Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
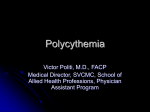
Evolving Therapeutic Options for Polycythemia Vera: Perspectives of the Canadian Myeloproliferative Neoplasms (MPN) Group Shireen Sirhan, Lambert Busque, Lynda Foltz, Kuljit Grewal, Caroline Hamm, Nicole Laferriere, Pierre Laneuville, Brian Leber, Elena Liew, Harold J. Olney, Jaroslav Prchal, Anna Porwit, Vikas Gupta Clinical Lymphoma, Myeloma and Leukemia Journal Background Objectives • To discuss the potential impact of the changing landscape of PV management on daily practice • To assist Canadian physicians in the management of PV patients • To standardize the management of PV across the country Development • Each member of the writing committee was assigned a specific topic – Several meetings and teleconferences were held to finalize the content Key Topics • Diagnostic Approaches – Current and proposed WHO criteria for diagnosis of PV • • • • Prognosis and Risk Assessment Goals of Therapy Therapeutic Approaches Specific Situations Key Topics • Diagnostic Approaches – Current and proposed WHO criteria for diagnosis of PV • • • • Prognosis and Risk Assessment Goals of Therapy Therapeutic Approaches Specific Situations Current and Proposed WHO Criteria for Diagnosis of PV 2008 WHO Diagnostic Criteria for PV1 2014 Proposed Revision of WHO Diagnostic Criteria for PV2 Major Criteria 1. Hemoglobin >185 g/L (men), >165 g/L (women), or evidence of increased red cell volume Hemoglobin >165 g/L (men), >160 g/L (women) or hematocrit >49% (men) >48% (women) 2. Presence of JAK2 V617F or other functionally similar mutation (e.g., JAK2 exon 12 mutation) Bone marrow findings consistent with WHO criteria with pleomorphic megakaryocytes Presence of JAK2 mutation Minor Criteria 1. BM biopsy showing hypercellularity for age with trilineage myeloproliferation Subnormal serum erythropoietin level 2. Serum erythropoietin level below the normal reference range 3. Endogenous erythroid colony formation in vitro Diagnosis of PV requires meeting either both major criteria and 1 minor criterion or the first major criterion and 2 minor criteria. Diagnosis of PV requires meeting either all three major criteria or the first two major criteria and one minor criterion. Adapted from: 1. Thiele J, et al. Lyon, France: IARC Press:2008:40-43 and 2. Tefferi A, et al. Leukemia. 2014;28(7):1407-1413. MPN Group Positioning Regarding the Proposed WHO Diagnostic Criteria • We acknowledge the necessity of appropriately diagnosing masked PV • However, there are concerns about potential misuse of these criteria for screening for PV • We emphasize that: – – Hb levels above the suggested threshold should not be taken in isolation, but rather in the context of other potential signs and symptoms indicative of PV. The intent of lowering the thresholds is to more accurately differentiate between JAK2-positive ET and mPV rather than to serve as a base for population screening • We suggest the cost-effectiveness analysis of the new proposed criteria Proposed Algorithm for PV Diagnosis Blood JAK2V617F & Erythropoietin screen JAK2V617F Positive* Polycythemia Vera Needed to confirm PV in JAKV617F negative cases JAK2V617F Negative Low Erythropoietin High Erythropoietin Screen for JAK2exon 12 mutation Not Polycythemia Vera Bone marrow biopsy Clinical clues : Splenomegaly, thrombosis, aquagenic pruritus, and erythromelalgia Laboratory clues: Thrombocytosis, leukocytosis, and leukocyte alkaline phosphatase score *Not specific for PV. The possibility of a false positive or false negative mutation test result can be addressed by the concomitant testing of EPO level, as more than 85% of patients with PV have low serum EPO concentrations Adapted from Tefferi A. Am J Hematol. 