
Meaningful Use criteria
cannot be met using paper
processes or existing,
separate information
systems.
Click to edit Master
titlefor
style
Considerations
– CPOE
medications
1.
Order sets are key | standardize with evidence
Click to edit Master subtitle style
2. Formulary standardization will help greatly!
3. Be wary of ‘duplicate items’ in many sets
4. Order entry has to be followed by routine
order maintenance!
5. Oncology is a specialty area of CPOE focus
6. Create a sustainable testing methodology
7. Policies and procedures will need updating
Click to edit Master
title style Alerts
Considerations
– Drug-Related
1. Alert fatigue is real and problematic
Click to edit Master subtitle style
2. Contraindicated DDI lists are available
Murphy et al., Development of computerized alerts with management
strategies for 25 serious drug-drug interactions, AJHP, Vol 66, Jan 1, 2009,
p 38.
3.
4.
5.
Allergy data quality is an important area for
focused improvement
Alerts need to be speedy | ‘actionable’
Dose alerts can be useful | also infusion rate
alerts may improve safety
Click to edit Master
title style
Considerations
– Clinical
Decision Support
1.
Each CDS rule is a project (!)
Click to edit Master subtitle style
2. How with the rule(s) be assessed for success
or failure? Which outcomes are involved?
3. Forcing functions should force! Medical
leadership support will be needed.
4. Assess alert-response workflow carefully …
> who should see the alert?
> when should they see it in their workflow?
> what happens if they ignore the alert?
> what do they need to document within the alert dialog?
Click to
edit Meaningful
Master title Use,
styleStage 2 !
Here
comes
Click
to edit
Master subtitle
style
While
we’re
working
on Stage I…
Proposed Stage II Rule published by CMS in the
Federal Register March 7th
Comment period open until May 7th, 2012
Final rule expected to be published later in 2012
ClickStage
to edit
title style
MU
2 –Master
Medication-related
changes?
1. to
CPOE
now has
to bestyle
for 60% of orders
Click
edit Master
subtitle
2.
3.
4.
5.
Five Clinical Decision Support interventions
eMAR is implemented and used for more
than 10% of med orders
Medication reconciliation at more than 65%
transitions of care
Menu: e-Prescribing for more than 10% of
discharge prescriptions from the hospital
Click to edit Use,
Master
title2 style
Meaningful
Stage
– eMAR & BCMA
Click
Master
subtitle style
CMSto –edit
“We
propose
to
define eMAR as
technology that automatically
documents the administration of
medication into Certified EHR
technology using electronic tracking
sensors, e.g., RFID or bar codes”
– p. 139
Click-The
to edit
Master
title style
MU
Tech
Picture
Supply Chain Integration into Medication-Use Cycle
Product Supply Chain
C
C
P
P
P
PROACTIVE
IV DRIP
REFILLS
OUTCOME
C
C
Clinical Focus
END
Click to edit Master subtitle style
AUTOMATED
PRESCRIBING
AUTOMATED
ORDER
VERIFICATION
COMPUTER
ASSISTED
IV FLUID
ANALYSIS
DISPENSED
PRODUCT
LOCATION
TRACKING
INHERENT
ORDERING
SAFETY
PHARMACIST
PATIENT
TRIAGE
SYSTEM
AUTOMATED
COMPOUNDING
ROBOTS
PATIENT-SIDE
DELIVERY
SYSTEMS
COMPATIBILITY,
ADMINISTRATION
AUTOMATED
ADC PICK-NREPLENISH
BCMA
CDS
SMART
IV PUMPS
CDS
INDICATION,
DOSE, DDI, DFI,
UTILIZATION
BAR CODE
SCANNING
AT COMPOUND
& DISPENSE
DDI/ALLERGY
Automated
Product
Selection
AUTOMATED
DOSE PICKING
SYSTEMS
CPOE
PHARMACY
SYSTEM
EMR-EHR
EMR-EHR
ORDER
SETS
BEGIN
CDS
LABELS
EMR
Sen
DOSE, TIMING
AUTOMATED
DISPENSING
CABINETS
(ADCs)
CDS
eMAR
EMR
TRACKING
LAYER V
AUTOMATED
TREATMENT
FAILURE
IDENTIFICATION
LAYER IV
CDS
BUG-DRUG,
CORE MEASURES,
P-KINETICS
ADE
SURVEILLANCE
RULES ENGINE
LABS
HX, DX
EMR-EHR
LAYER III
Sentry 7
LAYER II
LAYER I
FOUNDATION
Click&toPharmaceutical
edit Master title
style
MU
Care
Processes
Click to edit Master subtitle style
Medication Therapy Management /
RPh-led disease management
Pharmaceutical Care Planning / Outcome objectives listed for all meds
Indication Management
Pharmacist Charting /
Patient Medication List /
/
Every med has documented indication(s)
Some specific medications have RPh notations
All meds documented w/Medication Reconciliation
ClickSuccess
to edit Master
styleB, JHIM, 2010
MU
Factors title
– Hoehn
1. to
Strategic
focus on
Qualitystyle
& Safety of care
Click
edit Master
subtitle
2.
