Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
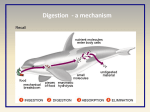
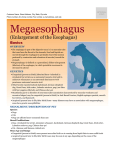
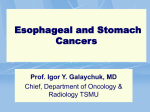
New York City College of Technology Department of Radiologic Technology & Medical Imaging By: Group #7 Group Members: Wendy Rodriguez Sae Young Park Adam Hernandez Jennifer Moreta Hardy Ward Scarla Colon Nene Bah Dharam Bhagwandas Introduction and Patient History Esophageal cancer is not common in the United States. In other areas of the world, such as Asia and parts of Africa, esophageal cancer is much more common. Esophageal cancer is among the causes of cancer related deaths worldwide as well. The management of patients with esophageal cancer is determined to a large extent by patient performance status, location of the primary cancer and stage of the disease. This case study focuses on a follow up exam of a 75 year-old woman with a history of breast cancer metastasized into her esophagus; causing for the removal and replacement of the esophagus. Ivor- Lewis esophagestomy is performed to the patient in order to remove part of the esophagus and part of the stomach. Part of the stomach and the small intestine are used to make a connection with the leftover part of the esophagus to allow swallowing and passage of food. Prior to the surgery the patient present mild pain swallowing and lower back pain. Esophageal cancer is a cancer that forms in the tissue lining of the esophagus. Cancer of the esophagus begins in the inner layer of the esophageal wall and grows outward. Esophageal cancer begins in the cells that line the esophagus. Cancer begins when normal cells change and grow uncontrollably, forming a mass called a tumor. A tumor can be benign or malignant. Esophageal cancer spreads to the wall, it can travel to the lymph nodes, blood vessels in the chest, and other nearby organs. Esophageal cancer can also spread to the lungs, liver, stomach, and other parts of the body. Anatomy The esophagus is a hollow organ that carries food and liquids from the throat to the stomach. It is part of the digestive system and is located between the trachea and the spine. The esophagus is about 11 inches long and just before entering the stomach, the esophagus passes through the diaphragm. The walls of the esophagus contain two sphincter; the upper esophageal sphincter Figure 1. Anatomy of the esophagus and the lower esophageal sphincter. The upper esophageal sphincter (UES) is a muscle that control breathing, belching, vomiting and keep food and liquids from going down the windpipe. The lower esophageal sphincter (LES) it is located where the esophagus and the stomach meets and it prevents acid and food contents from moving back up to the esophagus (Figure 1). The wall of the esophagus has several layers. These layers are important for understanding where cancers in the esophagus tend to start and how they grow. There are four layers; these layers are mucosa, submucosa, muscularis propia and adventitia. The mucosa layer subdivides into three parts. The epithelium forms the innermost lining of the esophagus and is normally made up of flat, thin cells called squamous cells and this is where most cancers of the esophagus start. The lamina propia is a thin layer of connective tissue right under the epithelium and the muscularis mucosa is a thin layer of muscle under the lamina propia. The submucosa is a layer of connective tissue below the mucosa that contains blood vessels and nerves. Muscularis propia is a muscle layer that contracts in a rhythmic way to push food along the esophagus from the throat to the stomach. The last portion is the most outermost layer of the esophagus called adventitia (Figure 2). There are two types of esophageal cancer. The two types are squamous cell carcinoma and adenocarcinoma. Squamous cell carcinoma is a type of esophageal cancer starts in squamous cells that line the esophagus. It usually develops in the upper and middle part of the esophagus. This is also called epidermoid carcinoma. Adenocarcinoma is a type that begins in the glandular tissue in the lower part of the esophagus where the esophagus produce and release fluids such as mucus. Figure 2. Muscular layers of the esophagus The stage of esophageal cancer is a standard summary of how far the cancer has spread. The most common system used to stage esophageal cancer is the TNM system. The T represents how far the primary tumor has grown in the wall and into nearby organs. The N refers to the spread to nearby lymph nodes and the M indicates if the cancer has metastasized, in other words spread to other distant organs. A risk factor is anything that can change your chance of getting any disease such as cancer. Evidently, different types of cancers have different risk factors. One of the main risk factor is age. People who tend to smoke, can increase the chance of getting esophageal cancer. People who have acid reflux, an abnormal backward flow of stomach acid into the esophagus. The stomach acid can damage the tissue of the esophagus. This may irritate part of the lower esophagus and cause Barrett esophagus over time. Early esophageal cancer may not cause symptoms, but as the tumor grows the most common symptoms that people go through are: food getting stuck in the middle of the esophagus and coming back up, pain swallowing, pain in the chest or back, weight loss and heartburn. There are several test to find and diagnose esophageal cancer. A general checkup to the doctor can be helpful finding early stages of esophageal cancer. And includes checking for lumps or anything that seems unusual. An x-ray of the chest also can be obtained to detect any abnormalities of the organs inside the thoracic cavity. A barium swallow could be more effective than a regular chest x-ray. The reason why it is because the patient drinks a liquid that contains barium that “highlights” the part examined for better visualization. Another test