2013;88(6):507-516. MPN Group Positioning Regarding Other Investigations Bone marrow evaluation • Limited additional value for diagnostic purpose in JAK2 V617F-positive patients with erythrocytosis; currently it is not routinely required • Information regarding age-adjusted bone marrow cellularity and grade of fibrosis may have prognostic value and, as such, help in optimizing therapeutic approaches • In addition, a baseline BM biopsy might be essential in cases where the diagnosis is unclear. Cytogenetic testing • May have prognostic value but not routinely performed in Canada Mutations other than those involving the JAK-STAT pathway • Increasing interest due to next-generation sequencing (NGS) Key Topics • Diagnostic Approaches • Current and proposed WHO criteria for diagnosis of PV • • • • Prognosis and Risk Assessment Goals of Therapy Therapeutic Approaches Specific Situations Risk Factors Based on available evidence we identified risk factors for the following 4 outcomes: • Thrombosis – Age and/or prior history of thrombosis* • Overall Survival • Age, history of thrombosis, leukocytosis, abnormal karyotype • Transformation to PPV-MF • JAK2 allele burden, disease duration (>10 years) • Transformation to AML • Age, abnormal karyotype, leukocyte count ≥15X109/L, Exposure to P32, busulfan, and pipobroman * the main indication for cytoreductive therapy Risk Factors Associated with Thrombosis and Overall Survival 1. 2. Risk Factors for Thrombosis1 Hazard Ratio (95% Confidence interval [CI]) P-value Age >65 (without prior thrombosis) 1.96 (1.29-2.97) P=0.0017 History of thrombosis (patients < 65) 2.00 (1.22-3.29) P=0.0061 Age > 65 years with prior thrombosis 4.35 (2.95-6.41) P<0.0001 Risk Factors for Reduced Survival2 Hazard Ratio (95% Confidence interval [CI]) P-value Age >61 7.4 (3.9-14.1) P<0.0001 Leukocytosis (>10.5x109/L) 3.3 (1.8-6.1) P=0.0001 History of venous thrombosis 3.9 (1.9-8.2) P=0.0002 Abnormal karyotype 3.1 (1.6-5.8) P=0.0005 Marchioli R, et al. J Clin Oncol. 2005;23(10):2224-2232. Tefferi A, et al. Leukemia. 2013;27(9):1874-1881 Risk Factors Associated with Disease Transformation Risk Factors for Post-PV MF Hazard Ratio (95% Confidence interval [CI]) P-value JAK2 allele burden1 1.05 (1-1.1) P=0.03 Disease duration >10 years2 15.24 (4.22-55.06) P<0.0001 Risk Factors for AML Hazard Ratio (95% Confidence interval [CI]) P-value Age >613 6.3 (1.8-22) P=0.004 Abnormal karyotype*3 3.9 (1.2-13.1) P=0.03 Leukocyte count ≥15X109/L*3 3.9 (1.3-11.6) P=0.01 Exposure to P32, busulfan, and pipobroman4 5.46 (1.84-16.25) P=0.0023 *Multivariable analysis; karyotype included as a covariate (n=383) 1. 2. 3. Tefferi A, et al. Leukemia. 2013S;27(9):1874-1881. Passamonti F, et al. Leukemia. 2010;24(9):1574-1579. Marchioli R, et al. J Clin Oncol. 2005;23(10):2224-2232. 4. Finazzi G, et al. Blood. 2005;105(7):2664-2670. Key Topics • Diagnostic Approaches • Current and proposed WHO criteria for diagnosis of PV • • • • Prognosis and Risk Assessment Goals of Therapy Therapeutic Approaches Specific Situations Goals of Therapy • Prevention of occurrence or recurrence of thrombosis – By decreasing the risk of thrombosis survival is extended • Control of Hct and normalization of other blood counts • Mitigation of disease-related symptoms Control of Cardiovascular Risk factors • Currently, there are no specific data informing lipid or blood pressure target ranges for individuals with PV – It is prudent to manage atherosclerotic risk factors (including hypertension, hyperlipidemia, diabetes) and encourage smoking cessation • Clinicians should refer to the Framingham Heart Study and the risk assessment tool incorporated into Canadian guidelines for general prevention of cardiovascular disease1 • Based on available data, Hct target <45% is the widely accepted standard of care in routine clinical practice.2 – Hematocrit > 45 is associated with a significantly higher death rate due to cardiovascular events or major thrombosis when compared with hematocrit <45% – The data is limited by the quality of available studies 1. Anderson TJ, et al. Can J Cardiol. 2013;29(2):151-167. 