3.
4.
5.
6.
7.
8.
9.
Physician champions / Executive Leadership engaged
Clinical IT governance is established (‘clinical ops’)
Track record of care process change successes
Organization is invested in adopting standards and driving
out unwanted workflow variance
Clinicians have experience using IT as they provide care
IT/IS department is on board and aligned with MU goals
IS infrastructure can support 24x7x365 needs
{Flynn} MU success is everyone’s success, all must take part
ClickSuccess
to edit Master
title style
MU
will be Yours
at CHS!
The Department
ofsubtitle
Veterans
Affairs and other large
Click
to edit Master
style
health systems have demonstrated precisely how quality
of care in the U.S. can be improved while costs of care
are reduced when EMR/EHR technology is widely used.
Teams around the country are taking up the challenge of
Meaningful Use and accomplishing great things for
patients. The entire, nationwide healthcare team at CHS
is destined to achieve great things as it puts EMR and
EHR technology to significant, good, meaningful use!
ClickEnd.
to edit
Master
The
Thank
you.title style
Click to edit Master subtitle style
How the Meaningful Use of
Electronic Health Records
relates to the Quality of
Patient Care
Wednesday, April 18, 2012
MEANINGFUL USE
Operations Approach to meet MU Objectives for
Attestation
Wednesday April 18, 2012
Burl Beasley, BS Pharm, MPH, MS Pharm
Operations Approach to meet MU Objectives for
Attestation
Agenda
Overview MU Stage 1
Core/Menu Sets
Examples Core Objective
Dashboard – Objective Tracker
Attestation Scorecard
Attestation Readiness
Timeline
Overview MU Stage 2
50
Meaningful Use Defined
•
The Department of Health and Human Services defines “Meaningful Use” as
furthering five (5) healthcare goals:
1.
Improving the quality, safety, and efficiency of care while reducing disparities
2.
Engaging patients and families in their care
3.
Promoting public and population health
4.
Improving care coordination
5.
Promoting the privacy and security of electronic health records
•
Federal Government has provided incentive funding to off-set a portion of the
cost of Electronic Health Record (EHR) implementation
•
This is contingent upon meeting the regulatory objectives within the required
timeframes.
