Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
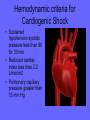
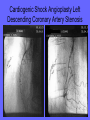
Nursing Care of the Adult (or anyone) experiencing shock Donna Roberson, PhD, APRN, BC Sharon Cherry,MPH,CNE Assistant Lecturer Four Classes of Shock as proposed by Dr. Alfred Blalock in 1934 • • • • Hypovolemic Vasogenic (Septic) Cardiogenic Neurogenic • Hypovolemic most common type resulting from a loss of circulating blood volume • Hallmark Clinical Indicators of shock are hypotension, tachycardia, decreased urine output and altered mental status What is shock? • Syndrome of low blood flow and/or abnormal blood flow patterns • Results in imbalance between oxygen and nutrient delivery and consumption on the cellular level • Five types – Low blood flow – Mal-distribution of flow Low Blood Flow Shock • Hypovolemic • Cardiogenic Maldistribution of Blood Flow • Septic • Neurogenic • Anaphylactic Shock • Key factor in any type of Shock is inadequate tissue perfusion • Adequate fluid replacement in shock victims should be indicated by urine outputs of 0.5 to 1ml/kg/hour • Watch liver failure for increasing acidosis when LR fluids are utilized. The liver may not be able to convert lactate to bicarbonate thus increasing lactic acidosis Clicker Question • Prepare Clickers Stages of Shock • Initial – May not have signs and symptoms – Lactic acid accumulates due to anaerobic metabolism, liver cannot excrete (no oxygen) • Compensatory – Neural, hormonal and biochemical mechanisms – Signs and symptoms seen – Reversible stage with treatment Compensatory Stage of Shock • • • • Increased Heart Rate Slightly decreased Blood Pressure Pale cool skin Increased Blood Glucose Second Stage of Shock • Progressive stage – Compensatory mechanisms fail – Third spacing seen – to the extreme – Without aggressive treatment, MODS • Respiratory – increased work, crackles, tachypneic • Cardiac – output falls, ischemia (distal first), dysrrhythmias, MI, complete failure Refractory Stage Third stage can be irreversible • Profound Hypotension and Hypoxemia • Accumulation of waste products throughout system • Cerebral ischemia occurs • Total, multiple organ failure • Recovery unlikely Hypovolemic Shock • Medical Stressors leading to Hypovolemic Shock • Hemorrhage • Burns • Severe vomiting and diarrhea • Peritonitis • Nursing Interventions • Initiate Intravenous therapy with NS or Lactated Ringers • Be prepared to administer Blood products PRBC’s and Platelets • Prepare patient for Surgery Burns can lead to Hypovolemic Shock Hypovolemic Shock • Blood Replacement • Crystalloids eg, 0.9% Saline or Ringers Lactate • Colloids eg, Albumin • Positive indicators urine output > 0.5 to 1mL/kg/hr, heart rate and mental status WNL Hypovolemic Shock • Patient has bleeding in lung • Knife removed in surgery Hypovolemic Shock • Loss of circulating vascular volume • Compounding problem – Decreased circulating volume – decreased venous return – decreased stroke volume – decreased cardiac output – decreased oxygen and nutrients to cells – decreased tissue perfusion – impaired metabolism Hypovolemic Shock • GSW to chest • Hemothorax • Note bleeding and collapsed lung Hypovolemic Shock • This young women was in a high speed collision • Stop sign impaled into abdomen • Patient survived with removal of stop sign and right colon Clicker Question Hypovolemic Shock • GSW to chest • Hemothorax • Note bleeding and collapsed lung Tissue Perfusion altered • Children playing with a machete • Patient taken to OR • Do you see the possibilities of more that one type of shock • Patient survived Open Chest CPR Patient Died in the Emergency Department Blount Abdominal Trauma • Bleeding of liver and laceration of liver is noted on the right side of this CT scan • Emergent surgery • What type of shock is this patient at risk for? • What nursing interventions are needed prior to surgery? TENSION PNEUMOTHORAX • Chest Trauma • High speed air bag deployed • Pt with low BP and Sats of 91% on 100% nonrebreather bag • Combative and agitated • Can lead to Cardiogenic Shock of a noncoronary nature Hemodynamic criteria for Cardiogenic Shock • Sustained hypotension