Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
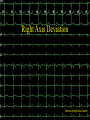
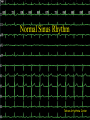
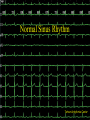
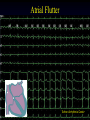
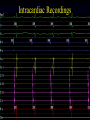
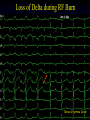
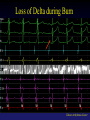
Electrocardiography & Cardiac Arrhythmias Saeed Oraii MD, Cardiologist Interventional Electrophysiologist Tehran Arrhythmia Clinic Some slides have accompanied notes. To view them you can right click on the screen, choose ‘Screen’ and then ‘Speaker Notes’. Tehran Arrhythmia Center ECG A graphic recording of electrical potentials generated by the heart A noninvasive, inexpensive and highly versatile test Tehran Arrhythmia Center Normal Pathway of Electrical Conduction Tehran Arrhythmia Center Cardiac Action Potential Tehran Arrhythmia Center Cardiac action potentials from different locations have different shapes Tehran Arrhythmia Center Electrophysiology • Electric currents that spread through the heart are produced by three components – Cardiac pacemaker cells – Specialized conduction tissue – The heart muscle • ECG only records the depolarization and repolarization potentials generated by atrial and ventricular myocardium. Tehran Arrhythmia Center Electrocardiograph 1903 Tehran Arrhythmia Center Normal Electrocardiogram Tehran Arrhythmia Center ECG Waveforms Labeled alphabetically beginning with the P wave Tehran Arrhythmia Center QRS-T Cycle Corresponds to Different Phases of Ventricular Action Potential Tehran Arrhythmia Center Limb Leads Tehran Arrhythmia Center Precordial Leads Tehran Arrhythmia Center Position of Precordial Electrodes Tehran Arrhythmia Center Precordial Leads Tehran Arrhythmia Center 3-D Representation of Cardiac Electrical Activity Tehran Arrhythmia Center Timing Intervals Tehran Arrhythmia Center Vector Concept • Cardiac depolarization and repolarization waves have direction and magnitude. • They can, therefore, be represented by vectors. • ECG records the complex spatial and temporal summation of electrical potentials from multiple myocardial fibers conducted to the surface of the body. Tehran Arrhythmia Center Limb Leads Directions Tehran Arrhythmia Center Vector Concept Tehran Arrhythmia Center Ventricular Depolarization Tehran Arrhythmia Center QRS Axis Tehran Arrhythmia Center Determination of QRS Axis Tehran Arrhythmia Center Direction of Propagation Tehran Arrhythmia Center Determination of QRS Axis Tehran Arrhythmia Center Determination of QRS Axis Tehran Arrhythmia Center Main Vector Tehran Arrhythmia Center Normal QRS Axis Tehran Arrhythmia Center Left Axis Deviation Tehran Arrhythmia Center Right Axis Deviation Tehran Arrhythmia Center Major ECG Abnormalities Tehran Arrhythmia Center Right Atrial Enlargement Tehran Arrhythmia Center Left Atrial Enlargement Tehran Arrhythmia Center Left Ventricular Hypertrophy Tehran Arrhythmia Center Right Ventricular Hypertrophy Tehran Arrhythmia Center RVH, RA enlargement Tehran Arrhythmia Center Left Bundle Branch Block Tehran Arrhythmia Center Left Bundle Branch Block Tehran Arrhythmia Center Right Bundle Branch Block Tehran Arrhythmia Center RBBB Tehran Arrhythmia Center RBBB, RAD (Bifascicular Block) Tehran Arrhythmia Center RBBB, LAD (Bifascicular Block) Tehran Arrhythmia Center Myocardial Ischemia • ECG is the cornerstone in the diagnosis of myocardial ischemia • Findings depend on several factors: – – – – – Nature of the process, reversible vs. irreversible Duration, acute vs. chronic Extent, transmural vs. subendocardial Localization, anterior vs. inferoposterior Other underlying abnormalities Tehran Arrhythmia Center Acute Ischemia Tehran Arrhythmia Center Myocardial Infarction Tehran Arrhythmia Center Acute Pericarditis Tehran Arrhythmia Center Metabolic Abnormalities Tehran Arrhythmia Center Hyperkalemia K 6.9 Tehran Arrhythmia Center Same patient K 3.9 Tehran Arrhythmia Center Hypothermia, Osborn Wave Tehran Arrhythmia