Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
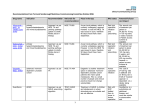
Primary Care Clinical Effectiveness Bulletin July 2011 Edition no. 7 Welcome to your South West London-wide digest of information focusing on primary care and public health evidence, guidelines and new research with the aim of informing and enabling best practice. The information is collated each month from National Institute of Health & Clinical Excellence (NICE), NHS Evidence (formerly National Library for Health), Scottish Intercollegiate Guidelines (SIGN), and SW London Effective Commissioning Initiative (ECI). Also included is PRODIGY, a clinical question answering database incorporating Clinical Knowledge Summaries, a source of evidence-based information and practical 'know how' about the common conditions managed in primary care. The bulletin contains hyperlinks to guidance – simply control + click to follow links to relevant websites where the complete document(s) are available for reading and/or downloading. CONTENTS 1. Clinical Guidelines & Care Pathways SIGN Guidance on management of Asthma NICE guideline on peritoneal dialysis NICE guideline on stable angina PRODIGY – New and updated topics for July 2011 2. NICE TAs, IPGs and MTGs Technology appraisals: Multiple Myeloma Macular oedema Myocardial infarction Epilepsy Interventional Procedure Guidance Medical Technology Guidance 3. SW London Effective Commissioning Initiative This month’s example criteria - Bariatric Surgery 4. Other useful information ‘Eyes on Evidence’ NICE 'do not do' recommendations – featuring Heart Failure Ways of influencing the work of NICE – including consultations NICE News – recent news items SW London Primary Care Clinical Effectiveness Bulletin 7th Edition Page 1 of 9 1. Clinical Guidelines and Care Pathways British Guideline on the Management of Asthma- an update (SIGN Guideline 101) (Relevant to primary & secondary acute services) The 2011 revisions include updates to monitoring asthma and pharmacological management, and a new section on asthma in adolescents. The timescale of the literature search for each section is given in Annex 1. It is hoped that this asthma guideline continues to serve as a basis for high quality management of both acute and chronic asthma and a stimulus for research into areas of management for which there is little evidence. Sections of the guideline will continue to be updated on the BTS and SIGN websites on an annual basis Peritoneal dialysis (NICE CG125) (Relevant to primary & secondary acute services) The guideline advises doctors and nurses to offer everyone with kidney failure (stage 5 chronic kidney disease) balanced and accurate information about their dialysis options. This includes people who have presented late or have had to start dialysis treatment urgently. Recommendations include consideration of the following, when discussing the options with their patients: The patient's or carer's ability to manage the treatment by themselves; How their choice of treatment would fit around their daily lives; Which settings they would prefer to receive treatment in; How far they live from their nearest centre and whether they would prefer to have a dialysis connection in their arm or abdomen. Healthcare professionals should also fully explain the risks, benefits and requirements of the options and how their choice may affect future treatments or outcomes. NB Please ctrl + click here to access the further details in the NICE Quick Reference Guide on peritoneal dialysis, from which the Care Pathway overleaf is taken. SW London Primary Care Clinical Effectiveness Bulletin 7th Edition Page 2 of 9 SW London Primary Care Clinical Effectiveness Bulletin 7th Edition Page 3 of 9 SW London Primary Care Clinical Effectiveness Bulletin 7th Edition Page 4 of 9 Stable angina (NICE CG126) (Relevant to primary and secondary care) NICE recommend the initial management of people diagnosed with stable angina should be optimal drug treatment, rather than revascularisation procedures, to provide immediate symptom relief and to prevent future attacks of angina. Further recommendations include: The optimal drug treatment should include one or two anti-anginal drugs. Additional drugs should also be offered for secondary prevention treatment, which aims to lower the risk of having a heart attack or stroke. If a person does not respond to drug treatment, they should be offered one of two techniques for revascularisation to help increase the flow of blood to the heart and to relieve symptoms. Imaging tests should be offered to determine whether revascularisation is necessary, and if so, which revascularisation procedure is best for the patient. Either coronary artery bypass surgery (CABG) or percutaneous coronary intervention (PCI) should be used where revascularisation is necessary. Healthcare professionals