Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
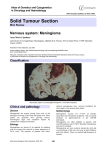
~1~ Copyright ©2015 By Reviews at LibraryOfMedicine.com, Library Of Medicine, LLC Central Nervous System Tumors: Meningioma Jeremy Badach B.S, Chirag D. Gandhi MD FACS FAANS Neurological Institute of New Jersey Rutgers New Jersey Medical School, Newark, NJ Abstract A meningioma is usually a slow growing tumor originating from the outer coverings of the brain and spinal cord. Many are asymptomatic and occur in 2‐3% of the population. Symptomatic meningiomas in the skull can cause patients a range of neurological symptoms including sensory loss, headaches, seizures, and paralysis.28 Symptomatic spinal meningiomas can cause pain, sensory loss, weakness, and bowel and bladder dysfunction. 14 Meningiomas can be diagnosed with CT (Computed Tomography) or MRI (Magnetic Resonance Imaging) scans with contrast although MRI with contrast is preferred. They can be treated with radiosurgery or surgical removal, with endovascular treatment and radiotherapy as an additional treatment.28 Background Information The meninges are three layers of tissue that cover the brain and spinal cord. The outer is the dura mater, the middle is the arachnoid mater, and the inner is the pia mater. The dura mater is the most external layer and sits immediately below the skull. In this layer lies the sinuses (large blood vessels that collect blood from veins in the brain and carry it into large veins in the neck). The dura mater, as the name would suggest, is tough and stiff and located throughout the inside of skull and bony orbits (compartments which house the eyes). Nerves also lie in this layer and pressure on the dura can result in headaches. The arachnoid mater sits between the pia mater and dura mater. It is thin and delicate and follows the surface of the dura mater. It is important to note that meningiomas arise from cells of the arachnoid mater called arachnoid rest cells. Between the arachnoid mater and pia mater is the subarachnoid space, which is filled by cerebral spinal fluid (CSF). The CSF delivers nutrients to nerves in the brain and spinal cord. Blockage of CSF drainage or interruption of CSF flow (ventricles and aqueduct) can cause a buildup of CSF. Larger meningiomas can cause CSF accumulation that may need other surgical treatments. January 2015 Volume 1 Number 4 ~2~ Copyright ©2015 By Reviews at LibraryOfMedicine.com, Library Of Medicine, LLC Below the subarachnoid space and directly on the brain and spinal cord tissue is the pia mater. The pia mater is next to the branches of the internal carotid arteries which deliver blood to the brain. Growth of a meningioma that puts pressure on the pia mater can cause seizures. Why do we get it? A meningioma is a benign (slow rate of doubling) neoplasia (tumor or mass) of the arachnoid mater. It can be in association with a genetic susceptibility, environmental factors, a combination of these factors, or be idiopathic (unknown origin) in nature. Environmental factors, or carcinogens, include chemical, biological, and physical agents. Environmental factors causing meningioma formation and growth are thought to include exposure to ionizing radiation (nuclear weapons and accidents, occupational hazards [flight crew, mining, various research and medical fields], and medicinal procedures [CT scans, X‐rays oncological radiation]). The likelihood of developing a meningioma secondary to radiation in children is increased because of their increased sensitivity.7,18,27 Cellular phone usage has been shown to have no effect on developing a meningioma (studied up to 10 years of cell phone usage).26 Another environmental risk factor is head trauma although the mechanism is unknown.20 There is also a possible link between high levels of sex hormones [progesterone, estrogen, and androgen] and meningioma growth but it has not been confirmed in population studies.29 Meningiomas affect 6 in 100,000 people annually in the United States and is the most common type of brain tumor, accounting for 13‐26%. They are twice as common in females as males but malignant meningiomas are equally common in both genders. Malignant meningiomas, which are a rare variant, present most often in or after the fifth decade. Both genders have an increasing likelihood of meningiomas from age 15 to 79, but then diminishes. 