CHS Goals for Achieving Meaningful Use:
•
Have all facilities Stage 1 compliant by July 2013
•
Implement any known Stage 2 technologies as they are available (for example,
Bar Code Medication Administration)
51
Meaningfully Using IT to Improve Outcomes
PATIENTCENTERED
CARE
2015 and beyond
2013 - 2015
STAGE 3:
STAGE 2:
2011 - 2013
STAGE 1:
Data capture
and sharing
52
Advanced
clinical
processes
Improved
Outcomes
Meaningful Use (MU) Technology Staged Approach
Foundational
Stage 1
Stage 2
Components
Components
Components
(2011 - 2012)
(Deadline July 2013)
(2 Yrs. Post Stage 1)
Certified Health Information
System (HIS)
ED CPOE
Bar Code
Medication Admin
Certified Emergency
Department System (EDIS)
ED Clinician
Documentation
Technology Foundation
Inpatient CPOE
Inpatient Phys. Doc
Clinical Doc/Vitals I&O
Order Set Governance
Evidence Based Orders
Physician Portal
Health Information
Exchange (HIE) Integration
Medication Reconciliation
Personal Health Record
(PHR)
Quality & Metrics Reporting
HIPAA Security Assessments
By
53
Meaningful Use Objectives – Stage 1 Core Set
• CPOE for Medication Orders
• Drug-Drug, Drug-Allergy
Checks
• Record Demographics
• Up-to-date Problem Lists
• Active Medication List
• Active Medication Allergy List
• Chart Changes in Vital Signs;
Growth Chart; BMI
Calculation
5454
• Record Smoking Status >/= 13
yrs old
• One Clinical Decision Support
Rule
• Report Clinical Quality
Measures
• E-Copy of Health Information
• E-Copy of Discharge
Instructions
• E-Exchange Key Clinical
Information
• Security and Data Protection
Meaningful Use Objectives – Stage 1 Menu Set
• Drug Formulary Checks
• Advanced Directives
• Incorporate Lab Results
into EMR
• Generate Lists of Patients
• Identify Patient-Specific
Education
• Medication Reconciliation
• Provide Summary of Care
at Transitions
• e-Submit Immunization
Data
• e-Submit Reportable Lab
Results
• e-Submit Syndromic
Surveillance Data
CHS recommends 1, 2, 3, 7, 8 (Optional 4 and 5)
5555
Core Objective 1 – CPOE for Medication Orders
56
Core Objective 1 – CPOE for Medication Orders
CHS Strategy for Stage 1
• ProMED
– Physicians enter orders directly into ED system
– No pharmacy check, orders are directly from physician to nurse
Status/Roadmap
•
•
•
•
•
57
ProMED update to MU-certified version
Implement EPD (physician documentation & order entry)
Update policies
Update workflows
30% threshold for all inpatients and ED observation
Core Objective 2 – Drug-Drug/Drug-Allergy Interaction
Checks
58
Core Objective 2 – Drug-Drug/Drug-Allergy
Interaction Checks
CHS Strategy for Stage 1
• Functionality should be turned on in ProMED and Pharmacy system
Status/Roadmap
• Hospital must attest yes that this functionality was active during the
entire reporting period
• Screenshot of functionality in action
• Documentation that the functionality has been active since beginning
of reporting period
– i.e. build documentation
59
Core Objective 4 – Active medication list
60
Core Objective 4 – Active medication list
CHS Strategy for Stage 1
• Clinicians will pull up a medication profile report from each system
Status/Roadmap
• Need sample medication profile
• Procedure/Workflow for who maintains the home medication list
• De-identified print screen of an indication of the “no active
medication” field within the med list.
• De-identified print screen of the review function field within the med
list
• Threshold Greater than 80%
61
Core Objective 5 – Maintain active medication allergy list
62
Core Objective 5 – Maintain active medication
allergy list
CHS Strategy for Stage 1
• Nursing will enter allergies on admission to be verified by Pharmacy
Status/Roadmap
• Information entered in AS400 where the patient first came into the
system…
• Procedure/Workflow on the “no known allergy” field within the system
• De-identified print screen of a patient’s record showing their allergies
• Print screen of the allergy vocabulary name and version
• Procedure/Workflow on who maintains, reviews, adds, etc. the allergy list
• Need a screenshot of an example
• 80% threshold
63
Menu Set Objective 1 – Drug formulary check
64
Menu Set Objective 1 – Drug formulary check
CHS Strategy for Stage 1
• Functionality should be turned on and maintained in the Pharmacy
system
Status/Roadmap
• Hospital must attest yes that this functionality was active during the
entire reporting period
• Print screen of the formulary or preferred drug list that is available in
the Electronic Health Record
• Procedure/Workflow for drug formulary checking
• Print screen of the alert of when a non-formulary medication is
selected in the system
65
Core Objective 6 – Record Demographics
66
Core Objective 6 – Record Demographics
CHS Strategy for Stage 1
• Demographic information will be entered by registration staff at time
of registration.
• Mortality information will be gathered at time of final coding.