systolic pressure less than 90 for 30 min • Reduced cardiac index less than 2.2 L/min/m2 • Pulmonary capillary pressure greater than 15 mm Hg Cardiogenic Shock: Patient with enlarged heart (echocardiogram) • Myocardial Infarction • End-stage Heart Failure • Cardiac Tamponade • Pulmonary Embolism • Cardiomyopathy • Dysrhythmias Clicker Question Cardiogenic Shock from Myocardial Ischemia Cardiogenic shock: EKG Presentation note ST segment elevation This was a result of Pericarditis and pericardial tamonade Clicker Question Septic Shock • Systemic inflammatory response to infection (usually bacterial) that has moved into the blood stream • High mortality rate • Bacteria release endotoxins • Systemic Inflammatory Response Syndrome (SIRS) Patients at risk for Sepsis • Immunocomprised ( AIDS, Cancer, Alcoholism, Diabetes) • Invasive procedures • Indwelling medical devices • Increased number of resistant organisms • Increased older population Septic Shock • Medical Stressors leading to Septic shock • Blood Stream Rank 1st • Lungs 2nd • Urinary tract infections 3rd • Gram Negative Organisms Most common cause of septic shock • eg,pseudomonas, acetobacter, E coli, Salmonella • Gram Positive Organisms • Fluid rescuitation with CVP of 15 is adequate • Antimicrobial agents • Inotropic agents • Vasopressors • Watch for bleeding abnormalities decreased platelets • Assess for DIC Other Gram Negative Bacteria • There are many groups of Gram-Negative bacteria such as Cyanobacteria, Spirochaetes, Green-Sulphur and Green Non-Sulphur Bacteria and Proteobacteria etc. Out of which, proteobacteria is one of the major group of known Gram-Negative bacteria (it includes bacteria like E-coli, Salmonella, Pseudomonas, Moraxella, Helicobacter, Stenotrophomonas, Legionella, Acetic Acid Bacteria etc.). Systemic Inflammatory Response Syndrome (SIRS) in response to Sepsis • Temperature greater than 38 or less than 36 • Heart rate greater than 90 • Respiratory rate greater than 30 • PaCO2 less than 32 • WBC count greater than 12000 or less than 4000 or greater than 10% immature bands Multiple organ dysfunction syndrome in response to Sepsis • • • • • • • Cardiovascular Hypotension Respiratory Hypoxemia Renal Increased Creatinine Hematologic Thrombocytopenia Metabolic lactic acidemia Neurologic Altered LOC Hepatic elevated liver function tests • Septic shock – 6-10 liters of crystalloids, 2-4 liters of colloids – Invasive monitoring (ICU patient) – Vasopressors and inotropics added if fluid fails – Ventilator – ANTIBIOTICS – broad spectrum until cultures back, then specific agents – Xigris – administered over 96 hours, boosts activated protein C (unknown action – possibly anti-inflammatory) Clicker question Specifics to Type • Cardiogenic – Diagnostic tests (caths) and supportive pumps (IABP or VAD) – Medications – diuretics, ACEI, Beta-blockers, nitrates, (+) inotropes Cardiogenic Shock Angioplasty Left Descending Coronary Artery Stenosis Neurogenic Shock • Medical Stressors leading to Neurogenic shock • • • • Spinal Cord injury Severe Pain Epidural Block Spinal Anesthetics • Treat hypotension and bradycardia • Administer medications as ordered Ephedrine and possible need for Vaspressin if patient has used ACE inhibitors • Keep HOB elevated 30 after spinal or epidural anesthesia • Immobilize spine with injury • Lovenox needed during period of inactivity and SCD’s Neurogenic Shock • Occurs after spinal cord injury at T5 or above • Massive vasodilation without sympathetic nervous system compensation (ex. SCI) • Pooling with bradycardia and hypotension • Also may have hypothalmic dsyfunction – Temperature deregulated • poikilothermia Neurogenic Shock • Usually begins within 30 minutes of injury and can last weeks • Also caused by spinal anesthesia and BZDs • Diagnosed based on cause and VS • Treatment Distributive Shock or Neurogenic Shock C-5 Burst Fracture Before and after repair Distributive Shock (Neurogenic Shock) • Cervical Spine disk 2 fracture • Hangman Fracture from look of a hanging • Caused by fall or MVA • Type of Shock nurse would assess for? • Neurogenic shock – Stabilize spine – Support hypotension – volume, neosynephrine (alpha