22 In addition, pregnancy may cause an asymptomatic meningioma to become symptomatic due to increased fluid retention and hormonal changes.15 It is worth noting that an estimated 2‐3% percent of people are found to have subclinical (non‐symptomatic) meningiomas upon inspection during autopsy and imaging studies for other medical issues.22,28 There are genetic links to the growth of a meningioma. Changes of tumor suppressor genes or proto‐ oncogenes are responsible for the growth of cancer. The most common mutation, a change in the neurofibromatosis gene (NH2) on chromosome 22q results is thought to cause 60% of meningioma. Additional implicated regions include chromosome 14q, 1p, 6q, 10q, and 18q, but not all genes that participate in the cancer process have been discovered.24,28,29 Increased risk of meningioma is also associated with cancer predisposition syndromes associated with the NH1, PTCH, CREBBP, VHL, PTEN, and CDKN2A genes. Benign meningiomas are usually associated with familial sensitivity to radiation suggesting some radiation‐induced cases are due to a genetic predisposition.11 January 2015 Volume 1 Number 4 ~3~ Copyright ©2015 By Reviews at LibraryOfMedicine.com, Library Of Medicine, LLC Locations Meningiomas are most commonly located within the skull, with about 10% being found in the spine (mostly in the upper back region). Very rarely do meningiomas arise in other areas like the ear, temporal bone (skull), mandible (jaw), foot, mediastinum (central chest), and lung. Meningiomas can metastasize (move to another part of the body) to the lungs, muscles, liver, lymphatic system, and kidneys but this occurs very rarely (0.1% of meningioma). It can enter the lymphatic and blood vessels of the brain as well as the brain and skull tissue. Cranial meningiomas are labeled convexity (surface of the brain), parasagittal (adjacent to falx cerebri), and intraventricular (in the ventricles), and skull base. Meningiomas of the skull base can be further distinguished as sphenoid wing, olfactory groove, posterior fossa, suprasellar, cavernous sinus, intraorbital, clivus, cerebropontine angle and foramen magnum. Most of meningiomas are convexity, parasagittal, or sphenoid wing meningiomas.22,28 Grading System The World Health Organization has a grading system for meningiomas based on histology (cell architecture and severity). There are three grades of meningioma. A Grade I meningioma (~90% of meningiomas) are called benign (slow growing) and follow a benign clinical course. This type of meningioma has distinct borders (it does not invade surrounding tissue). A Grade II meningioma (5‐7% of meningiomas) is called atypical and is characterized by cells either that divide faster than that of Grade I or have cell architecture that is abnormal based on several parameters. A Grade III meningioma (1‐3% of meningiomas) is called anaplastic. They have very high rates of division, are likely to enter brain tissue and metastasize, and have a very high rate of return. How do we diagnose it? What are the symptoms? The symptoms of meningioma are quite broad. Asymptomatic meningiomas can be in one’s body their entire life without showing symptoms or causing problems, only to be later found on autopsy or when imaging for another condition. Symptomatic meningiomas can present in a wide variety of ways depending on the locations in which they can occur. When they begin growing, they can compress or enter nearby structures including brain tissue, the spinal cord, CSF channels, blood vessels, and venous sinuses. Intracranial meningiomas commonly cause seizure disorders (27‐67%). Other symptoms include increased intracranial pressure, due to the invading meningioma or swelling of the brain as a result of the body’s reaction to the meningioma. Additional typical symptoms of meningioma include morning headaches and severe headaches. They can also present with symptoms related to the brain region which they are affecting. This can include one or a few of the following: visual deficits, hearing deficits, pain, numbness, paresthesia (tingling), loss of motor function, decreased alertness, difficulty speaking or January 2015 Volume 1 Number 4 ~4~ Copyright ©2015 By Reviews at LibraryOfMedicine.com, Library Of Medicine, LLC understanding others, difficulty swallowing, difficulty reading and writing, tremors, loss of balance and coordination, abnormal taste or smell and loss of