Status/Roadmap
• Print screen of all the required data elements within demographics
• Procedure/Workflow for how race and ethnicity are collected and
stored within the system
• Describe the process if a patient declines to answer race and ethnicity
• De-identified print screen of where a preliminary assessment and
clinical impression for cause of death is recorded in the system
67
Core Objective 8 – Record Smoking Status
68
Core Objective 8 – Record Smoking Status
CHS Strategy for Stage 1
• Smoking status requirement met for all platforms
• Data should be completed at the time of the admission assessment
Status/Roadmap
• Procedure/Workflow for capturing patients smoking status
• Print screen of the smoking field in the system
69
Core Objective 10 – Clinical Decision Support Rule
70
Core Objective 10 – Clinical Decision Support Rule
CHS Strategy for Stage 1
• Clinical decision support rule may be decided at facility level
• Falls utilizing the Morse Fall Scale with appropriate assessments
Status/Roadmap
• Print screen showing the system configuration dates or a copy of the
change control log indicating when the decision build was enabled
• Print screen of the real time notification that occurs in the system
• Procedure/Workflow of if an override occurs in the system (e.g., does
an alert track this)
• Procedure/Workflow on what structured elements will be used in the
decision support from the system (e.g., patient’s problem list, med list,
demographics, etc.)
71
MU Readiness Review – Scorecard & Dashboard
• Review Attestation requirement and process and roles
– Operations Support - RCI
– Internal Audit
– Revenue Management
• Attestation Readiness Scorecard
• Dashboard MU Objective Tracker
– Completion and update of dashboard with
multidisciplinary group
72
Readiness Scorecard
• Shows progress implementing foundational elements
towards achieving each of the Stage 1 objectives
– Progress rated on scores of 0-5 per objective
• “% Score without EMR”
– Readiness before EMR application go live
• “Live in EMR”
– % Readiness with EMR application
73
Attestation Scorecard ….Next Steps
• When Attestation Readiness shows…
– Total score = 6 for each of the 14 core objectives
– Total score = 6 for 5 of 10 menu objectives
• Then Operations Support…
– Sets up Attestation Readiness Assessment with IT Compliance and
Audit in preparation to attest
• Upon successful audit & completion of 90-day reporting
period…
– Revenue Management submits attestation form to CMS
74
Overview of Readiness Assessment Process
•
Internal Audit was assigned ownership of the Meaningful
Use(MU) readiness assessment project and partnered with
Ernst & Young(E&Y) and Operations Support to develop an
effective approach for assessing MU Stage 1 compliance.
•
The E&Y MU readiness framework is a proven best practice
designed approach that was successfully piloted at two CHS
facilities in 2011.
•
The readiness assessments are designed to evaluate each
core and menu set objective and determine if the usage
outcomes are meeting MU Stage 1 requirements.
75
Readiness Assessment - Corporate Support
Operations Support Regional Clinical
Informaticist (RCI)
Internal Audit (IA)
Revenue Management
(RM)
By
76
Monitoring, Reporting and Filing Timeline
30 Days
USAGE MONITORING
77
90 Days
ATTESTATION REPORTING
14 Days
ATTESTATION FILING
Monitoring, Reporting and Filing Timeline
30 Day Usage Monitoring Period
USAGE MONITORING
30 Days
• RCI notifies IA that facility
is ready to start 90
attestation period
• IA issues Engagement
Letter and RFI to facility
C-team.
• RFI is returned to IA prior
to the start of the 90
attestation period
• IA schedules on-site visit
78
ATTESTATION REPORTING
90 Days
• IA analyzes RFI deliverables prior
to on-site visit. Works with RCI
and facility to address any issues
or questions
• IA performs interim readiness
assessment 2-3 weeks after start
of 90 day attestation period
• IA completes interim assessment,
issues report and schedules an
exit meeting to discuss results
• IA monitors remediation efforts (if
applicable)
• End of 90 period – IA requests
final MU statistics report and
analyzes results
ATTESTATION FILING
14 Days
• IA issues final report to
management
• RM provides attestation
package to facility to
complete and return to
Corporate
• Attestation package is
approved by facility
management and
retuned to Corporate
• IA validates attestation
package and sends
package to RM
• RM enters data into CMS
website
• Stage 1 compliance is
achieved
Monitoring, Reporting and Filing Timeline
90 Day Attestation Reporting Period
USAGE MONITORING
30 days
• RCI notifies IA that facility
is ready to start 90
attestation period
• IA issues Engagement
Letter and RFI to facility
C-team.