adrenergic agonist) – Keep warm – Methylprednisolone (Solu-medrol) prevents secondary cord injury from inflammatory mediators Clicker question Anaphylactic Shock • Medical Stressors leading to Anaphylactic shock • Insect bites • Vaccines • Adverse reactions to medications or foods • Intravenous Epinephrine • Inhalation bronchodilators • Colloidal fluid replacement eg, Albumin • Benadryl • Corticosteroids • H2 blockers eg, Tagamet • Assess for Respiratory failure Anaphylactic Shock • Medical Stressors leading to Anaphylactic shock • Insect bites • Vaccines • Adverse reactions to medications or foods • Intravenous Epinephrine • Inhalation bronchodilators • Colloidal fluid replacement eg, Albumin • Benadryl • Corticosteroids • H2 blockers eg, Tagamet • Assess for Respiratory failure Anaphylactic Shock • Life-threatening hypersensitivity to a substance (bee stings, medications, food) • Massive vasodilation, vasoactive mediators released and increased capillary membrane permeability • Laryngeal edema, hypotension, wheezing/stridor, skin changes – death! • c/o dizziness, chest pain, difficulty swallowing or breathing, anxiety Clicker Question • Prepare Clickers Presentation • Young, healthy people can compensate up to a point • HR elevated, narrowed pulse pressure, hypotensive • Tachypneic, decreased UO, increased specific gravity, pallor, cool/clammy • Confused, anxious Presentation • Hypotension despite fluid support • Cardiac dysfunction, respiratory failure, oliguria, confusion, GI bleeds • Systolic BP <90 or more than 40mmHg below baseline (inadequate for perfusion of major organs) • One or more organs fail – multiple organ dysfunction syndrome (MODS) Typical Interventions (collaborative) • Oxygen/airway (have intubation tray ready) • Stabilize spine (as indicated) • IV – at least 2 #18 or bigger bore – Prepare to give crytalloids like NS or LR • Stop obvious bleeding • Assess for worsening cardiac and respiratory function Collaborative Management • Requires immediate action by nurse (or family, or rescue, etc.) • Protocols are established in areas that see this type of shock • Usually administer epinephrine (subq, IV, IM). Benadryl (IV, IM, PO), steroids also given • Anti-venom for insect stings • IV support and monitoring • Anaphylactic shock – Prevention – Epinephrine #1, Benadryl, Tagamet – Airway preservation – Nebulizers with Alupent or Albuterol – Fluid replacement with colloids (prevent 3rd spacing) Diagnostic Interventions • Monitor dropping hemoglobin and hematocrit, electrolytes • FAST(Focused abdominal sonographic technique) can be done at the bedside of the trauma pt • CT scans (Computed tomography scan) • EGD • Chest Radiographs • Angiography • Nuclear Medicine Scanning • ABG’s • Coagulation studies • Electrolyte Studies Treatment Interventions • Preserve and replace volume – Blood, plasma expanders, albumin – Crystalloid’s first choice of fluid for resuscitation (Normal Saline or Lactated Ringers Diagnostics • Cardiac enzymes – troponin levels • EKG, Chest Xray and echocardiogram • See page 1800! Treatment • Correct underlying cause • Hypovolemic – Fluid replacement – Crystalloids – NS, LR (used for most shock) – Blood- PRBC (all if Hgb <12) and as indicated – Colloids- AKA plasma expanders • hespan (all) • Albumin – • Dextran – • Renal – acute failure, increased BUN/crt, requires hemodialysis • GI – ulcers, bleeding, paralytic ileus • Hematologic – DIC • Hepatic – liver failure, enzymes increase Clicker Question • Prepare Clickers Clicker question Clicker question • Prepare to administer vasopressives • Prepare to insert Foley and NG • Monitor and use protocols to treat dysrrhthmias • Keep warm (septic may use cooling blankets) • Daily weights – TPN after enteral feedings fail A word about positioning • Pay attention to research studies – Consider sample size, methods to measure • Most agree, positioning does not impair tissue perfusion. • Old-timers – firmly believe in Trendelenburg positioning to increase cerebral blood flow – Not used with cord injuries • Shock position– flat on back, elevate legs 12 inches (not for cord injuries), cover Clicker question • Prepare Clickers • End of Shock Lecture