consciousness. Meningiomas can sometime imitate transient ischemic attacks (TIAs or temporary lack of blood flow) or intracranial bleeds by presenting with many of the symptoms listed previously, but typically a meningioma will cause symptoms limited to the nearby brain region or nerve. Spinal meningiomas generally present with motor and/or sensory deficits. Thoracic meningiomas present with slowly increasing spastic partial paraparesis (paralysis of the lower body) with or without radiating (traveling) or night‐time pain. These symptoms can imitate other serious neurological conditions such as demyelinating disease. Cervical and craniocervical spinal meningiomas present with symptoms of spastic quadriparesis (paralysis below the head) with or without low bulbar signs (Issues with swallowing, chewing, and speaking due to injury of some cranial nerves). Occasionally, spinal meningiomas present as a sudden spinal event due the meningioma affecting the spinal cord’s blood supply. Diagnostic studies/testing Imaging (CT scan or MRI) is essential for the diagnosis of meningiomas. MRI imaging is the preferred technique due to its ability to clearly outline the location of tumor. Gadolinium (MRI contrast agent) is commonly used to better visualize the tumor. CT scans, which are better for visualizing bone, may also be used to determine whether the meningioma is interacting with, or invading the bones of the skull (more common in skull base meningiomas). If a meningioma is close to a major artery or vein, MR angiography or venography can be used to determine blood flow through the vessels. This test is minimally invasive, very low risk and can help describe the blood supply of the tumor and if the tumor is invading any of the structures carrying blood. There are some diseases that can imitate meningioma’s presentation on diagnostic imaging. These include solitary fibrous tumors, gliosarcomas, leiomyosarcomas, hemangiopericytomas, melanocytomas, Hodgkin's disease, plasmacytomas, inflammatory pseudotumors, neurosarcoidosis, plasma cell granulomas, Rosai‐Dorfman disease, Castleman's disease, xanthomas, rheumatoid nodules, and tuberculomas.12 Diseases that mimic a skull‐invading meningioma include bony metastases, osteomas, fibrous dysplasia, Paget’s disease, hyperostosis frontalis interna, hemolytic anemias, and hyperparathyroid disorders. Natural History January 2015 Volume 1 Number 4 ~5~ Copyright ©2015 By Reviews at LibraryOfMedicine.com, Library Of Medicine, LLC Meningiomas are generally benign tumors and many of them are asymptomatic and incidental. Asymptomatic meningiomas found in the elderly or meningiomas that contain calcifications have low chances of growth and therefore likely remain asymptomatic. Meningiomas found in younger people (<70) have a longer time to grow and develop further mutations; as such they have a higher likelihood to become symptomatic. If untreated, asymptomatic meningiomas grow in only about 1/3 of tumors. Those that grow do so by an average of 4 mm per year. Therefore if left alone, benign asymptomatic meningiomas are more likely to remain asymptomatic and treatment needs to be taken on a case‐by‐ case basis. However, benign meningiomas can grow and cause symptoms by pushing brain structures or becoming atypical or anaplastic. Survival rates for symptomatic benign meningiomas are greater than 80% at 5 years. Growth of a benign meningioma can continue at a variable rate and cause increasing neurological problems. Small growth near important structures can be more problematic. For example, growth into the sinuses can prevent the possibility of a complete surgical resection and can be more likely to metastasize. Growth near the optic chiasm can cause vision loss with small amounts of pressure. Of the 97.5 /100,000 Americans who have a symptomatic meningioma, only around 5% are atypical or anaplastic. Metastasis to other parts of the body is extremely rare. Behavior of both atypical and anaplastic meningioma are similar in that they cause increasing neurological deficits; however, atypical meningiomas have a mortality rates of 21% at 5 years while anaplastic meningiomas have a median survival of 1.5 years and 5‐year mortality rate of 68%. Non‐Operative Treatment Options If a meningioma has been deemed as low risk by a doctor, following multiple imaging studies, they may wish to continue with repeated