is called esophagoscopy. This procedure is performed to look inside the patient’s esophagus to look for abnormal areas. An esophagoscope is a thin, tube-like instrument with lens and lights and it is inserted through the mouth or nose down the throat. If the cancer is detected through these exams, patient may or may not have to go through esophagectomy. Esophagectomy is the surgical procedure of the removal of the lower portion or the entire esophagus in extreme cases, along with the most upper portion of the stomach and its surrounding lymph nodes. The stomach then is reshaped into a new esophagus and reconnected to the remaining part of the esophagus or neck. There are three types of surgical approach that can be performed for the removal of the tumor in the esophagus. The most common and frequently performed procedure for resection of the thoracic is the Ivor-Lewis’s trans-thoracic approach and the trans-hiatal approach. The Ivor-Lewis’s procedure the esophageal cancer is removed through an abdominal incision and a right thoracotomy (a surgical procedure of the Figure 3. A transthoracic esophagectomy through a right thoracotomy procedure. chest wall). Then the esophagogastric anastomosis is performed to reconnect the stomach and the remaining portion of the esophagus (Figure 3). The Trans hiatal esophagectomy is performed on the neck and abdomen at the same time. This procedure is performed without thoracotomy. First, the abdomen is opened and assessed for metastasis. The stomach is mobilized in preparation of the resection. Then, the esophageal hiatus is widened and the esophagus is mobilized and in the last phase the cervical portion of the esophagus is mobilized inferiorly and the dissection of the stomach is performed. The esophagus is resected and a stomach tube is created. The stomach is brought up in the neck and esophagogastric anastomosis is done in other words reconnection is performed (Figure 4). Figure 4. A Trans-hiatal esophagectomy procedure Various complications may occur after these surgical procedures. These complications can happen internally or right after the surgery. Internal complications may include hemorrhage, injury to the tracheobronchial tree, laryngeal nerve injury and pneumothorax. Postoperative complications include anastomotic leak, mediastinitis (infection of the mediastinum) atelectasis, pneumonia, adult respiratory distress syndrome, myocardial infarction, pericardial tamponade (blockage), hernia, obstruction, reflux esophagitis and ulceration. The most common complication is pneumothorax, pleural effusion, aspiration bronchiolitis and respiratory failure. People with esophageal cancer have several treatment options. The options are surgery, radiation therapy, chemotherapy, or a combination of these. These therapies depends on the location of the cancer, whether the cancer invaded other parts of the body, whether the cancer has spread to lymph nodes and the patient’s overall health. In some cases, radiation therapy may be used instead of invasive surgical procedure if the cancer has not spread to nearby organs. Usually chemotherapy and radiation therapy can be performed before and after the surgery. Chemotherapy and radiation may be used to shrink the tumor and make surgeries easier to perform. If the patient is too ill to have major surgery or the cancer has already spread to another site, these procedures can be used to reduce symptoms. This is called palliative therapy. A change is diet may also help to treat cancerous diseases, but there are other treatments that may be used to help the patients to swallow. These include dilating (widening) the esophagus using an endoscope, a feeding tube into the stomach, photodynamic therapy, in which special drug is injected into the tumor and is then exposed to light. This light activates the injected drug to attack the tumor. Esophageal cancer is a medical condition that can be treated and prevent if found at an early stage. It is very important to do general checkup with the doctor. Esophageal cancer can be dangerous if it is not treated. It could lead to death in some extreme cases. The best way to treat this condition is to consult with surgeons about the treatments and surgical procedures and also discuss about the short and long term outcomes and act promptly to prevent any complications. The recovery may be a long period of time, although the commitment to therapies and following doctor’s advices could be the key to return to a healthy lifestyle. Tests to Diagnose Esophageal Cancer (Illustration) Barium Swallow. The patient swallow barium liquid and it flows through the esophagus and into the stomach. Esophagoscopy. A thin, lighted tube is inserted through the mouth and into the esophagus to look for abnormal areas. References 1. Das A. Tumors of the esophagus. In: Feldman M, Friedman LS, Brandt LJ, eds. Sleisenger and Fordtran's Gastrointestinal and Liver Disease. 9th ed. Philadelphia, PA: Elsevier Saunders; 2010: chap 46. 2. National Cancer Institute: PDQ Esophageal cancer treatment. Bethesda, MD: National Cancer Institute. Date last modified 2/1/2013. Available at: http://www.cancer.gov/cancertopics/pdq/treatment/esophageal/HealthProfessional . Accessed February 4, 2013. 3. National Comprehensive Cancer Network. NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines): Esophageal and esophagogastric junction cancers. Version 2.2012. Available at http://www.nccn.org/professionals/physician_gls/pdf/esophageal.pdf. Accessed February 4, 2013. 4. Sugarbaker DJ, Jaklitsch MT, Liptay MJ: Thoracoscopic staging and surgical therapy for esophageal cancer. Chest 107 (6 Suppl): 218S-223S, 1995. 5. (n.d.). Retrieved from http://www.webmd.com/digestive-disorders/picture-of-theesophagus 6. (n.d.). Retrieved from http://www.cancer.org/Cancer/EsophagusCancer/DetailedGuide/esophaguscancer-staging 7. Baldwin, K. (n.d.). Retrieved from http://emedicine.medscape.com/article/277930-overview