Center Hypothermia, Corrected Tehran Arrhythmia Center Right Axis Deviation Tehran Arrhythmia Center Tehran Arrhythmia Center Superior P Wave Axis Tehran Arrhythmia Center Tehran Arrhythmia Center Normal Sinus Rhythm Tehran Arrhythmia Center Tehran Arrhythmia Center Anterior MI Tehran Arrhythmia Center Tehran Arrhythmia Center RBBB and Inferior MI Tehran Arrhythmia Center Tehran Arrhythmia Center LA Enlargement and Prolonged PR Interval TehranArrhythmia ArrhythmiaCenter Center Tehran LBBB TehranArrhythmia ArrhythmiaCenter Center Tehran LA Enlargement and Prolonged PR Interval TehranArrhythmia ArrhythmiaCenter Center Tehran Left Anterior Hemiblock TehranArrhythmia ArrhythmiaCenter Center Tehran LVH and LA Enlargement TehranArrhythmia ArrhythmiaCenter Center Tehran Anterior MI TehranArrhythmia ArrhythmiaCenter Center Tehran Old Inferior MI TehranArrhythmia ArrhythmiaCenter Center Tehran RA Enlargement TehranArrhythmia ArrhythmiaCenter Center Tehran RBBB, LAH, Prolonged PR (Trifascicular Block) TehranArrhythmia ArrhythmiaCenter Center Tehran RBBB and Inferior MI TehranArrhythmia ArrhythmiaCenter Center Tehran Tehran Arrhythmia Center Cardiac Arrhythmias Tehran Arrhythmia Center Normal Pathway of Electrical Conduction Tehran Arrhythmia Center Normal Sinus Rhythm • Normal and constant P wave contours • Normal P wave axis • Rate between 60 and 100 bpm Tehran Arrhythmia Center Normal Sinus Rhythm Tehran Arrhythmia Center Tehran Arrhythmia Center Anatomical Aspects of Normal Sinus Node • Located at the superior anterolateral portion of right atrium near its border with the superior vena cava • It is an epicardial structure near sulcus terminalis • From endocardial approach the closest approach is near the superior end of crista terminalis Tehran Arrhythmia Center Sinus Node Function • • • • • The dominant cardiac pacemaker Highly responsive to autonomic influences Decreasing rate with vagal stimulation Increasing rate with sympathetic activity Normal sinus rate under basal conditions is 60-100 bpm. Tehran Arrhythmia Center Sinus Tachycardia • Sinus rhythm exceeding 100 bpm in adults • Usually between 100 and 180 bpm but may be higher with extreme exertion • Maximum heart arte decreases wit age from near 200 bpm to less than 140 bpm • Gradual onset and termination Tehran Arrhythmia Center Sinus Tachycardia Tehran Arrhythmia Center Sinus Tachycardia Causes • Common in infancy and childhood • Normal response to a variety of physiological and pathological stresses – – – – – – Exertion, anxiety Hypovolemia, anemia Fever Congestive heart failure Myocardial ischemia Thyrotoxicosis • Drugs • Inflammation Tehran Arrhythmia Center Sinus Bradycardia • Sinus rhythm at a rate less than 60 bpm • Can result from excessive vagal or decreased sympathetic tone as well as anatomic changes in sinus node • Frequently occurs in healthy young adults, particularly well-trained athletes • Sinus arrhythmia often coexists Tehran Arrhythmia Center Sinus Bradycardia Tehran Arrhythmia Center Sinus Bradycardia Causes • • • • • • • • Hypothyroidism Drugs During vomiting or vasovagal syncope Increased intracranial pressure Hypoxia, hypothermia Infections Depression Jaundice Tehran Arrhythmia Center Sinus Arrhythmia • Phasic variation in sinus cycle length • Maximum minus minimum sinus cycle length exceeds 120 msec. • May be considered the most common form of arrhythmia • Respiratory form is a normal event • Common in the young esp. with slower heart rates or enhanced vagal tone Tehran Arrhythmia Center Sinus Arrhythmia Tehran Arrhythmia Center Wandering Pacemaker • Passive transfer of dominant pacemaker focus from sinus node to latent pacemakers in other atrial sites or AV junctional tissue • Occurs in a gradual fashion over the duration of several beats Tehran Arrhythmia Center Wandering Pacemaker ECG • A cyclical increase in RR interval • A PR interval that gradually shortens to less than 120 msec • A change in P wave contour that becomes negative in lead I or II or is