• RFI is returned to IA prior
to the start of the 90
attestation period
• IA schedules on-site visit
79
ATTESTATION REPORTING
90 days
• IA analyzes RFI deliverables prior
to on-site visit. Works with RCI
and facility to address any issues
or questions
• IA performs interim readiness
assessment 2-3 weeks after start
of 90 day attestation period
• IA completes interim assessment,
issues report and schedules an
exit meeting to discuss results
• IA monitors remediation efforts (if
applicable)
• End of 90 period – IA requests
final MU statistics report and
analyzes results
ATTESTATION FILING
14 days
• IA issues final report to
management
• RM provides attestation
package to facility to
complete and return to
Corporate
• Attestation package is
approved by facility
management and
retuned to Corporate
• IA validates attestation
package and sends
package to RM
• RM enters data into CMS
website
• Stage 1 compliance is
achieved
Monitoring, Reporting and Filing Timeline
14 Day Attestation Filing Period
USAGE MONITORING
30 days
• RCI notifies IA that facility
is ready to start 90
attestation period
• IA issues Engagement
Letter and RFI to facility
C-team.
• RFI is returned to IA prior
to the start of the 90
attestation period
• IA schedules on-site visit
80
ATTESTATION REPORTING
90 days
• IA analyzes RFI deliverables prior
to on-site visit. Works with RCI
and facility to address any issues
or questions
• IA performs interim readiness
assessment 2-3 weeks after start
of 90 day attestation period
• IA completes interim assessment,
issues report and schedules an
exit meeting to discuss results
• IA monitors remediation efforts (if
applicable)
• End of 90 period – IA requests
final MU statistics report and
analyzes results
ATTESTATION FILING
14 days
• IA issues final report to
management
• RM provides attestation
package to facility to
complete and return to
Corporate
• Attestation package is
approved by facility
management and
returned to Corporate
• IA validates attestation
package and sends
package to RM
• RM enters data into CMS
website
• Stage 1 compliance is
achieved
Stage 1 Readiness Assessment – Interim Scorecard
81
Stage 1 Readiness Assessment – Detailed Report
82
Stage 1 Readiness Assessment – Final Report
83
MU Readiness Review - Summary
•
•
•
•
•
•
•
•
84
Facility to determine 30 day usage monitoring period
Facility to determine 90 day reporting period
Clinical Decision Support – Falls Assessment Test
Menu Items 1, 2, 3, 7, and 8 (Optional 4 & 5)
Policy and Procedure Updates
Workflow review and validation
Governance Structure (MU, BCMA, CPOE, etc)
Establish MU Core Team Meetings
– MU Objectives 14 Core and 5 Menu
– Zynx Order Set
Suggested Attestation Dates/Readiness
Determine Usage Monitoring Date – May 1st 2012
Determine Attestation DATE - June 1st 2012
Attestation Date: September 1st 2012
Attestation Period – 90 Days
– 30 Day Usage Monitoring - May 1- May 31
– 90 Day Attestation Period June 1 – August 31st
– Attestation Filing 14 days (EST at: August 20 – 31 2012)
• Continued Monitoring by CHS and CMS
•
•
•
•
st
– Of note: Reporting period for facility may not be the same as audit
period for CMS
85
Meaningful Use Stage 2
• Stage 1 starts the process for continuation to Stage 2, 3 …..4
• Published Federal Register
– March 7th 2012 proposed rules
• Eligible Hospitals and Critical Access Hospitals:
– Federal Fiscal Year-based
– Starts on October 1, 2013
• Modifications to
– Core Set
– Menu Sets
• eRx, HIE, structured data
86
Meaningful Use Stage 2 (continued)
• Eligible Hospitals and Critical Access Hospitals must meet or
qualify for exclusion on:
• 16 Core Objectives
• 2 of 4 Menu Objectives
• Exchange of Key Clinical Information Objective is being
replaced by Transitions of Care Objective
• Re-evaluating the process for providing patients with an
eCopy of health information to address practical challenges
facing EPs, EHs, and CAHS
87
MU Stage 2 vs Stage 1
88
MU Stage 2 Core (cont)
– Medications – Increase threshold of CPOE to 60%
• Incorporate Medications, Lab, Radiology Orders
– Electronic transmission of Prescriptions
• eRX
• Compare to a formulary and transmit
• Drug-drug and drug allergy checks (eHR reporting period)