How can the nurse assess for Heart Failure? • Listen for Heart sounds and Lung Sounds • Assess pulses • Assess BP Heart Failure: The heart’s inability to pump enough blood through the body DRG Heart Failure • • • • • • • • • • • • DRG 127 - Substantiating Congestive Heart Failure SIGNS/SYMPTOMS/CONDITIONS Shortness of breath Fatigue with exertion Orthopnea Paroxysmal nocturnal dyspnea Tachycardia Tachypnea Pulmonary rales (fine crackles) Edema of lower extremities Jugular vein distention Gallop on cardiac auscultation Heart Failure • COMMON TREATMENT • Medical treatment includes oxygen, nitroglycerin, diuretics, vasodilators, ACE inhibitors, ARB (Angiotensin receptor blocker), hydralazine, digoxin, betablockers or anticoagulation. Patients are educated and encouraged to restrict dietary salt and fluid intake. Heart Failure • Systolic dysfunction – inability to move blood forward through the heart • Diastolic dysfunction – inability to move blood out of heart (poor right or left ventricular filling) • Physiologic state in which inadequate tissue perfusion results from cardiac dysfunction Heart Failure • TESTS • Chest x-rays may indicate presence of alveolar edema, interstitial infiltrates, pleural effusion or congestive heart failure • Echocardiogram shows left ventricle dysfunction, diastolic dysfunction or ejection fraction of <50% • Gated pool studies reveal moderate-to-severe left ventricular dysfunction or ejection fraction of <50% • Cardiac Catheterization findings reveal left ventricular dysfunction or ejection fraction of <50% Diagnostic test for Heart Failure • Chest x-rays may indicate presence of alveolar edema, interstitial infiltrates, pleural effusion or congestive heart failure • Echocardiogram shows left ventricle dysfunction, diastolic dysfunction or ejection fraction of <50% • Gated pool studies reveal moderate-to-severe left ventricular dysfunction or ejection fraction of <50% • Cardiac Catheterization findings reveal left ventricular dysfunction or ejection fraction Presentation • Tachycardia, hypotension and narrow pulse pressure • Tachypneic, adventitious breath sounds • Cyanosis, pallor, cool/clammy skin, decreased capillary refill time • Increased central venous pressures • Decreased cardiac output • Oliguria • Altered Mentation Assessment findings: The patient’s heart is weaker • Blood and fluid back up into the lungs • Fluid builds up into the feet, ankles and legs • Patients experience tiredness and SOB Nursing Care of the Adult with Cardiovascular Complications Donna W. Roberson, PhD(c), APRN, BC Anemias • Deficiency in red blood cell mass and hemoglobin content. • Deficiency occurs from – blood loss – reduced production – excessive hemolysis Manifestations • Mild (Hgb 10-14 g/dL) – – none, slight fatigue, pale mucous membranes, DOE • Moderate (Hbg 6-10g/dL) – – increased fatigue, palpitations, dyspnea, diaphoresis • Severe (Hbg <6 g/dL) – – pallor, jaundice, glossitis, tachycardia, murmurs, cardiac symptoms, HA, vertigo, decreased concentration, organomegaly, bone pain, cold intolerance, lethargy Etiology • Decreased Erythrocyte Production – Iron deficiency anemia (IDA) – Thalassemia and thalassemia trait – Pernicious anemia (vitamin B12 deficiency) – Folic acid deficiency anemia – Aplastic anemia – Anemias of leukemia/cancer – Anemia of chronic disease (ACD) • Blood Loss – trauma, hemorrhage, GI, menstrual • Increased Erythrocyte Destruction – Hemoglobin abnormalities (SSC, G6PD deficiency) – Trauma – prosthetic valve, hemodialysis and other extracorporeal circulation, autoimmune disorder, infections and toxins Morphology • Size – consider diameter of cell – RDW • Weight – how heavy the cell is – MCV • Chromicity – how pretty and red the cell is – MCH, MCHC • Normochromic, normocytic – normal color, size and weight Normal Red Blood Cell Production • Erythropoietin produced by the kidney regulates cell production. • Mature erythrocytes form from adequate – caloric intake – Iron – folic acid – vitamin B12 – erythropoietin Normal laboratory values • Reticulocyte count 0.5-2% Hgb 12-18 Hct 37-52% MCV 80-95 MCH 27-31 MCHC 32-36 RDW 11-14.5% Serum Ferritin >10 TIBC 250-420 • The normal