lost within the QRS Tehran Arrhythmia Center Wandering Pacemaker Tehran Arrhythmia Center Inappropriate Sinus Tachycardia • Persistent sinus tachycardia at rest or with minimal exertion • Usually occurs in otherwise healthy people • More common in health care personnel • May result from a defect in either sympathetic or vagal nerve control of sinus node automaticity or an abnormality of intrinsic heart rate • Some cases may need radiofrequency ablation of sinus node Tehran Arrhythmia Center Sinus Node Dysfunction Mechanisms • A disease affecting a limited amount of tissue at or near the sinus node causing dysfunction of impulse formation or propagation or recovery from overdrive suppression • A disease affecting the atria in general that consequently affects the sinus node function and also frequently generates atrial arrhythmias Tehran Arrhythmia Center Sinus Node Dysfunction ECG Manifestations • • • • • Sinus bradycardia Sinus pauses Sinus arrest Atrial asystole Sinus exit block Tehran Arrhythmia Center Sinus Pause Tehran Arrhythmia Center Sinoatrial Exit Block 1st and 2nd degree Tehran Arrhythmia Center Sinus Node Dysfunction Etiology • Most often in elderly as an isolated phenomenon • Drugs • Infiltration of atrial myocardium • Interruption of blood supply • Hypothyroidism, advanced liver disease, severe hypoxia, acidemia … Tehran Arrhythmia Center High Vagal Tone • • • • Usually in the young Normal heart rate response during exercise Normal intrinsic heart rate Bradycardia may be severe enough to cause syncope (especially in familial form) Tehran Arrhythmia Center Sick Sinus Syndrome • A combination of symptoms (dizziness, fatigue, confusion, syncope and congestive heart failure) caused by sinus node dysfunction • Atrial tachyarrhythmias may accompany sinus node dysfunction <bradycardia-tachycardia syndrome> Tehran Arrhythmia Center Sick Sinus Syndrome Clinical Manifestations • Predominantly seen in the elderly • Most patients with sinus node dysfunction are asymptomatic • Two types of presentations – Syncope or near-syncope – Fatigue or worsening heart failure Tehran Arrhythmia Center Sick Sinus Syndrome Diagnosis • • • • Holter monitor recordings Intrinsic heart rate by autonomic blockade Sinus node recovery time Sinoatrial conduction time The most important step is to correlate symptoms with ECG findings. Tehran Arrhythmia Center Normal SNRT Tehran Arrhythmia Center Abnormal SNRT Tehran Arrhythmia Center SA Block during Overdrive Pacing Tehran Arrhythmia Center Sinus Arrest after Termination of AF Tehran Arrhythmia Center Loop Recorder Showed Junctional Rhythm during Syncope Tehran Arrhythmia Center Sinus arrest with syncope Tehran Arrhythmia Center Therapy for Sick Sinus Syndrome • Based mostly on symptoms and any clinical documentation of cardiac arrhythmia associated with these symptoms • Drug therapy is rather limited • Most effective treatment is pacing therapy • Anticoagulation in certain situation Tehran Arrhythmia Center Tehran Arrhythmia Center Heart Block • • • • Disturbance of impulse conduction Transient or permanent Due to anatomical or functional impairment Must be distinguished from interference, a normal phenomenon that is a disturbance of impulse conduction caused by physiological refractoriness due to inexcitability from a preceding impulse Tehran Arrhythmia Center AV Conduction Disturbances Clinical Significance • Heart block may be asymptomatic or lead to syncope or cardiac arrest • Clinical significance of conduction abnormalities depend on: – The site of disturbance – The risk of progression to complete block – The probability that a subsidiary escape rhythm distal to the site of block develops and is stable Tehran Arrhythmia Center AV Block Types • First degree AV block • Second degree AV block – Mobitz type I (Wenckebach) – Mobitz type II • Third degree block (Complete heart block) • High degree (advanced) AV block Tehran Arrhythmia Center First Degree AV Block • Conduction time is prolonged but all