2. Marchioli R, et al. N Engl J Med. 2013;368(1):22-33. Cardiovascular Risk Assessment WHO TO SCREEN Men 40 years of age and women 50 years of age or post-menopausal (consider earlier in ethnic groups at increased risk, such as South Asians or First Nations individuals) OR All patients with the following conditions, regardless of age • Current cigarette • Family history of smoking hyperlipidemia • Diabetes • Erectile dysfunction • Arterial hypertension • Chronic kidney • Family history of disease premature CVD • Inflammatory disease • HIV infection • COPD • Clinical evidence of atherosclerosis or abdominal aneurysm • Clinical manifestation of hyperlipidemia • Obesity (BMI >27) HOW TO SCREEN For all: History and examination, LDL, HDL, TG, non-HDL (will be calculated from profile), glucose, eGFR Optional: apoB (instead of standard lipid panel), urine albumin:creatinine ratio (if eGFR <60, hypertension, diabetes) Framingham risk score <5% Repeat every 3-5 years Anderson TJ, et al. Can J Cardiol. 2013;29(2):151-167. Framingham risk score 5% Repeat every year Importance of Keeping Hematocrit < 45% Death from Cardiovascular Causes or Major Thrombotic Events 1.0 Total Cardiovascular Events 1.0 Low HCT 0.9 Low HCT 0.9 P=0.004 by log-rank test 0.8 High HCT High HCT Hazard Ratio 0.7 Low HCT 5/182 (2.7%) 1.00 High HCT 18/183 (9.8%) 3.91 (95% CI, 1.45–10.53) 0.0 0.6 0 6 12 18 24 30 36 42 P=0.01 by log-rank test 0.8 48 Risk of CV death or major thrombotic event is significantly higher when HCT > 45% Hazard Ratio 0.7 Low HCT 8/182 (4.4%) 1.00 High HCT20/183 (10.9%) 2.69 (95% CI, 1.19– 6.12) 0.0 0.6 0 6 12 18 24 30 36 42 48 Significantly higher probability of CV event in patients with HCT > 45% Hematocrit between 45 and 50% is associated with a significantly higher death rate due to cardiovascular events or major thrombosis when compared with hematocrit <45% (HR = 3.91, 95% CI 1.45-10.53, P = 0.004) Marchioli R, et al. N Engl J Med. 2013;368(1):22-33. Correlation Between White Blood Cells and Hematocrit White-Cell Count (x10-3/mm3) • Significantly higher WBC count in the high-HCT group Low HCT High HCT vs low-HCT group 75th Percentile Median 25th Percentile 13 12 75th Percentile Median 25th Percentile 11 10 9 8 7 6 5 4 0 0 6 12 18 24 30 36 42 Months HCT: hematocrit; WBC: white blood cell Marchioli R, et al. N Engl J Med. 2013;368(1):22-33 MED/JAKp/0001 Key Topics • Diagnostic Approaches • Current and proposed WHO criteria for diagnosis of PV • • • • Prognosis and Risk Assessment Goals of Therapy Therapeutic Approaches Specific Situations Phlebotomy Advantages • Immediate reduction of Hct • Well tolerated – Some patients might experience fatigue after the procedure; this might be managed by adequate hydration *Cytoreduction is recommended in patients at high risk for thrombosis 1. 2. Kim J, Wessling-Resnick M. J Nutr Biochem. 2014;25(11):1101-1107. Tobiasson M, et al. Med Oncol. 2010;27(1):105-107. Disadvantages • Inconvenience • Does not decrease the platelet or leukocyte counts* • Frequent phlebotomies may – Lead to iron deficiency, abnormal red blood cell morphology, and eventually reactive thrombocytosis. – Rarely, phlebotomy-induced iron deficiency might lead to complications such as cognitive problems and restless leg syndrome1,2 Antiplatelet Drugs and Anticoagulants • Low-dose Aspirin® is recommended for all PV patients without contraindications1 • For patients with acute thrombotic events, acute antithrombotic therapy, as per general thrombosis management is recommended (LMWH followed by warfarin) – There is no consensus regarding the optimal duration of anticoagulation • Due to high rate of recurrence of thrombosis, an individualized risk-factor based approach is recommended – German and Austrian consensus guidelines recommend assessment after 3-6 months2 • Aspirin® is a reasonable option after 3-6 months of warfarin and cytoreduction in patients with VTE at initial diagnosis • Long-term anticoagulation may be favored in patients with high-risk features (recurrent, splanchnic, or life-threatening VTE) and low bleeding risk 1. Barbui T, et al. J Clin Oncol. 2011;29(6):761-770. 2. Kreher S, et al. Ann Hematol. 