Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
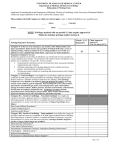
SAN GORGONIO MEMORIAL HOSPITAL PRIVILEGE DELINEATION LIST RADIOLOGY NAME OF APPLICANT:__________________________________ DATE:______________________ YEAR OF BOARD CERTIFICATION/RECERTIFICATION____________ RIVILEGES CATEGORY CATEGORY I QUALIFICATIONS/CRITERIA CATEGORY 2 MODERATE SEDATION PRIVILEGES R # Done 24 mos D P/O G DIAGNOSTIC CORE PRIVILEGES (Procedures considered included in minimal formal training.) QUALIFICATIONS: 1. Successful completion of an accredited Radiology residency training program, AND, 2. Board qualified/certified by the American Board of Radiology with specific training and recent experience in privileges requested, OR, (in lieu of Board Certification) 3. Demonstrate comparable competency to perform the privileges requested based on proctoring reports, reference letters, activity/operative reports or other documentation acceptable to the Medical Service, AND have been practicing in Radiology for the past 5 years. 4. Privileges will be proctored per Medicine Service Rules and Regulations. DIAGNOSTIC NON-CORE PRIVILEGES Physicians applying for Diagnostic Non-Core Privileges must have completed a Radiology Residency and must have exercised these privileges at least two times within the past two years or provide evidence of Continuing Medical Education. QUALIFICATIONS: 1. Board qualified/certified by American Board of Radiology, 2. AND, documented evidence of additional training, experience and competence by hands-on training, special certification, or written documentation of supervised numbers performed and outcomes. 3. Privileges will be proctored per Medicine Service Rules and Regulations. IV MEDICATIONS FOR SPECIAL PROCEDURES (All medications with potential loss of protective reflexes, regardless of route of administration) QUALIFICATIONS: • Documentation of in-house training for non-anesthesiologists in I.V. Sedation including possible complications, OR, • Successful completion of didactic and practical examination. • Training and documentation to be reviewed and approved by Anesthesia Services. CATEGORY 1 - DIAGNOSTIC CORE PRIVILEGES Diagnostic Radiology Bone/Soft tissues – head/neck, chest, abdomen, pelvis, spine, extremities, IVP, fluoroscopies and barium studies Mammography Ultrasound Head, neck, chest, abdomen, pelvis, extremities, small parts, OB, vascular, breast Computerized Tomography Head/neck, chest, abdomen, pelvis, spine, extremities Magnetic Resonance Imaging (MRI) Head/neck, chest, abdomen, pelvis, spine, extremities, breast San Gorgonio Memorial Hospital Radiology Privilege Delineation R # Done D P/O G 24 mos CATEGORY 1 - DIAGNOSTIC CORE PRIVILEGES Nuclear Medicine Thyroid, parathyroid, hematopoietic, reticuloendothelial and lymphatic, GI, musculoskeletal, cardiovascular, respiratory, CNS and GU. Drainage Procedures Percutaneous fluid and abscess drainage-neck, chest, abdomen, pelvis, extremities, breast, small parts. Galactography and breast localization, lumbar puncture, myelogram, cystogram, cystourethrogram (retrograde/voiding), nephrostogram, urethrogram, hysterosalpingogram, sonohystergram, therapeutic steroid/anesthetic injection. Telemedicine Interpretation or diagnostic medical images by way of digital transmission and display of images, which include, but are not limited to, general diagnostic imaging (originating site) from a distant site (site of reading). R # Done 24 mos D P/O G CATEGORY 2 NON-CORE PRIVILEGES Echocardiogram Therapeutic Nuclear Medicine (Thyroid) Iodine-131 (hyperthyroid therapy only) Strontium Therapy Diagnostic Radiology Biliary and Genitourinary Procedures Percutaneous transhepatic cholangiogram, percutaneous biliary duct stone removal, dilatation, stent placements. Percutaneous nephrostomy, tract dilatation, stent placements. Stone Extractions-Biliary and Urinary. Percutaneous Biopsy-Soft tissue and bone, including neck, chest, breast, abdomen, pelvis, extremities. Interventional Procedures IVC filter placement Venography-extremity, pelvis, IVC and SVC Thrombolytic therapy-catheter, dialysis graft/fistula Venous access catheters-placement and removal (short/long term) Moderate Sedation Use of Fluoroscopy (certificate required) Revised/Approved 4/05/2016 Legend: [R] = Requested [# Done 24 mos.] = Procedures done in the last 24 months [D] = Deferred/Denied [P/O] =Granted with Proctoring/Observation [G] = Granted San Gorgonio Memorial Hospital Radiology Privilege Delineation STAFF CATEGORY REQUESTED: ACTIVE ( Involved in the care of at least twenty (20) patients per year in this Hospital) COURTESY (Have not had more than twenty (20) patient contacts within the past twelve (12) months) CONSULTING (To render clinical services within one’s area of competence and expertise) TELEMEDICINE Distant Site location in which equipment is located delivering patient care services – Originating site location where the patient is located. The provider contract with the entity that serves as the Distant Site. SIGNATURE OF APPLICANT: _________________________________ DATE ________________ PRINT NAME OF APPLICANT: _______________________________________ APPROVALS: Applicant may perform privileges and procedures as indicated: [ ] Exceptions/Limitations:_______________________________________________________________ _____________________________________________________________________________________ I have reviewed the applicant's health status and can attest that there is no health problems that exists that could affect his or her ability to perform the privileges requested. ____________________________________________________ ________________________________ Medical Services Committee Chairman Date ____________________________________________________ ________________________________ Credentials Committee Chairman Date ____________________________________________________ ________________________________ Medical Executive Committee Chairman Date ____________________________________________________________________________________ Board of Directors Chair Date Revised/Approved 4/05/2016 Legend: [R] = Requested [# Done 24 mos.] = Procedures done in the last 24 months [D] = Deferred/Denied [P/O] =Granted with Proctoring/Observation [G] = Granted