impulses are conducted. • PR interval exceeds 0.2 sec in adults • Site of conduction delay may be in the AV node (most commonly), in the His-Purkinje system or both. Tehran Arrhythmia Center First Degree AV Block Tehran Arrhythmia Center Second Degree AV Block • Block of some atrial impulses at a time when physiological interference is not involved • Non-conducted P waves can be infrequent or frequent, at regular or irregular intervals, and can be preceded by fixed or lengthening PR intervals. • The association of P with QRS is not random. Tehran Arrhythmia Center Mobitz Type I Second Degree AV Block • Also called Wenckebach block • Typical type characterized by progressive PR prolongation culminating in a nonconducted P wave • Narrow QRS in most cases Tehran Arrhythmia Center WB Tehran Arrhythmia Center Wenckebach Block Tehran Arrhythmia Center Wenckebach Block • Atypical pattern in over half the cases • The site of block is almost always in the AV node. • Generally benign and does not advance to more advanced AV block • Can occur in normal children and welltrained athletes Tehran Arrhythmia Center Mobitz Type II Second Degree AV Block • PR interval remains constant prior to the blocked P wave • Commonly associated with bundle branch blocks Tehran Arrhythmia Center Mobitz Type II Second Degree AV Block Tehran Arrhythmia Center Mobitz Type II Second Degree AV Block Tehran Arrhythmia Center Mobitz Type II Second Degree AV Block • Site of block His-Purkinje system in most case • Often antedates the development of AdamsStokes syncope and complete AV block • Never observed in normal people • An indication for implantation of permanent pacemaker even in asymptomatic cases Tehran Arrhythmia Center 2:1 AV Block Tehran Arrhythmia Center 2:1 AV Block Tehran Arrhythmia Center 2:1 AV block Tehran Arrhythmia Center Complete AV block • No atrial activity conducts to the ventricles • AV dissociation is present. The atria and ventricles are controlled by independent pacemakers. • Ventricular focus is usually located just below the site of block. • Higher sites are more stable with a more faster escape rate. Tehran Arrhythmia Center Complete AV block Tehran Arrhythmia Center Complete AV block Isorhythmic AV Dissociation Tehran Arrhythmia Center Advanced AV block Block in two or more consecutive P waves Tehran Arrhythmia Center AV Conduction Disturbances Etiology • Degenerative diseases are the most common causes • A variety of other diseases may be responsible: myocardial infarction, drugs, acute infections, infiltrative diseases, neoplasms, etc. • Hypervagotonia Tehran Arrhythmia Center Investigation of the Site of AV Conduction Disease by Electrophysiologic Study (EPS) Tehran Arrhythmia Center Cardiac Pacemakers • The treatment of symptomatic bradyarrhythmias is implantation of cardiac pacemakers. Tehran Arrhythmia Center Cardiac Pacing Tehran Arrhythmia Center First Implanted Pacemaker Tehran Arrhythmia Center Common Uses for Permanent Pacemaker Therapy Tehran Arrhythmia Center AV Block With Carotid Massage Tehran Arrhythmia Center Long Asystole Tehran Arrhythmia Center Sinus Pause and Junctional Escape Beats Tehran Arrhythmia Center Sinus Pause and Junctional Escape Beats TehranArrhythmia ArrhythmiaCenter Center Tehran BradycardiaTachycardia Syndrome Tehran Arrhythmia Center Mobitz Type I (Wenckebach) Tehran Arrhythmia Center 2:1 AV block TehranArrhythmia ArrhythmiaCenter Center Tehran Complete Heart Block TehranArrhythmia ArrhythmiaCenter Center Tehran Sinus Pause TehranArrhythmia ArrhythmiaCenter Center Tehran Sinus Arrhythmia TehranArrhythmia ArrhythmiaCenter Center Tehran Sinus Tachycardia TehranArrhythmia ArrhythmiaCenter Center Tehran Wandering Pacemaker TehranArrhythmia ArrhythmiaCenter Center Tehran Sinus Tachycardia TehranArrhythmia ArrhythmiaCenter Center Tehran Wandering Pacemaker TehranArrhythmia ArrhythmiaCenter Center Tehran Asystole and Junctional Escape Rhythm Tehran Arrhythmia Center Tehran Arrhythmia Center Tachyarrhythmias Tehran