2014;93(12):1953-1963 Cytoreductive Therapy • In addition to patients with high risk of thrombosis (>60 years of age and/or prior history of thrombosis) cytoreductive therapy can be considered in: – Extreme thrombocytosis with platelet count ≥1500x109/L – Progressive leukocytosis ≥25x109/L – Symptomatic splenomegaly – Severe disease-related symptoms – Intolerance to phlebotomy, especially in patients with compromised cardiac function, inability to comply with phlebotomy requirements, or poor venous access Treatment Algorithm Suggested by the Canadian MPN group Risk Stratification Low-risk Age <60 years and no history of thrombosis High-risk Age >60 years and/or prior thrombosis 1. Cardiovascular risk factors modifications to prevent thrombotic complications 2. Low-dose Aspirin to reduce risk of cardiovascular events 3. Phlebotomy to control erythrocytosis by maintaining hematocrit <45% • Progressively increasing leukocyte and/or platelet count • Enlarging spleen • Uncontrolled disease-related symptoms • Poorly tolerated phlebotomy *If hydroxyurea and/or IFN-α-resistant/intolerant **If not used front-line Cytoreduction Front-line • Hydroxyurea • IFN-α Second-line* • Hydroxyurea or IFN-α** • Ruxolitinib • Busulfan, anagrelide, participation in clinical trials Hydroxyurea: Efficacy in Preventing Thrombosis in PV Patients Investigator PVSG 081 Najean et al2 Kiladjian et al3 Number, Follow-up Intervention Comparator Thrombosis Rates 51 patients 15.2 years HU (prospective) Phlebotomy (134 historical controls) HU: 9.8%* Phlebotomy: 32.8%* 292 pts (<65 yrs) 7 years HU (randomized) Piprobroman No significant difference 285 pts 16 yrs HU (randomized) Piprobroman No significant difference *On study events; all events, first 378 weeks—13.7% vs. 38.1% HU: hydroxyurea; PVSG: Polycythemia Vera Study Group 1. Fruchtman SM, et al. Semin Hematol. 1997;34:17-23. 2. Najean Y, et al. Blood. 1997; 90:3370-3377. 3. Kiladjian JJ, et al. J Clin Oncol. 2011;29:3907-3913. MPN Group Positioning on HU in PV • Based on the perceived risk-benefit ratio, HU is widely used for the treatment of PV in Canada and is usually well-tolerated – The starting dose is 500 mg/day, with dose increases until the desired response is obtained. – When selecting an appropriate dose of HU, the clinician should consider: • The extent of myeloproliferation (higher doses in cases of leukocytosis, thrombocytosis, and splenomegaly) • Symptom burden • The patient’s ability to tolerate higher doses – Female patients should be advised that HU is contraindicated in pregnancy and, therefore, appropriate contraceptive precautions should be taken • Although not a common problem in PV, the development of HU resistance or intolerance needs to be further examined, especially with the availability of other treatment options Resistance/Intolerance to Hydroxyurea in Polycythemia Veraa Any of the following European LeukemiaNet (ELN) definitions 1. Need for phlebotomy to keep HCT < 45% 2. Uncontrolled myeloproliferation i.e. platelet count >400x109/L AND white blood cell count >10x109/L 3. Failure to reduce massive splenomegalyb by more than 50% as measured by palpation, OR failure to completely relieve symptoms related to splenomegaly 4. Absolute neutrophil count <1.0x109/L OR platelet count <100x109/L or haemoglobin <100 g/L at the lowest dose of hydroxycarbamide required to achieve a complete or partial clinico-haematological responsec 5. Presence of leg ulcers or other unacceptable hydroxycarbamide-related nonhaematological toxicities, such as mucocutaneous manifestations, gastrointestinal symptoms, pneumonitis or fever at any dose of hydroxycarbamide aAfter 3 months of at least 2 g/day of Hydroxyurea extending by more than 10 cm from the costal margin cComplete response was defined as: haematocrit <45% without phlebotomy, platelet count 400 x109/L, white blood cell count 10 x109 /L, and no disease related symptoms. Partial response was defined as: haematocrit <45% without phlebotomy, or response in three or more of the other criteria bOrgan Adapted from Barosi G, et al. Br J Haematol. 