should consider which of these procedures is most appropriate considering the risks and benefits of each and taking into account other medical conditions, such as diabetes, age, and the severity of symptoms. A team of specialist healthcare professionals should meet regularly to discuss the risks and benefits of revascularisation and drug treatment for particular patients. NB ctrl + click here to access the care pathway and further details in the NICE Quick Reference Guide. (HINT: to view in landscape, click on ‘rotate clockwise’ icon in Adobe Acrobat’). PRODIGY (formerly CKS) is a reliable source of evidence-based information and practical 'know how' about the common conditions managed in primary care. See new and updated topics for July 2011 2. NICE TAs, IPGs, and Medical Technology Guidance Technology Appraisals Multiple myeloma (first line) - bortezomib and thalidomide (TA228) (Relevant to secondary acute services) Thalidomide (Thalidomide Celgene, Celgene) in combination with an alkylating agent and a corticosteroid is recommended as an option for the first-line treatment of multiple myeloma in people for whom high-dose chemotherapy with stem cell transplantation is considered inappropriate. Bortezomib (Velcade, Janssen) is also recommended under these circumstances, if the person is unable to tolerate or has contraindications to thalidomide. Macular oedema (retinal vein occlusion) - dexamethasone (TA229) (Relevant to secondary acute services) NICE has recommended dexamethasone (Ozurdex, Allergan) intravitreal implant, for the treatment of macular oedema following central retinal vein occlusion (CRVO). The guidance also recommends dexamethasone following branch retinal vein occlusion (BRVO) when: Treatment with laser photocoagulation has not been beneficial, or Treatment with laser photocoagulation is not considered suitable because of the extent of macular haemorrhage. Myocardial infarction (persistent ST-segment elevation) - bivalirudin (TA230) (Relevant to secondary acute services) SW London Primary Care Clinical Effectiveness Bulletin 7th Edition Page 5 of 9 Bivalirudin (Angiox, The Medicines Company) in combination with aspirin and clopidogrel is recommended for the treatment of adults with ST-segment-elevation myocardial infarction (STEMI) undergoing primary percutaneous coronary intervention. Epilepsy (partial) - retigabine (adjuvant) (TA232) (Relevant to secondary acute services) Retigabine is recommended as an option for the adjunctive treatment of partial onset seizures with or without secondary generalisation in adults aged 18 years and older with epilepsy, only when previous treatment with carbamazepine, clobazam, gabapentin, lamotrigine, levetiracetam, oxcarbazepine, sodium valproate and topiramate has not provided an adequate response, or has not been tolerated. Depression - agomelatine (terminated appraisal) (TA231) NICE is unable to recommend the use in the NHS of agomelatine for the treatment of major depressive episodes because no evidence submission was received from the manufacturer or sponsor of the technology. Interventional Procedures - all mainly relevant to secondary acute care: Key: Normal arrangement Evidence concerning both safety and efficacy of this procedure is good enough to apply normal consent, audit and clinical governance arrangements plus any additional recommendations, for example, on training, service delivery or data collection. Special arrangement Some concerns around the safety and/or efficacy of this procedure mean that special arrangements should be used: notify clinical governance leads, ensure patients understand the uncertainties referred to in the guidance, and audit and review clinical outcomes of all patients having the procedure plus any additional recommendations, for example, on training, service delivery or data collection. Other (see guidance) Due to concerns around safety and/or efficacy, the guidance recommends a combination of normal and special arrangements. Research only Use only in the context of a formal research protocol. Do not use The procedure should not be used in the National Health Service (NHS) Endoscopic radical inguinal lymphadenectomy (IPG398) Special arrangements Percutaneous endoscopic catheter laser balloon pulmonary vein isolation for atrial fibrillation (IPG399) Special arrangements Thoracoscopic exclusion of the left atrial appendage in atrial fibrillation (with or without other cardiac surgery) for the prevention of thromboembolism (IPG400) Other (see guidance) Selective internal radiation therapy for non-resectable colorectal metastases in the liver (IPG401) Special arrangements Percutaneous cryotherapy for renal tumours (IPG402) Normal arrangements SW London Primary Care Clinical Effectiveness Bulletin 7th Edition Page 6 of 9 Open femoro-acetabular surgery for hip impingement syndrome (IPG403) Normal