Arrhythmia Center Tachyarrhythmias Mechanisms Automaticity Tehran Arrhythmia Center Tachyarrhythmias Mechanisms Triggered activity Tehran Arrhythmia Center Tachyarrhythmias Mechanisms Reentry Tehran Arrhythmia Center Premature Complexes Tehran Arrhythmia Center Ventricular Premature Complexes Compensatory Pause Interpolated VPC Tehran Arrhythmia Center Premature Complexes • The most common arrhythmias • Detected during 24h Holter monitoring in over 60% of adults • May cause palpitations or be asymptomatic • May trigger more serious tachyarrhythmias • May be associated with a normal heart or a variety of cardiac disturbances Tehran Arrhythmia Center Variability of Ventricular Ectopy with Age • Effect of age on probability (%) of having more than a given number of PVCs per 24 hours in subjects with normal hearts. 60% 50% > 0 PVCs > 50 PVCs > 100 PVCs 40% 30% 20% 10% 0% 10-29 30-39 40-49 50-59 60-69 Data from Kostis JB. Circulation. 1981;63(6):1353. Age Tehran Arrhythmia Center Ventricular Premature Complexes • Without heart disease, PVCs have not been shown to be associated with any increased incidence in morbidity or mortality • In the presence of underlying disease (ischemia, heart failure …) they may add to the risk of the disease. No treatment is, however, shown to definitely decrease this increased risk. Tehran Arrhythmia Center Atrial Fibrillation • • • • • The most common sustained arrhythmia Incidence increases progressively with age. Prevalence: 0.4% of overall population Mortality rate double that of control AF is characterized by disorganized atrial activity without discrete P waves Tehran Arrhythmia Center Atrial Fibrillation Tehran Arrhythmia Center Atrial Fibrillation • Undulating baseline or atrial deflections of varying amplitude and frequency ranging from 350 to 600 bpm. • Irregularly irregular ventricular response. Tehran Arrhythmia Center Atrial Fibrillation • Morbidity related to: – – – – – – Excessive ventricular rate Pause following cessation of AF Systemic embolization Loss of atrial kick Anxiety secondary to palpitations Irregular ventricular rate Tehran Arrhythmia Center Atrial Fibrillation • Persistent AF usually in patients with cardiovascular disease – Valvular heart disease – Hypertensive heart disease – Congenital heart disease • Paroxysmal AF may occur with acute hypoxia, hypercapnia or metabolic or hemodynamic derangements • Normal people with emotional stress or surgery or acute alcoholic intoxication • Lone AF Tehran Arrhythmia Center Atrial Fibrillation • Therapeutic Goals: – Control of ventricular rate – Restoration and maintenance of sinus rhythm – Prevention of thromboembolism Tehran Arrhythmia Center Atrial Flutter • Regular atrial tachyarrhythmia with atrial rate between 250-350 bpm. • Flutter waves are seen as saw-tooth like atrial activity Tehran Arrhythmia Center Atrial Flutter • Atrial Flutter is a form of atrial reentry localized to right atrium. • Typically the ventricular rate is half the atrial rate, but the ventricular response may be 4:1, 2:1, 1:1 etc. Tehran Arrhythmia Center Atrial Flutter Circuit Tehran Arrhythmia Center Atrial Flutter Tehran Arrhythmia Center Tehran Arrhythmia Center Atrial Flutter • Most often in patients with organic heart disease • Usually less long-lived than AF and may convert to AF. • Control of ventricular rate is difficult in atrial flutter • The most effective treatment is DC cardioversion Tehran Arrhythmia Center Paroxysmal Supraventricular Tachycardia (PSVT) • Usually at a rate of 150-250 bpm • No organic heart disease in the majority • Presentations – Palpitations – Chest discomfort,dyspnea, lightheadedness – Frank syncope – SCD Tehran Arrhythmia Center PSVT Tehran Arrhythmia Tehran ArrhythmiaCenter Center PSVT Mechanism • Reentry in the vast majority • Reentry may be localized to sinus node, atrium, AV junction or a macroreentrant circuit involving a bypass tract (WPW) • In the absence of WPW, more than 90% are due to reentry through AV node or a concealed