2010;148(6):961-963. Occurrence and Consequences of HU Resistance/Intolerance • A survey of 3,411 MPN patients treated with HU found a 5% incidence of significant non-hematologic side effects1 – GI or cutaneous problems accounting for 90% of events • HU resistance seems to be associated with: • Shorter survival (median 5.2 years compared to >20 years for non-resistant patients) • Higher risk of transformation to PPV-MF or AML (HR,6.8; 95% CI, 3.0%-15.4%; P <0.001).2 • HU has limited efficacy in relieving some PV-related symptoms, such as aquagenic pruritus.3 1. 2. 3. Antonioli E, et al. Am J Hematol. 2012;87(5):552-554. Alvarez-Larrán A, et al. Blood. 2012 ;119(6):1363-1369 Saini KS, et al. Eur J Clin Invest. 2010;40(9):828-834. Resistance to Hydroxyurea and Outcomes in PV Effect of Resistance to HU on Survival Effect of Resistance to HU on Disease Transformation (MF & AML) 1.0 1.0 0.8 Incidence Probability 0.8 0.6 0.4 0.2 0.0 Resistance Non resistance 5 10 0.4 0.2 Resistance Non resistance 0 0.6 15 20 25 Years 0.0 0 5 10 15 20 25 Years – Resistance to hydroxyurea was associated with higher risk of: • Death (HR, 5.6; 95% CI, 2.7%-11.9%; P < .001) • Transformation to AML or myelofibrosis (HR,6.8; 95% CI, 3.0%-15.4%; P < .001) 261 PV patients with a median follow-up of 7.2 years MF:myelofibrosis; AML: acute myeloid leukemia; HU: hydroxyurea Alvarez-Larrán A, et al. Blood. 2012 ;119(6):1363-1369. MED/JAKp/0001 Hydroxyurea as Mutagen: Myths vs. Scientific Data • A potential hazard in using HU is a mutagenesis as a consequence of the role of ribonucleotide reductase in DNA repair • Conflicting evidence due to the inherent risk of leukemic progression in PV even when untreated • The ELN guidelines state that HU should be used with caution in young patients (i.e., age <40 years)1 • The use of HU in a non-malignant blood disorder, sickle cell disease in children, does not increase the risk of transformation to MDS/AML2 1. Barbui T, et al. J Clin Oncol. 2011;29(6):761-770 2. Schultz WH, Ware RE. Am J Hematol. 2003;74(4):249-253148(6):961-963. Hydroxyurea: Risk of Transformation to AML/MDS Investigator PVSG 081 Finazzi et al2 Kiladjian et al3 Tefferi et al4 Number, Follow-up Intervention Comparator AML/MDS 51 patients 15.2 years HU (prospective) Phlebotomy (134 historical controls) HU: 6% vs. Phleb: 1.5%* (NS) (9.8% all event) 1638 pts 2.8 yrs (4,393 pt-yrs) Observational - No association with single-agent HU 285 pts 16 yrs HU (randomized) PIP 10, 15, 20 yrs HU: 6.6, 16.5, 24.2% PIP: 13.1, 34.1, 52.1% 1,545 pts 6.9 yrs Retrospective No association with single-agent HU *On study-event, 795 weeks AML: acute myeloid leukemia; HU, hydroxyurea; MDS: myelodysplastic syndromes; NS: non-significant; PIP: piprobroman; PVSG: Polycythemia Vera Study Group 1. 2. 3. 4. Fruchtman SM, et al. Semin Hematol. 1997;34:17-23. Finazzi G, et al, Blood. 2005;105:2664-2670. Kiladjian JJ, et al. J Clin Oncol. 2011;29:3907-3913. Tefferi A, et al. Leukemia. 2013;27:1874-1881. Interferon • Widely used in some European jurisdictions. In Canada, the coverage by provincial reimbursement plans for primary treatment of PV varies between provinces • May be considered first-line therapy, particularly in younger patients • The dose should be titrated individually based on efficacy and toxicity. • Currently no firm conclusion can be made on the superiority of INF over HU and its effects on thrombosis and survival Benefits • The absence of leukemogenic risk • Better disease control ( in JAK2 allele burden) • Improvement in symptoms, including pruritus Disadvantages • Side effects, including autoimmune disorders, flu-like manifestations, depression, heart and ocular disease, lead to permanent discontinuation in ~25% of patients Ongoing randomized trial comparing HU with interferon will be critical in defining the future role of IFN in management of PV patients (DALIAH trial; NCT01387763) 1. 2. Kiladjian JJ, et al. Blood. 2008;112(8):3065-3072. Quintas-Cardama A, et al. J Clin Oncol. 2009;27(32):5418-5424. Other Therapies Busulfan • Safe for short-term use in the elderly population, where the recognized risk of increased AML transformation with prolonged use may not be clinically relevant1 Anagrelide • Use restricted to patients in whom decreasing the platelet count causes ongoing symptoms and HU is ineffective or not tolerated.2 1. 