imaging for as long as is necessary, to monitor growth and be sure that no symptoms develop. Some meningiomas require further treatment. Radiotherapy, the use of high‐energy radiation to damage tumor cells, has been used to treat meningiomas. It can be used as a primary treatment but can also be used preoperatively, to shrink the tumor, and postoperatively, to reduce tumor reappearance rates. As an alternative to surgery, radiotherapy has little data to compare it to surgery. Side effects include sore skin, tiredness, hair loss, nausea, loss of appetite, and slightly increased risk of developing cancer (increased risk in children).28 Radiosurgery or stereotactic radiotherapy, is a fairly new technique. It relies on a focused dosage of radiation that reduces radiation applied to healthy tissue. This enables a larger dosage of radiation to be applied to the tumor. A side effect of treating a meningioma, unproven by pathology, with radiosurgery is contradictory tumor growth in 2.3% of cases.10 There are several options for radiosurgery, Gamma Knife, CyberKnife, and others, with more being introduced as technology evolves. CyberKnife utilizes a robot to stabilize the beam so that body January 2015 Volume 1 Number 4 ~6~ Copyright ©2015 By Reviews at LibraryOfMedicine.com, Library Of Medicine, LLC movements based on breathing or other subtle movements do not affect the target area in order to increase accuracy. Gamma Knife fixes the head with a frame in order to increase accuracy. Both technologies are evolving and experience in each varies greatly from hospital to hospital. Operative Treatment Options Craniotomy (opening of the skull) and microsurgery (optional use of microscope when necessary) are used for the surgical removal of a symptomatic meningioma. The length and risk of surgery vary significantly depending on the exact location of the tumor. Tumors of the spine, falx cerebri, and brain surface have generally less morbidity. There are different grades (Simpson grades) to describe the removal of a meningioma. A grade I excision is a complete removal of the tumor, and some of its surrounding meninges and bone. A grade II excision is the removal of the tumor while cauterizing (heating) surrounding meninges. A grade III excision is the removal of a portion of the tumor while leaving a small piece intact (the case where it is adjacent to an important structure). A grade IV excision is an extended biopsy leaving a large piece intact. A grade V excision is decompression of increased intracranial pressure (locally or generally) without removing any tumor.28 In general, the surgical goal is attempt as aggressive of a resection as possible without causing neurological damage. Simpson Grade 1 excision, although preferred, is not always possible, depending on the location of the tumor. Pre‐operative endovascular embolization (blocking of vessels) of cranial meningiomas, has been shown to reduce bleeding during the operation by blocking blood supply to the tumor. It is estimated that the complication rate (bleeding or neurological dysfunction) is less than 0.6%; however, the outcomes vary.3,4 This technique is not used for all meningioma tumors prior to surgery but rather those that have a more complex blood supply. Radiotherapy, is often used after partial resection, tumor recurrence, or attempted total resection of a grade II or III meningioma. There are few studies that have successfully evaluated the efficacy of this post‐operative radiation in the long‐term. Smaller studies present inconsistent results about its ability to lower recurrence rates.1,5,8,25,28 Treatments Under Development Currently there are no FDA approved chemotherapy agents to treat meningioma although some medications are undergoing clinical trials.17 Similarly, there have been very few medications that show effectiveness in treating meningioma due to the fact that the cause of the disease is not completely known. Drugs that block hormones and growth factors have also been unsuccessful so far for similar reasons. The drug Celecoxib, which has been cleared by the FDA for slowing growth of several other January 2015 Volume 1 Number 4 ~7~ Copyright ©2015 By Reviews at LibraryOfMedicine.com, Library Of Medicine, LLC cancers, has been shown to be effective in slowing growth of meningioma, increasing meningioma cell death, and decreasing meningioma blood supply.6 Additionally, gene therapy, the passage of curative or normal genes to a diseased cell, is being developed for the treatment of meningioma.9 Treatment Outcomes Survival and quality of life after surgery is based on size and location of the tumor, excision (Simpson) grade, histological grading, and preoperative conditions of the patients. Five‐year survival is 69%‐81% for those aged below 65 and 56% for those aged 65 or older. 