bypass tract Tehran Arrhythmia Center AV Nodal Reentrant Tachycardia (AVNRT) • The most common form of paroxysmal supraventricular tachycardia (about 70%) • More common in women (66%) • Usually a regular narrow QRS complex tachycardia • No P wave is usually evident during the tachycardia. Retrograde P waves may occasionally be seen at the end of QRS. Tehran Arrhythmia Center Longitudinal Dissociation Within AV Node Atrium Slow Pathway Fast Pathway His Bundle Tehran Arrhythmia Center AVNRT Tehran Arrhythmia Center AVNRT Tehran Arrhythmia Center Preexcitation Tehran Arrhythmia Center Wolff-Parkinson-White Syndrome Tehran Arrhythmia Center Tehran Arrhythmia Center AV Reentrant Tachycardia (AVRT) • Incorporates a bypass tract as part of the tachycardia circuit. • Surface ECG: – Manifest with short PR interval and delta wave (preexcitation) – Concealed with normal ECG • Prevalence of ECG pattern: 0.1% to 0.3%. Tehran Arrhythmia Center AVRT Tehran Arrhythmia Center Concealed Accessory Pathway TehranArrhythmia ArrhythmiaCenter Center Tehran PSVT Treatment • Vagal maneuvers particularly carotid sinus massage • AV nodal blocking drugs – – – – Adenosine Verapamil Propranolol Digoxin • DC cardioversion if hypotensive • Radiofrequency ablation Tehran Arrhythmia Center Electrophysiologic Study (EPS) Tehran Arrhythmia Center Catheter Positions at Fluoroscopy Tehran Arrhythmia Center Intracardiac Recordings Tehran Arrhythmia Center Radiofrequency Ablation (RFA) Through femoral vein and right atrium Tehran Arrhythmia Center Loss of Delta during RF Burn Tehran Arrhythmia Center Tehran Arrhythmia Center Loss of Delta during Burn Tehran Arrhythmia Center Ventricular Arrhythmias Definitions • Premature Ventricular beats – Single beats – Ventricular Bigeminy, the appearance of one PVC after each sinus beat – Couplets, two consecutive premature beats – Triplets, three consecutive premature beats – Salvos, runs of 3-10 premature beats • Accelerated Idioventricular Rhythm (Slow VT), rate 60100 bpm • Ventricular Tachycardia (VT), rate over 100 bpm • Ventricular Flutter, regular large oscillations at a rate of 150-300 bpm • Ventricular Fibrillation (VF), irregular undulations of varying contour and amplitude Tehran Arrhythmia Center Ventricular Tachycardia Classification • Duration – Sustained VT defined as VT that persists for than 30 s or requires termination because of hemodynamic collapse – Nonsustained VT, 3 beats to 30 s • Morphology – Monomorphic – Polymorphic Tehran Arrhythmia Center Salvos Tehran Arrhythmia Center Sustained Monomorphic VT Tehran Arrhythmia Center Sustained Polymorphic VT Tehran Arrhythmia Center VT, Holter Recording Tehran Arrhythmia Center VT Presentations Tehran Arrhythmia Center VT Etiology • VT generally accompanies some form of structural heart disease most commonly: – Ischemic heart disease – Cardiomyopathies • Primary electrical abnormalities – Long QT syndromes – Brugada syndrome • Idiopathic VT Tehran Arrhythmia Center Electrocardiographic Differentiation of VT vs. SVT with Aberrancy • • • • • • Clinical history AV dissociation QRS morphology QRS axis Fusion beat Capture beat Tehran Arrhythmia Center A-V Dissociation, Fusion, and Capture Beats in VT V1 E ECTOPY F C FUSION CAPTURE Fisch C. Electrocardiography of Arrhythmias. 1990;134. Tehran Arrhythmia Center Fusion and Capture Beats in VT F C C C C Fisch C. Electrocardiography of Arrhythmias. 