Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
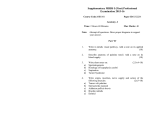
Anaesth Intensive Care 2010; 38: 946-948 Ultrasound-guided bilateral superior laryngeal nerve block to aid awake endotracheal intubation in a patient with cervical spine disease for emergency surgery S. Manikandan*, P. K. Neema†, R. C. Rathod‡ Department of Anaesthesiology, Sree Chitra Tirunal Institute for Medical Sciences and Technology, Trivandrum, Kerala, India Summary Ultrasound has been widely used to locate nerves for various nerve blocks. The potential advantages of using ultrasound imaging for nerve blocks include reduction in the amount of local anaesthetic required, improved success rate, reduced time to perform the block and reduced complication rate. We describe the successful performance of ultrasound-guided bilateral superior laryngeal nerve block to facilitate awake fibreoptic intubation in a patient presenting for emergency surgery on the cervical spine. Key Words: superior laryngeal nerve block, ultrasound, awake intubation Ultrasound can be useful to identify and assist in blocking the superior laryngeal nerves in patients with difficult neck anatomy undergoing awake fibreoptic bronchoscope (FOB) intubation. In addition, ultrasound may reduce the likelihood of accidental injection into blood vessels in this area which are particularly numerous. anaesthetise the larynx, bilateral superior laryngeal nerve (SLN) block at the level of the greater horn of hyoid (GHH) was undertaken. Due to soft tissue oedema of the neck caused by previous surgery, identification of landmarks was considered difficult. Hence, we decided to use ultrasound for identification of the laryngeal nerves. CASE HISTORY A 50-year-old male patient (weight 66 kg) underwent posterior fixation for atlantoaxial dislocation uneventfully under general anaesthesia. Two days later he developed sudden onset of weakness of both lower limbs and required emergency re-exploration. In the operating room, with appropriate monitoring, intravenous and radial artery cannulation were performed under local anaesthesia. Airway assessment showed mouthopening of less than two fingers. Considering the immobile upper cervical spine by implants and the onset of new neurological deficits, awake intubation using a flexible FOB was planned. Glycopyrrolate 0.2 mg was administered intravenously for its antisialogogue action. Topical lignocaine 10% was sprayed over the anterior aspect of his tongue. To *M.D., D.N.B., P.D.C.C., Associate Professor. †M.D., Additional Professor. ‡ M.D., Professor and Head of Department. Address for correspondence: Dr S. Manikandan, B-14, NFQ, SCTIMST, Poonthi Road, Kumarapuram, Trivandrum-695011, Kerala, India. Email: [email protected] Accepted for publication on March 28, 2010. Figure 1: The initial position of the probe insinuating the submandibular gland (1), lingual artery (2) and hypoglossal nerve (3). Anaesthesia and Intensive Care, Vol. 38, No. 5, September 2010 Case Report Figure 2: The second position of the probe insinuating the external carotid artery (1), superior laryngeal artery (2), superior laryngeal nerve (3), superior thyroid artery (4), greater horn of hyoid (5). Technique The neck area was cleaned with antiseptic solution. The head was kept in the neutral position. Ultrasound localisation was performed with the SiteRite™ 5 Ultrasound system (Bard Access Systems, Inc, Salt Lake City, UT, USA). The Site-Rite™ 5 uses a 5 to 10 MHz linear probe for identification of structures. The probe was initially placed over the submandibular triangle just below and parallel to the mandibular border and adjusted to visualise the submandibular gland. Along the lower pole of the submandibular gland arterial pulsations were identified, which is the lingual artery in the long axis plane. The lingual artery runs below the sublingual gland parallel with the hypoglossal nerve (Figure 1). The probe was moved caudally and laterally approximately 0.5 cm and adjusted to visualise the external carotid artery that can be identified as a round structure with pulsations in the short axis view (Figure 2). Pulsations of a branch arising from the external carotid artery running medially and parallel to the probe can be viewed at this plane, which is the superior thyroid artery (STA). The probe was moved slightly medially and the STA could be seen giving rise to the superior laryngeal artery (SLA) that runs parallel to the probe, wth the main artery continuing inferiorly (Figure Anaesthesia and Intensive Care, Vol. 38, No. 5, September 2010 947 Figure 3: The final position for the placement of local anaesthetic agent. 1) omohyoid, 2) external carotid artery, 3) greater horn of hyoid, 4) superior laryngeal artery, 5) superior laryngeal nerve, 6) superior thyroid artery. 3). The greater horn of the hyoid bone could also be seen as a bright structure medial to the SLA. Additional confirmation was obtained by moving the probe medially, which showed the curved bright image of the hyoid bone. The internal branch of SLN (ibSLN) runs along with the SLA, just below the level of GHH. A 22 gauge hypodermic needle was passed perpendicular to the skin at this point between the GHH and SLA. Lignocaine 2% 0.75 ml was injected after negative aspiration of blood, and the solution was seen spreading in the plane. The procedure was repeated on the other side. After a few minutes the patient had voice changes indicating the onset of the block. The FOB was introduced and the vocal cords appeared paralysed. The trachea was intubated successfully without any discomfort to the patient. DISCUSSION Techniques employed to anaesthetise the airway for awake FOB intubation include topical anaesthesia combined with bilateral SLN block or lignocaine nebulisation combined with either ‘spray-as-yougo’ topical anaesthesia or cricothyroid puncture and instillation of a local anaesthetic drug1. In a recent study, Xue et al found that with topical application 