arrangements Endoluminal gastroplication for gastro-oesophageal reflux disease (IPG404) Special arrangements Medical Technologies Guidance (relevant to secondary care) MTG5 MIST Therapy system for the promotion of wound healing in chronic and acute wounds MTG6 Ambulight photodynamic therapy for the treatment of non-melanoma skin cancer 3. South West London Effective Commissioning Initiative (ECI) A good example of the use of scientific evidence in the commissioning of local health services is the SW London Effective Commissioning Initiative (ECI), which is driven by the need to ensure that NHS funded treatments are effective and evidence-based and provide value for money, and that access to them is equitable. These criteria have been devised by local clinicians under the aegis of the South West London Public Health Network, and have been approved by the Boards of all five SW London PCTs and four local Acute Trusts. The following set of patient criteria for bariatric surgery has been taken directly from the ECI document: (see next page) SW London Primary Care Clinical Effectiveness Bulletin 7th Edition Page 7 of 9 Bariatric surgery PCTs will fund bariatric surgery for morbidly obese patients aged 20-65 who meet all of the criteria within one of the following groups: Group 1 Patients with a BMI>50 kg/m2; OR Group 2 Morbidly obese patients with a BMI >35 kg/m2 and with a significant obesity-related comorbidity that could be improved if they lost weight; AND Have failed to maintain a clinically significant weight loss for at least 6 months (at least 5% of their initial weight); AND Have received a minimum of 6 months obesity management in line with local weight management pathways which includes a multi-component weight management programme which includes support to change behaviour, increase physical activity, improve eating behaviour and diet quality and reduce energy intake and three months of anti-obesity medication. ALL patients must be fit for surgery and motivated to follow an intensive weight management programme after surgery. This is one of the new surgical procedures agreed and added to the ECI document from July 2011. For further information on the Effective Commissioning Initiative please e-mail Dr Josephine Ruwende, Consultant in PH Medicine, [email protected] 4. Other Useful Information ’Eyes on Evidence’ (NHS Evidence) ‘Eyes on Evidence’ is a newsletter which covers major new evidence as it emerges, with an explanation about what it means for current practice. This is a second chance to view the Eyes on Evidence July 2011 issue. (Ctrl+Click on the heading of this section to access all back issues.) NICE 'do not do' recommendations During the process of guidance development NICE often identify clinical practices that they recommend should be discontinued completely or should not be used routinely due to evidence that the practice is not on balance beneficial or a lack of evidence to support its continued use. These type of recommendations, since 2007, have been pulled together into the 'do not do' recommendations on the NICE website. SW London Primary Care Clinical Effectiveness Bulletin 7th Edition Page 8 of 9 This month’s example is: Management of heart failure Ways of influencing the work of NICE NICE tries to be open and transparent in the way it develops its guidance, and there are a number of ways you can get involved. Details of all NICE consultations can be accessed here. NICE News The following is a list of recent news items (not exhaustive) from the NICE website: NICE COPD quality standard complements government strategy on respiratory disease The NICE quality standard on chronic obstructive pulmonary disease (COPD) will be valuable in improving quality of care and will help the government achieve the aims of its strategy to improve outcomes for people with respiratory disease. Draft guidance launched on new surgical treatment for severe asthma A treatment for severe asthma that applies heat to the walls of the airway could reduce symptoms and improve quality of life, says draft guidance from NICE. More investment needed in gathering evidence on effective behaviour change, says Lords committee The Government must invest in gathering more evidence about what measures work to influence population behaviour change, according to a report by the House of Lords Science and Technology Sub-Committee, published today. Editorial team As always your feedback on the usefulness of this bulletin would be much appreciated. Dr. Usman Khan, Richmond Borough Team, [email protected] Tracy Steadman, Croydon Borough Team, [email protected] Alastair Johnston, Wandsworth Borough Team, [email protected] Livia Royle, Kingston Borough Team, [email protected] Jacqueline Lindo, Sutton & Merton Borough Team, [email protected] SW London Primary Care Clinical Effectiveness Bulletin 7th Edition Page 9 of 9