1990;135. Tehran Arrhythmia Center VT Prognosis • Depends on the underlying disease state – 75% first year mortality in the first few weeks after MI – Poor prognosis in patients with left ventricular dysfunction – No increased risk in those with idiopathic VT Tehran Arrhythmia Center Ventricular Fibrillation Tehran Arrhythmia Center Sudden Death Syndrome • Incidence – 400,000 - 500,000/year in U.S. – Only 2% - 15% reach the hospital – Half of these die before discharge • High recurrence rate Tehran Arrhythmia Center Underlying Arrhythmia of Sudden Death Primary VF 8% Torsades de Pointes 13% VT 62% Bradycardia 17% Adapted from Bayés de Luna A. Am Heart J. 1989;117:151-159. Tehran Arrhythmia Center Snapshot of Death Tehran Arrhythmia Center Tehran Arrhythmia Center Return of Life Not the usual case ! Tehran Arrhythmia Center Tehran Arrhythmia Center Clinical Substrates Associated with VF Arrest • • • • • • Coronary artery disease Idiopathic cardiomyopathy Hypertrophic cardiomyopathy Long QT syndrome RV dysplasia Rarely: WPW syndrome Tehran Arrhythmia Center VT/VF Therapeutic Options • • • • Antiarrhythmic drugs Anti-tachycardia pacing Radiofrequency ablation Implantable defibrillators Tehran Arrhythmia Center Earliest Defibrillator in Clinical Use, 1899 Tehran Arrhythmia Center First Implantable Defibrillator 1970 Tehran Arrhythmia Center Thoracotomy Lead System, the technique used at the beginning Tehran Arrhythmia Center Nonthoracotomy Lead System Tehran Arrhythmia Center Pectoral Implantation The Current Technique Tehran Arrhythmia Center Tiered Therapy Defibrillators Tehran Arrhythmia Center Defibrillator Function Tehran Arrhythmia Center Interrogated ICD Event VT, treated appropriately by burst pacing therapy Tehran Arrhythmia Center Interrogated ICD Event VT (CL 320ms), no response to burst pacing therapy Tehran Arrhythmia Center Interrogated ICD Event VT (CL 320ms), cardioverted by DC shock Tehran Arrhythmia Center Clinical Uses of Defibrillator Therapy Tehran Arrhythmia Center Tehran Arrhythmia Center Congenital Long QT Syndrome A Frequently Missed Diagnosis Long QT Interval Tehran Arrhythmia Center Long QT Interval Tehran Arrhythmia Center Long QT Interval Tehran Arrhythmia Center Clinical Manifestations • Long QT syndrome is characterized by the presence of a long QT interval (usually over 440 ms) and emergence of ventricular arrhythmias. • The presenting arrhythmia is a polymorphic ventricular tachycardia called ‘Torsade de Pointes’. • Patient present with recurrent syncope or sudden cardiac death. • Early diagnosis by ‘looking at ECG’ is critical! Tehran Arrhythmia Center Torsade de Pointes • Prolonged QT interval associated with a polymorphic VT characterized by QRS complexes that change in amplitude and cycle length, giving the appearance of oscillations around the baseline • Congenital or acquired Tehran Arrhythmia Center Brugada Syndrome Definition • Clinical-electrocardiographic diagnosis based on: - High incidence of sudden cardiac death - Structurally normal heart - Characteristic ECG pattern Tehran Arrhythmia Center ECG Abnormalities • ST segment elevation in V1-V3 • QRS complex resembling RBBB • J-point elevation Tehran Arrhythmia Center Brugada ECG Pattern Tehran Arrhythmia Center Brugada ECG Pattern Tehran Arrhythmia Center History • First time in 1986: a 3-year polish boy • First presentation at NASPE meeting in 1991 • First paper by Pedro and Josep Brugada in 1992 • In the Philippines as “ bangungut” • In Japan as “Pokkuri” • In Thailand as “ Lai tai”, SUDS Circ. 1997 • Thai men correlated to Brugada, SUNDS Hum. Mol. Gen. 2002 Tehran Arrhythmia Center Brugada Syndrome Prevalence in men (8:1 ratio males: females) Familial incidence (autosomal dominant with incomplete penetrance ranging between 5 and 66 per 10 000) True prevalence is difficult to estimate as the ECG pattern is often concealed. It is endemic in Southeast Asia including: Thailand, Japan, Laos, Cambodia, Vietnam, the Philippines, and China. Appearance of arrhythmic events at an average age of 40 years Tehran Arrhythmia Center Clinical Manifestations Sudden cardiac death Syncope, seizure, agonal respiration, Episodes at night during sleep with labored respiration, agitation, loss of urinary control, recent memory loss Most commonly occurs during sleep, in particular during the early morning hours Early diagnosis is of utmost importance The only treatment is currently implantation of an ‘Implantable Cardioverter Defibrillator’. Tehran Arrhythmia Center Tehran Arrhythmia Center WWW.IranEP.org [email protected] Tehran Arrhythmia Center