948 S. Manikandan, P. K. Neema, R. C. Rathod of either 2 or 4% lignocaine in the spray-as-yougo technique, one could successfully intubate the trachea using awake FOB. However, they noticed that 61 to 74% patients had grimace or cough response during intubation and they attributed this to inadequate anaesthesia of the airway2. They suggested that this may be due to non-uniform spread of the lignocaine and variability in the absorption of the local anaesthetic agents caused by oropharyngeal secretions. In a volunteer study, Woodall et al found increases in blood pressure and heart rate during awake nasal FOB with the spray-as-you-go technique combined with nebulised lignocaine without intravenous sedation3. They also reported a failure rate of 10% and complications related to local trauma to the nose. Translaryngeal instillation of local anaesthetic technique is another method used for airway anaesthesia. However, translaryngeal block predominantly produces anaesthesia of infraglottic structures and the trachea; it produces inadequate anaesthesia of the supraglottic area for FOB intubation. Moreover, it can be associated with cough, bleeding and airway compromise1. In contrast, bilateral SLN block combined with topical anaesthesia has been found to produce better haemodynamic stability and patient comfort than the spray-as-you-go technique4. The SLN arises from the vagus nerve and descends posteriorly to the carotid arteries towards the larynx. The SLN divides into external and internal branches. The external branch has a motor supply to the cricothyroid muscle. The internal branch provides sensory innervation to the base of the tongue, epiglottis and the mucous membrane of the larynx as far inferiorly as the vocal folds. The internal branch passes immediately inferior to the greater horn of the hyoid bone and approaches the thyrohyoid membrane accompanied by the SLA, a branch of the STA. The approach to blockade of the ibSLN can be either anterior or lateral5. The anterior approach involves identifying the thyroid cartilage incisura and introducing the needle in a cranial and lateral direction. In the commonly used lateral approach, the nerve is blocked by inserting the needle below and slightly anterior to the GHH. In a large study, the success of bilateral ibSLN blocks using a lateral approach combined with topical application of local anaesthetic was found to be 92%6. The failure rate could be due to variations in the anatomical position of SLN with respect to hyoid bone. Furlan found that the distance between the ibSLN and GHH varied between 0 to 20.1 mm (mean 2.4 mm, variance 10.9 mm)5. In a cadaveric study of structures around the GHH, Lemaire et al found that the hypoglossal nerve and lingual artery lie approximately 6.3±1.8 mm superior in the submandibular triangle and the ibSLN lies approximately 9.6±1.7 mm below the GHH7. Wide variation exists in the origin of the superior thyroid artery. The STA arises from the bifurcation of the carotid artery (type I 49.3%), but can arise from either the common carotid artery (type II 26.6%) or external carotid artery (type III 23.2%). The origin of the STA lies approximately within 1.5 cm of the carotid bifurcation in type II and III8. Despite this variable origin, the arterial pulsation seen immediately below the lingual artery pulsations is mainly the STA, which helps its identification. The SLA is usually the first branch of STA. Infrequently, it can arise directly from the external carotid artery (78%) or carotid bifurcation8. Kiray et al in a cadaveric study found that the ibSLN is the only nerve to traverse between the GHH and the thyroid cartilage from lateral to medial side. It is accompanied by the superior laryngeal artery9. The position of the SLA is considered to be a useful landmark for identification of the ibSLN during surgical dissections10. Similarly, we have used this anatomical landmark to identify and successfully block the ibSLN. References 1.Simmons ST, Schleich AR. Airway regional anaesthesia for awake fiberoptic intubation. Reg Anesth Pain Med 2002; 27:180-192. 2.Xue FS, Liu HP, He N, Xu YC, Yang QY, Liao X et al. Sprayas-you-go airway topical anaesthesia in patients with a difficult airway: a randomized, double-blind comparison of 2% and 4% lignocaine. Anesth Analg 2009; 108:536-543. 3.Woodall NM, Harwood RJ, Barker GL. Complications of awake fibreoptic intubation without sedation in 200 healthy anaesthetists attending a training course. Br J Anaesth 2008; 100:850-855. 4.Kundra P, Kutralam S, Ravishankar M. Local anaesthesia for awake fibreoptic nasotracheal intubation. Acta Anaesthesiol Scand 2000; 44:511-516. 5.Furlan JC. Anatomical study applied to anaesthetic block technique of the superior laryngeal nerve. Acta Anaesthesiol Scand 2002; 46:199-202. 6.Gotta AW, Sullivan CA. Anaesthesia of the upper airway using topical anaesthetic and superior laryngeal nerve block. Br J Anaesth 1981; 53:1055-1058. 7.Lemaire V, Jacquemin G, Nelissen X, Heymans O. Tip of the greater horn of the hyoid bone: a landmark for cervical surgery. Surg Radiol Anat 2005; 27:33-36. 8.Vázquez T, Cobiella R, Maranillo E, Valderrama FJ, McHanwell S, Parkin I et al. Anatomical variations of the superior thyroid and superior laryngeal arteries. Head Neck 2009; 31:1078-1085. 9.Kiray A, Naderi S, Ergur I, Korman E. Surgical anatomy of the internal branch of the superior laryngeal nerve. Eur Spine J 2006; 15:1320-1325. 10.Monfared A, Kim D, Jaikumar S, Gorti G, Kam A. Microsurgical anatomy of the superior and recurrent laryngeal nerves. Neurosurgery 2001; 49:925-933. Anaesthesia and Intensive Care, Vol. 38, No. 5, September 2010 Copyright of Anaesthesia & Intensive Care is the property of Australian Society of Anaesthetists and its content may not be copied or emailed to multiple sites or posted to a listserv without the copyright holder's express written permission. However, users may print, download, or email articles for individual use.