27,29 Surgical problems occur (neurological deficits) with rates of 4.9% in asymptomatic meningiomas and 23% in symptomatic meningiomas. Rates in spinal meningioma are 35% morbidity and 0.8% mortality. A large predictor of problems in spinal meningioma is tumor calcification (tumor hardening). Recurrence rate for most meningiomas has been associated with the amount of resection. Simpson Grade I removal has a recurrence rate from 9% at 5 years and 20% at 10 years. Simpson Grade II has a recurrence rate of 19% at 5 years. Simpson grade III results in a recurrence rate of 29% at 5 years. Simpson Grade IV and Simpson Grade V have even larger recurrence rates at 5 years27,29. Recurrence rate is highly dependent on the grade of meningioma. Benign meningiomas recur at 6.96%, atypical at 34.6%, and anaplastic at 72.7% after surgical removal27,29. Conclusion Symptomatic meningioma is a common intracranial tumor that can lead to headaches, seizure disorders, and varied neurological deficits. Although some risk factors are known, the genetic and environmental causes are not completely characterized. Patient history, neurological examination, and imaging (MRI and CT) are useful in diagnosis. Non‐operative management can include interval imaging and observation, radiosurgery, and radiotherapy. Radiation treatments can reduce the size of tumors and preserve neurologic function, but are not known to reduce recurrence rates when compared surgery. Chemotherapy and medical drugs are currently in development. Surgical treatments include craniotomy and spinal surgery. Radiation treatment and pre‐operative endovascular embolization may be used as an adjunct to surgery. Bullet Points Symptomatic Meningioma is the most common brain tumor affecting 97.5 per 100,000. January 2015 Volume 1 Number 4 ~8~ Copyright ©2015 By Reviews at LibraryOfMedicine.com, Library Of Medicine, LLC Meningiomas have some known genetic and environment causes, but all of its causes have not been characterized. Non‐operative choices may include: radiographic imaging and observation, radiosurgery, and radiotherapy. Surgical choices include: craniotomy or spinal surgery with or without preoperative embolization and postoperative radiotherapy. Radiosurgery treatment tends to preserve neurological function with lower mortality/morbidity, however their recurrence rates are unknown long term. References 1. Adegbite AB, Khan MI, Paine KWE, Tan LK: The recurrence of intracranial meningiomas after surgical treatment. J Neurosurg 58:51–56, 1983 http://dx.doi.org/10.3171/jns.1983.58.1.0051 2. Aghi MK, Carter BS, Cosgrove GR, Ojemann RG, Amin‐Hanjani S, Martuza RL, et al.: Long‐Term Recurrence Rates of Atypical Meningiomas After Gross Total Resection With or Without Postoperative Adjuvant Radiation. Neurosurgery 64:2009 http://dx.doi.org/10.1227/01.NEU.0000330399.55586.63 3. Bateman BT, Lin E, Pile‐Spellman J: Definitive Embolization of Meningioma: A Review. Interv Neuroradiol 11:179–188, 2005 4. Bendszus M, Martin‐Schrader I, Schlake HP, Solymosi L: Embolization of intracranial meningiomas without subsequent surgery. Neuroradiology 45:451–455, 2003 5. Black PM: Meningiomas. Neurosurgery 32:1993 http://dx.doi.org/10.1097/00006123‐ 199304000‐00023 6. Choy W, Kim W, Nagasawa D, Stramotas S, Yew A, Gopen Q, et al.: The molecular genetics and tumor pathogenesis of meningiomas and the future directions of meningioma treatments. Neurosurg Focus 30:E6, 2011 7. Claus EB, Calvocoressi L, Bondy ML, Schildkraut JM, Wiemels JL, Wrensch M: Dental x‐rays and risk of meningioma: Dental X‐Rays and Risk of Meningioma. Cancer 118:4530–4537, 2012 http://dx.doi.org/10.1002/cncr.26625 8. Curry WT, McDermott MW, Carter BS, Barker FG: Craniotomy for meningioma in the United States between 1988 and 2000: decreasing rate of mortality and the effect of provider caseload. J Neurosurg 102:977–986, 2005 January 2015 Volume 1 Number 4 ~9~ Copyright ©2015 By Reviews at LibraryOfMedicine.com, Library