2. Shvidel L, et al. Leukemia. 2007;21(9):2071-2072. Anagrelide Study Group. Am J Med. 1992;92(1):69-76 Ruxolitinib • Emerging data (RESPONSE trial) supports its use in PV • Based on this, MPN group recommends ruxolitinib as a second line therapy in hydroxyurea-resistant/intolerant patients • Undergoing Health Canada approval process • It is being studied in other patient populations not included in the RESPONSE trial • Health Canada label and access / reimbursement will have significant impact on its use in PV Novel Investigational Approaches for PV Other JAK inhibitors • Several have been investigated in PV, some of which have been discontinued from further development due to either toxicity or lack of efficacy (fedratinib, momelotinib, lastarutinib, XL-019) Histone Deacetylase Inhibitors (HDACi) • Givinostat • Vorinostat Combination Therapy Key Topics • Diagnostic Approaches • Current and proposed WHO criteria for diagnosis of PV • • • • Prognosis and Risk Assessment Goals of Therapy Therapeutic Approaches Specific Situations Specific Situations Splanchnic vein thrombosis (SVT) • Strongly associated with MPN; patients with unexplained SVT should undergo JAK2 V617F testing • Medical treatment of SVT includes LMWH followed by lifelong oral anticoagulation Perioperative thrombosis • Perioperative optimization of cytoreductive treatment for adequate control of Hct and platelet count is essential • In addition, DVT prophylaxis is recommended, especially in high-risk surgery • Aspirin® should be discontinued one week prior to elective interventions, if the patient’s cardiovascular status permits Pregnancy • Rare, due to advanced age of the majority of PV patients • Recommendations are based mostly on expert opinion and case series. These include: – Tight Hct control with phlebotomy and low-dose Aspirin® throughout the pregnancy, as well as LMWH prophylaxis for six weeks post-partum is recommended – Uterine artery Doppler examinations at 20 and 24 weeks to obtain an assessment of placental function are recommended – Interferon for Hct and platelet count control in patients with previous thrombosis or pregnancy complications as these patients are considered at a higher risk – Teratogenic drugs, such as HU or anagrelide, should be stopped prior to conception, with a three- to six-month washout period Robinson S, et al. Haematologica. 2005;90(11):1477-83. Griesshammer M, et al.. Blood Rev. 2008;22(5):235-45. Transformation of the Disease Post-PV MF • MF evolution is difficult to foresee, although leukocyte count >15x 109/L and allele burden >50% predicted a higher risk1,2 • The diagnosis is based on International Working Group for Myelofibrosis Research and Treatment (IWG MRT) criteria3 • PPV-MF is managed as primary MF tailoring treatment to anemia, splenomegaly, and constitutional symptoms • Following progression of PV to PPV-MF, survival is predicted using IPSS4 at diagnosis and DIPSS5 at the follow-up assessments, although these risk scores were not specifically validated in PPV-MF Post-PV AML • An aggressive disease with very poor outcomes • Intensive chemotherapy has a limited role in management unless further consolidated by allogeneic transplant6 • Hypomethylating agents and/or experimental therapies should be considered7 1. 2. 3. 4. Passamonti F, et al. Leukemia. 2010;24(9):1574-1579 Passamonti F, et al. Blood. 2008;111(7):3383-3387 Barosi G, et al. Leukemia. 2008;22(2):437-438. Cervantes F, et al. Blood. 2009;113(13):2895-2901. 5. Passamonti F, et al. Blood. 2010;115(9):1703-1708. 6. Kennedy JA, et al. Blood. 2013;121(14):2725-33. 7. Passamonti F, et al. Cancer. 2005;104(5):1032-1036 Summary • It is important that PV patients are appropriately managed and followed on a regular basis – Therapy should be individualized in every patient and adjusted based on disease burden, as well as patient individual needs and preferences • Shared-care models between centers with MPN expertise and community healthcare providers are being explored in Canada • These models provide access to expert centers while routine clinical care is provided in the community