– Clinical Decision Support Measures
• 5 CDS –
– Possible ……HbA1C, INR, FSBS, CrCl
•
Generate and transmit permissible discharge prescriptions electronically (eRx)
– More than 10% of hospitals discharge medication orders are:
• Compared to at least one drug formulary
• Transmitted electronically using Certifiend eHR
•
89
Medication Reconcilation – moved to core measure
Impact on Patient Care
• Drug interactions represent 3-5% of preventable hospital
adverse drug reactions (ADRs)
– $136 Billion yearly
– LOS, Cost and Mortality double for ADR patients
• Important contributor to the number of ED visits and
hospital admissions
• ADR’s increase exponentially with 4 or more medications
• Prescribe to avoid ADR’s – DDI and DAI
•
90
http://www.fda.gov/Drugs/DevelopmentApprovalProcess/DevelopmentResources/DrugInteractionsLabeling/ucm11484
8.htm
Meaningful Use is predicted to have the following
effects
•
•
•
•
•
Reductions in repeated tests
Reductions in medical record keeping costs
Decreased length of stay
Increased patient safety
Reduction in medical errors
– eMAR is critically important to making care safer by reducing medication errors
which may make care more affordable
– eMAR cuts in half the adverse drug event (ADE) rates for nontiming medication
errors
– Hospital bar-coding demonstrated that associated ADE cost savings allowed
hospitals to break even after 1 year and begin reaping cost savings going
forward.
91
Meaningful Use Program Communication
For more information, please visit the CHS Meaningful Use program
website, i-connect, at:
http://chsweb.chs.net/i-connect/Pages/default.aspx
92
• Selected References:
•
Medicare and Medicaid Programs; Electronic Health Record Incentive Program—
Stage 2 available at:
– http://www.gpo.gov/fdsys/pkg/FR-2012-03-07/pdf/2012-4443.pdf
– Accessed April 3rd 2012
•
HIMMS Executive Summary MU Stage 2 NOTICE OF PROPOSED RULE MAKING:
42 CFR 412, 413, and 495 available at:
– http://www.himss.org/content/files/20120301_HIMSS_ExecutiveSummaryMU_Stage
2.pdf
– Accessed April 3rd 2012
93
Clinical Pharmacy Program Updates
Trent A. Beach, Pharm.D., M.B.A., M.H.A., FASHP
Director, Clinical Pharmacy Services
Community Health Systems
94
Overview
Clinical Initiative in Medical Imaging
Sentri7 Discussion
Formulary Standardization
Medication Use Evaluations
95
Medical Imaging
Myocardial Perfusion Imaging (MPI)
Myocardial perfusion Imaging
Myocardial blood flow is impacted by stenosis (>40%) with
hyperemia
• A nuclear-medicine study used to
evaluate the adequacy of blood
supply to the heart muscle
Disparity in flow between normal and diseased
myocardium with stenosis
PET & SPECT capture images of relative myocardial
perfusion before and after radionuclide administration and
hyperemia
Comparative images determine the coronary flow reserve
and areas of compromised myocardial perfusion.
Uren et al. NEJM. 1994; 330: 1782-8.
Iskandrian. Am J Cardiol. 2007; 99: 1619-20.
Hyperemia is preferably induced by exercise, however
agents such as dipyridamole, adenosine, and regadenoson,
which temporarily increase blood flow, is used in ~40% of
the 8.5 millions MPI studies performed annually in the U.S.
96
Medical Imaging
LexiScan® Conversion Initiative
Convert regadenoson (LexiScan®) to
dipyridamole in radionuclide myocardial
perfusion imaging
Develop a procedure with
the imaging staff for
ordering and dispensing
pharmacy-prepared
dipyridamole syringes
Generic adenosine could
be considered a
secondary position if
significant physician
pushback to dipyridamole
97
IVIG
Eliminate
Gammagard
Convert to
Octagam
Convert 25%
Flebogamma
Move 25% of
Flebogamma to
Octagam
Move to single
lyophylized
powder
Convert
Gammagard
S/D to
Carimune
98
• Role in
redefining
pharmacy
productivity
• Internal
performance
• External
benchmarking
Expectations
• Phase I
Hospitals
• Begin May
• Phase II
Hospitals
• Begin
September
New metrics
Implementation Timeline
Sentri7
• Utilization
• Performance
• Scheduling &
Assignments
99
Formulary Standardization
eHR
CPOE
Zynx Initiative
Standard Formulary
100
Medication Use Evaluations
Minimum Annual
Target – 4
MRSA MUE
Sign up now
with HPG
Documented
Improvement
• Performance
• Utilization
• Safety
101
Questions?