Of Medicine, LLC 9. Dirven CMF, Grill J, Lamfers MLM, van der Valk P, Leonhart AM, van Beusechem VW, et al.: Gene therapy for meningioma: improved gene delivery with targeted adenoviruses. J Neurosurg 97:441–449, 2002 http://dx.doi.org/10.3171/jns.2002.97.2.0441 10. Flickinger JC, Kondziolka D, Maitz AH, Lunsford LD: Gamma knife radiosurgery of imaging‐ diagnosed intracranial meningioma. Int J Radiat Oncol 56:801–806, 2003 http://dx.doi.org/10.1016/S0360‐3016(03)00126‐3 11. Flint‐Richter P, Sadetzki S: Genetic predisposition for the development of radiation‐associated meningioma: an epidemiological study. Lancet Oncol 8:403–410, 2007 12. Johnson MD, Powell SZ, Boyer PJ, Weil RJ, Moots PL: Dural lesions mimicking meningiomas. Hum Pathol 33:1211–1226, 2002 http://dx.doi.org/10.1053/hupa.2002.129200 13. Kondziolka D, Mathieu D, Lunsford LD, Martin JJ, Madhok R, Niranjan A, et al.: Radiosurgery As Definitive Management of Intracranial Meningiomas. Neurosurgery 62:2008 http://dx.doi.org/10.1227/01.NEU.0000311061.72626.0D 14. Levy WJ, Bay J, Dohn D: Spinal cord meningioma. J Neurosurg 57:804–812, 1982 http://dx.doi.org/10.3171/jns.1982.57.6.0804 15. Lusis EA, Scheithauer BW, Yachnis AT, Fischer BR, Chicoine MR, Paulus W, et al.: Meningiomas in Pregnancy: A Clinicopathologic Study of 17 Cases. Neurosurgery 71:2012 http://dx.doi.org/10.1227/NEU.0b013e31826adf65 16. Marosi C, Hassler M, Roessler K, Reni M, Sant M, Mazza E, et al.: Meningioma. Crit Rev Oncol Hematol 67:153–171, 2008 http://dx.doi.org/10.1016/j.critrevonc.2008.01.010 17. Moazzam AA, Wagle N, Zada G: Recent developments in chemotherapy for meningiomas: a review. Neurosurg Focus 35:E18, 2013 http://dx.doi.org/10.3171/2013.10.FOCUS13341 18. Pearce MS, Salotti JA, Little MP, McHugh K, Lee C, Kim KP, et al.: Radiation exposure from CT scans in childhood and subsequent risk of leukemia and brain tumours: a retrospective cohort study. The Lancet 380:499–505, 2012 19. Perry A, Scheithauer BW, Stafford SL, Lohse CM, Wollan PC: Malignancy in meningiomas: A clinicopathologic study of 116 patients, with grading implications. Cancer 85:2046–2056, 1999 http://dx.doi.org/10.1002/(SICI)1097‐0142(19990501)85:9%253C2046::AID‐CNCR23%253E3.0.CO;2‐M 20. Phillips LE, Koepsell TD, van Belle G, Kukull WA, Gehrels J‐A, Longstreth WT: History of head trauma and risk of intracranial meningioma: Population‐based case‐control study. Neurology 58:1849– 1852, 2002 21. Reinert M, Babey M, Curschmann J, Vajtai I, Seiler RW, Mariani L: Morbidity in 201 patients with small sized meningioma treated by microsurgery. Acta Neurochir (Wien) 148:1257–1266, 2006 January 2015 Volume 1 Number 4 ~ 10 ~ Copyright ©2015 By Reviews at LibraryOfMedicine.com, Library Of Medicine, LLC http://dx.doi.org/10.1007/s00701‐006‐0909‐z 22. Rohringer M, Sutherland GR, Louw DF, Sima AA: Incidence and clinicopathological features of meningioma. J Neurosurg 71:665–672, 1989 http://dx.doi.org/10.3171/jns.1989.71.5.0665 23. Rubin G, Herscovici Z, Laviv Y, Jackson S, Rappaport ZH: Outcome of untreated meningiomas. Isr Med Assoc J IMAJ 13:157–160, 2011 24. Ruttledge MH, Sarrazin J, Rangaratnam S, Phelan CM, Twist E, Merel P, et al.: Evidence for the complete inactivation of the NF2 gene in the majority of sporadic meningiomas. Nat Genet 6:180–184, 1994 http://dx.doi.org/10.1038/ng0294‐180 25. Sandalcioglu IE, Hunold A, Müller O, Bassiouni H, Stolke D, Asgari S: Spinal meningiomas: critical review of 131 surgically treated patients. Eur Spine J 17:1035–1041, 2008 26. Schuz J: Cellular Phones, Cordless Phones, and the Risks of Glioma and Meningioma (Interphone Study Group, Germany). Am J Epidemiol 163:512–520, 2006 27. Shintani T, Hayakawa N, Hoshi M, Sumida M, Kurisu K, Oki S, et al.: High Incidence of Meningioma among Hiroshima Atomic Bomb Survivors. J Radiat Res (Tokyo) 40:49–57, 1999 http://dx.doi.org/10.1269/jrr.40.49 28. Whittle IR, Smith C, Navoo P, Collie D: Meningiomas. The Lancet 363:1535–1543, 2004 http://dx.doi.org/10.1016/S0140‐6736(04)16153‐9 29. Wiemels J, Wrensch M, Claus EB: Epidemiology and etiology of meningioma. J Neurooncol 99:307–314, 2010 http://dx.doi.org/10.1007/s11060‐010‐0386‐3 30. Yamasaki F, Yoshioka H, Hama S, Sugiyama K, Arita K, Kurisu K: Recurrence of meningiomas. Cancer 89:1102–1110, 2000 http://dx.doi.org/10.1002/1097‐0142(20000901)89:5%3C1102::AID‐ CNCR20%3E3.0.CO;2‐L January 2015 Volume 1 Number 4