adult requires 20 mg of iron per day to produce HgB. • About 10 mg comes from degraded HgB. • Most can absorb 1mg of iron per 10mg ingested (in duodenum) IDA • Most common anemia • Very young, poor diet, women, absorption problems (lactose intolerance, celiac sprue), cancer • *repeated blood draws (decreases recycling of iron from Hbg) • Microcytic, hypochromic Presentation • Fatigue, pallor, glossitis • Worsens as stored iron is depleted Diagnosis • History and physical • CBC with differential, serum ferritin, serum iron, TIBC, hemoccult, hemoglobin electrophoresis (peripheral smear) Thalassemia and Thalassemia Trait • Genetic disorder of decreased erythrocyte production • Common in Mediterranean ancestry, equatorial Asia and Africa • AKA Thalassemia major and minor (trait) • Microcytic, hypochromic • Thalessemia results in severe deficiencies and death Megaloblastic Anemias • Cobalamin (B12 deficiency) – dietary deficits, loss of intrinsic factor, hyperactive gut disorders • Folic Acid deficiency – Inadequate oral intake of folate-rich foods (ETOH abusers, pregnancy) – Impaired absorption • Macrocytic normochromic cells • Pernicious anemia – intrinsic factor is not secreted by the gastric mucosa –Erroneously used for all Cobalamin deficiency Anemias • prolonged use of PPI in high doses (atrophy) • Destroyed parietal cells (autoimmune) Presentation • • • • • • • Fatigue Sore tongue Anorexia, N/V Abd pain Peripheral paresthesias Confusion Death if not corrected Diagnosis • CBC with diff, peripheral smear • B12 and folate levels • Gastric exam (r/o cancer, check for atrophy) Schilling test • NPO 8-12 hrs, no B vitamins 3d before, no laxatives 1d before • Collect small urine sample • Radioactive B12 (po capsule) in radiology • May eat • RN gives 1mg B12 IM 1-2hrs after radioactive dose (saturates liver so capsule can be absorbed in sm. intestines) • 24 hour urine (lab decides if iced or not) Anemia of Chronic Disease • microcytic to normocytic and normochromic cells • chronic depletion of RBC (none for recycling) • Chronic state of over-iron utilization or bone marrow failure (cancers/chemo, infections, rheumatoid arthritis, lupus, diabetes, COPD, etc.) Aplastic Anemia • All blood components are low • Congenital (Fanconi syndrome) • Acquired – Idiopathic – Chemical exposure – Meds – Pregnancy – Radiation – Infections Care regimens – Medical and Nursing • Diet and nutrition • Based on deficiency, encourage foods high in need (tends to be the same foods for iron and folate) • Examples: spinach, liver, raisins, cast iron cooking pots, green leafy vegetables, yeast, dried beans, nuts • Absorptive disorders interfering • Educate and support restrictive diet Examples: assist in determining irritating foods - limit diary, teach label reading to avoid glutens Supplementation - IRON • Expect improved S&S 5-7d – ½ labs corrected labs in 3 weeks – normal by 2 months. – Iron stores refilled 4-6 months (if successful.) • Biggest complaint – constipation and heartburn • Normal – tarry, dark looking stools Iron • ferrous sulfate – 300 -325mg body absorbs 65mg • ferrous gluconate – 325mg body absorbs 38mg • ferrous fumarate – 325mg body absorbs 106mg • iron dextran –IV or IM monthly – use Ztrack to prevent skin staining (test dose) Cobalamin and Folic Acid • Vitamin B12 – 1000mg IM daily for 2 weeks – Then weekly until normal hematocrit – Then monthly for life • Folic acid – usually give with multivitamin since malnutrition typical root of problem – 1-5mg daily Erythropoietin • • • • • • ACD (not BM cancers) EPO, Procrit, Epogen Refrigerated Never shaken Subq at room temperature Monitor labs Preventative care • Balanced diet – particularly menstruating women • Use of COC for planned amenorrhea (also called chemical menopause) • Substance abuse counseling • Care for those with chronic illnesses or prolonged infections • Management includes nutritional counseling Protective care • Support use of supplements – problem shooting for GI c/o • Allow ventilation of concerns, offer support groups- use of the internet • Encourage routine health screens by age – new onset of anemia over age 50 presumed cancer until proven otherwise! Anemia