102
To Ask a Question & Adjust Control Panel
Expand or Collapse
Type your question here
103
103
Click
to edit Master title style
CE
Numbers:
LIVE
Click PRESENTATION
to edit Master subtitle style
ACPE # 204-999-12-082-L04P
Credit: 2.0 CE Hours for Live Webinar and post test
Transcript ID: 12082
HOME STUDY
ACPE: 204-999-12-507-H04P
Credit: 1.5 CE Hours for Recorded webinar post-test
Transcript ID: 12507
Obtaining ACPE Continuing Education
Click to edit Master title style
Continuing
Education
Pharmacists
Click to edit
Masterforsubtitle
style
The American Society of Health-System Pharmacists is accredited by the
Accreditation Council for Pharmacy Educations as a provider of continuing
pharmacy education.
Live Webinar
This live knowledge-based CE activity offers 2.0 contact hours (0.20
CEUs) of continuing education credit for pharmacists. Participants must
successfully complete the online post-test and evaluation to earn CE
credit.
LIVE PRESENTATION CE Number:
ACPE # 204-999-12-082-L04P
Credit: 2.0 CE Hours for Live Webinar and post test
Transcript ID: 12082
105
Obtaining
ACPE
Continuing
Education
Click to edit Master title style
To receive
ACPE
continuing
credit you must
Click
to edit
Master
subtitleeducation
style
complete the assessment test found on the ASHP website.
Go to ASHP Learning Center at http://ce.ashp.org. Login
using your ASHP username (email address) and password.
If you are not an ASHP member/customer create a free account by
clicking on the “Register” button and follow the prompts.
A. Enter your username (email address) and password, click submit
B. Enter your name, address, and select your customer class as
“Pharmacist”
C. Complete all the required fields to create your customer record.
ClickObtaining
to edit Master
title style Education
ACPE Continuing
After
you
login
to
the ASHP
Learningstyle
Center, you should be on the My
Click
to
edit
Master
subtitle
Account screen; click on “Exam Center” on this screen.
Search for tests on the “Exam Center” screen using keyword “CHS” then
click on the “Filter” button. The Key word search will give you a listing of
all the CHS webinar tests available online (both live and recorded).
1. Click the check box to select the test and click “Register” button to add
the test to you test bank.
2. Click on “Start” to begin the test, answer the questions
3. Click on “Grade Test” at the end to see your score. (70% or higher to
pass). If you do not pass, you have one more opportunity to retake the
test.
4. Click on the link to complete the evaluation and click the “Finish” button
before you can print your statement.
5. Your CE Statement should appear on the screen to print.
Obtaining ACPE Continuing Education
Click to edit Master title style
The recorded knowledge-based CE (home study) activity offers 1.5 hours
Click
to edit Master subtitle style
(0.15 CEU) of continuing pharmacy education credit upon successful
completion of the online post-test and evaluation. The recorded Webinar will
be available within 4 - 7 days after the live webinar and posted on the CHS
Pharmacy Services website.
From this site, select the “Pharmacy Conferences and National Pharmacy
Directors” section. This link will take you to the 2011 presentations with
handouts. From this screen, you can select the appropriate handout to view
or print and the recorded presentation desired.
HOME STUDY
ACPE: 204-999-12-507-H04P
Credit: 1.5 CE Hours for Recorded webinar post-test
Transcript ID: 12507
108
ClickObtaining
to edit Master
title style Education
ACPE Continuing
Note: to
If you
not complete
evaluation, you will see your
Click
editdid
Master
subtitlethe
style
transcript page with a link to complete the evaluation next to
the title of the test.
If you have any questions, contact the Educational Services
Division staff at [email protected]
109
UPDATE ON CURRENT CHS
INITIATIVES AND STRATEGIES
Bob Fink, Pharm.D., M.B.A., FASHP, BCNSP, BCPS
Chief Pharmacy Executive
Community Health Systems
110