due to blood loss • Volume replacement and PRBCs • Correct underlying cause – Pressure, cautery – COC • Chronic losses – iron, diet Hemolytic Anemia • Overdestruction of RBCs • Defects of cell causes destruction by spleen and liver (Sickle Cell) • Autoimmune disorder • Jaundice from elevated bilirubin as RBCs destroyed • In all cases, ensure renal protection from large RBC bits (ATN) Polycythemia • Overproduction of RBCs • Causes thickened blood – problems? • Blood letting, hydration, BM suppression Coagulation disorders platelets nl 150k-400k excess - thrombocytosis deficit - thrombocytopenia 10k-20k results in hemorrhage from minor trauma < 10k results in spontaneous hemorrhage Immune thrombocytopenia purpura (ITP) acute - usually children/young adults follows a viral event chronic - usually women (20-50), unknown precipitating factor Platelets coated with antibodies and destroyed as an immune response by spleen after only 1-3 days Manifestations of ITP Purpura, ecchymoses and petechiae Epistaxis Menorrhagia Hematuria GI bleeds Secondary thrombocytopenia anemias, ETOH abuse, viral infections (Mono), AIDS, heparin, Coumadin, sulfonamides, digoxin, Lasix, MSO4, Tagamet ASA and NSAIDS interfere with platelet function but not production Diagnostics and treatment CBC - H/H and plt count bleeding times prolonged in ITP treat with plt transfusion - warming increase counts by 28% expect a rise in count by 8-10k per unit given. Can recheck plt count in 15 mins. after tx Disseminated intravascular coagulation state of both clotting and hemorrhage inappropriate thrombin response causes diffuse clotting, clotting factors are consumed and the fibrinolytic system is activated. Clots are dissolved, but no clotting factors are available, therefore hemorrhage occurs. Clinical picture causes include trauma, obstetrics complications, hemolytic reactions, shock, sickle cell crisis, MI, PE, and others Skin - purpura, ecchymoses, petechiae, cyanosis of extremities, bleeding from wounds More GI- ABD distention, blood in stool and vomitus, frank hemorrhage Resp/CV – shock symptoms GU - hematuria, oliguria, renal failure CNS - confusion, coma, seizures Diagnostics PT & INR/PTT increased Plt decreased plasma fibrinogen decreased decreased clotting factors Treatment heparin used when organ function is impaired Heparin contraindicated in shock/active bleeding nursing care - promote hemostasis, tissue perfusion, manage pain, gas exchange and anxiety Heart failure • Many still call it Congestive Heart Failure (CHF) • Systolic failure -pump fails – Decreased ejection fraction (EF) – Decreased contractility – Increased afterload – cardiomyopathy • Diastolic heart failure (DHF) – ventricles fail to fill – Venous engorgement with S&S (criterion 1) – Normal EF (criterion 2) – Abnormal diastolic function (criterion 3) • Can have both! • To distinguish between SHF & DHF – must have measure of EF Treatment • Similar medications, different doses and reasons • SHF – improve inotropic function and improve remodeling of LV with Beta blockers. Digoxin still used. No use for calcium channel blockers • DHF – Beta blockers used to decrease HR, increase diastole, improve response to exercise *smaller doses than SHF DHF – improve venous congestion • Fluid and sodium restriction • Dialysis • Nitrates (nitroprusside, long acting oral agents) • Diuretics- spironolactone, loops • ACEI and ARBs DHF – increasing diastole • Beta blockers, calcium channel blockers • Digoxin only used in those with atrial fibrillation or very short term in the acute period Cardiomyopathy • Disease of the myocardium resulting in impaired function • Primary – Unknown • Secondary – Dilated, hypertrophic, or restrictive Dilated Myopathies • ETOH, cocaine, doxorubicin, genetic, HTN, idiopathic, ischemia, etc. • c/o fatigue, palpitations, SOB/DOE, cough • PE enlarged heart, decreased contractility, valve failure, arrhythmias, decreased CO • Diagnostics – Xray, EKG, cath Dilated Management • Treat underlying cause • ACEI, diuretics, anticoagulants, cardiac transplant • Teach family CPR, how to access EMS • No ETOH, limited sodium Hypertrophic Myopathies • • • • Asymmetric enlargement without dilation Genetic, stenosis or HTN cause c/o exertional dyspnea, fatigue, angina Syncope seen in those with aortic outflow obstruction • PE SVT, fib, tachy, S3 or S4 • Primary diagnostic tool – EKG with increased QRS, also may get cath Hypertrophic Management • Improve ventricular filling • Support patient/family • Relieve symptoms Restrictive Myopathies • Fibrotic changes in the myocardium prevent ventricular filling • c/o angina, syncope, fatigue, DOE *hallmark sign • PE DHF signs and symptoms • Diagnosis – EKG shows tachy at rest, CT or MRI Restrictive management • No treatment other than DHF therapies • Nursing supportive • Cardiac transplant – Recipient/donor matching based on body size, heart size and ABO type – Maximum out-of-body time 6 hours – Place recipient on cardiopulmonary bypass – Start immunosuppressives in OR • Nursing care focused on • Acute – Operative recovery – Teaching about medications and diet • Long term – Ongoing support of lifestyle changes – Monitor for rejection, lymphoma and vasculopathy Heart Blocks 1st degree AV Prolonged PR interval 2nd degree AV Type I (Wenckebach) AV node problem Lengthened PR, some P have no QRS Type II (Bundle Branch Block) His-Purkinje problem Ratios of Ps with QRS 3:1, 2:1 Poorer prognosis, requires temporary pacemaker 3rd degree AV complete No relation between P and QRS Junctional rhythm common with HR 20-40 Ventricular disturbance • PVCs – indicates electrical irritation across myocardium – Bigeminy, Trigeminy possible – Couplets lead to v-tach • Ventricular Tachycardia – run of 3 or more PVCs • Wide, aberrant QRS pattern • Rate 100-250 • Leads to v-fib if not interrupted • Ventricular fibrillation • Asystole – flat line or occasional P, assess in different leads to make sure not V-fib Treatment for AV Block • Internal pacemaker – takes the place of the SA node • Wide variety available – on demand, preset, responsive to exercise, etc. • Complications – infection, bleeding, failure to capture, failure to sense, battery failure Nursing care of pacemakers • Administer pre-pacer antibiotic • Monitor for infection – small incision anterior chest or abdomen • Reassurance – fear big problem • Teach how to assess pulse *family too • Avoid magnetic fields and electrical generators (Microwaves are safe) • Medic alert Treatment of Ventricular Dsyrhthmias • Automatic Internal Cardio-Defibrillator (AICD) also ICD • Lead inserted through subclavian vein to endocardium. • Pulse generator – upper chest or abdomen • Lead senses v-tach or v-fib, cues pulse generator • 25-joule shock delivered • Recycles and can continue to work Nursing Care • Similar to pacers • Reassurance – fear of arrest, fear ICD won’t work properly • Sexuality • Anxiety – patient and family Revascularization of the Myocardium • Treats post-MI ischemia and failed medication management of CAD • CABG, RIMA, LIMA, saphenous veins • Traditional method – Open sternum incision, bypass, heart stopped – Long leg(s) incision – Chest tubes – External pacing wires – Cordis • Requires at least 2 days ICU in specialty care unit. • Usually 24-48 hrs ventilator support • Pain management • Monitor CT drainage (2-4 CTs usual) • EKG, cardiac output, pulmonary pressures Robotics! • Minimally Invasive Direct CABG – MIDCAB for short – Used for LAD or single vessel bypass • Several, small intercostal incisions • Harvested LIMA used on heart slowed by calcium channel blockers or beta blockers Nursing Care of MIDCABG • • • • Usually 2 CTs Nitro drip Pain management No bypass used, so quicker recovery, shorter LOS • *Teaching for both centers on lifestyle changes Reduce Risk of Coronary Artery Disease and Heart Failure • Keep LDL cholesterol below 100 • Keep HDL Cholesterol above 40 in men and above 50 in women • Keep Triglycerides another fat in the blood below 150 • Keep BP 130/80 or below • Keep Blood Glucose under control • Limit alcohol intake and quit smoking • Dietary mg Foods low in saturated fats and low in salt General Care Principles • Identify patients at risk • Careful history and examination • Report early signs, prepare to act with supportive measures (IV, blood, medications, etc) • Protect and support function