Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
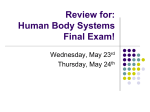
eBooks Proprioception: The Forgotten Sixth Sense Chapter: Elbow Problems and Proprioception Edited by: Defne Kaya Published Date: May, 2015 Published by OMICS Group eBooks 731 Gull Ave, Foster City, CA 94404, USA Copyright © 2016 OMICS Group All book chapters are Open Access distributed under the Creative Commons Attribution 3.0 license, which allows users to download, copy and build upon published articles even for commercial purposes, as long as the author and publisher are properly credited, which ensures maximum dissemination and a wider impact of our publications. However, users who aim to disseminate and distribute copies of this book as a whole must not seek monetary compensation for such service (excluded OMICS Group representatives and agreed collaborations). After this work has been published by OMICS Group, authors have the right to republish it, in whole or part, in any publication of which they are the author, and to make other personal use of the work. Any republication, referencing or personal use of the work must explicitly identify the original source. Notice: Statements and opinions expressed in the book are those of the individual contributors and not necessarily those of the editors or publisher. No responsibility is accepted for the accuracy of information contained in the published chapters. The publisher assumes no responsibility for any damage or injury to persons or property arising out of the use of any materials, instructions, methods or ideas contained in the book. A free online edition of this book is available at www.esciencecentral.org/ebooks Additional hard copies can be obtained from orders @ www.esciencecentral.org/ebooks I eBooks Elbow Problems and Proprioception Derya Celik1*, Ebru Kaya Mutlu2 PT, PhD, Associate Proffesor, Istanbul University, Faculty of Health Sciences, Division of Physiotherapy and Rehabilitation, Istanbul, Turkey 1 PT, MSc, Istanbul University, Faculty of Health Sciences, Division of Physiotherapy and Rehabilitation, Istanbul, Turkey 2 *Corresponding author: Derya Çelik, PT, PhD, Associate Proffesor, Istanbul University, Faculty of Health Sciences, Division of Physiotherapy and Rehabilitation, Istanbul, Turkey, Tel: 0090 212 414 1528, E-mail: [email protected] Abstract The term ‘proprioception’ describes the ability to determine the spatial orientation and movement of body parts from the body itself. It is a fundamental ability used every day to aid people in relating and communicating with their environment and to enhance motor skills. Receptors found in the skin, in tendons and muscles and in joints all produce stimuli necessary for proprioception. Typical joint proprioception may vary in individuals who suffer from diseases affecting the elbow. Professional athletes are particularly vulnerable to insufficiencies in proprioception. The loss of proprioception in patients with elbow conditions has not been comprehensively researched despite the importance of such diseases in relation to the loss of proprioception, as with conditions affecting other joints. In this chapter we will discuss the anatomy of elbow, definition of proprioception, assessment and treatment of elbow joint proprioception. In addition factors influenced the proprioception will be discussed. Elbow Anatomy The elbow joint technically consists of three joints: 1) the humeroulnar joint, 2) the humeroradial joint, and 3) the proksimal radioulnar joint. These joints operate together to form the full elbow complex. There are two articular surfaces present at the distal end of the humerus. The first, the trochlea, controls the ulna, whereas the second, the capitulum, controls the radius head. Both extension and flexion operate in this process, by interacting with the two joint surfaces. Additionally, the radius works in conjunction with the ulna radial notch, producing a complex called the proximal radioulnar joint. This operates via supination and pronation across the length of the distal radioulnar joint. The three aforementioned subsidiary joints are encased within the elbow capsule. However, the distal radioulnar joint is located separately from the rest of the elbow complex, in spite of how it operates in conjunction with the proximal radioulnar joint [1,2]. For normal functioning, the upper extremity relies on an elbow complex that can move freely and displays strength and stability. The spatial mobility of the hand is supported by 1 the elbow and forearm structure through two functions, namely, upper extremity shortening and lengthening as well as forearm rotation. The hand would not be able to undertake the wide range of activities that it does, including, among many others, eating, dressing, lifting, turning throwing, catching, and using different instruments, without the muscles, which provide it control and keep it stable [3,4]. The majority of daily activities demand not only a 100˚ arc of flexion and extension at the elbow, particularly with a range from 30˚ to 130˚, but also a forearm rotation of 100˚ balanced between pronation and supination [3]. The extension of the elbow is necessary for tasks such as putting on socks, while the bending of the elbow is demanded by actions such as taking a drink or eating a meal. Muscles help to dynamically stabilise and control the elbow joint. A variety of flexor muscles control this action: biceps brachii, brachialis and brachioradialis. Elbow flexion and forearm supination are achieved via the biceps brachii. Further elbow flexion is utilised via the brachialis. The brachioradialis had multiple functions, including elbow flexion, semisupination, and semipronation. The triceps brachii and related anconeus muscles are the elbow extensor muscles [1]. The Medial Collateral Ligament (MCL) and Lateral Collateral Ligament (LCL) and the anterior and posterior joint capsule are the elbow’s static soft-tissue stabilisers. The primary stabiliser is the MCL and motion ranges from 20-120 degrees, and the elbow’s primary lateral stabiliser is the LCL. However, it is at the joint capsule that an elbow’s stability begins and it is used for all three of the articulations of which the elbow is capable. In both flexion and extension, movement is made possible by the anteriorly and posteriorly unconstrained capsule. The extra support provided by the MCL and LCL means that the capsule is rigid laterally and medially. The joint capsule can produce proprioception as it has a number of nerves. It, in fact, acts as the connection to proprioceptivity for the upper part of the hand [1,2,4]. The elbow joint can be influenced by the functions of the shoulder, the hand and wrist and the cervical spine. The elbow complex can be affected by restrictions or weakness found in these functions. Thus, a comprehensive evaluation of proprioception and the treatment of disorders or injuries of the elbow require a full understanding of the anatomical system of not only the elbow but related joints also. Proprioception Sensory input sent through the brain from receptors in the joints, skin, muscles, eyes and the vestibular apparatus of the inner ear produce proprioception, the capacity to sense the spatial orientation of body parts and their movements [5-9] (Figure 1). AFFERENT INPUT LEVELS OF MOTOR CONTROL Peripheral afferents • • • Joint Muscle Skin Spinal refleks Visual receptors Vestibuler receptors Central Nervous System MUSCLE Cognitive Programming Figure 1: Summary of Proprioceptive System. Figure 1: Summary of Proprioceptive System. Muscle receptors The components of muscle receptors are muscle spindles and Golgi tendon organs [6,7]. Special muscle fibers, muscle spindles are positioned parallel to ordinary skeletal muscle fibers and are present in a large proportion in the “skill” muscles of the hands, but in a more limited number in the “strength” muscles of the lower extremity and back [10]. The gamma 2 feedback loop is employed by these muscle spindles to transmit information to the central nervous system. This loop provides indirect information regarding joint position through the detection of modifications in the length of the muscles and velocity of contraction. The stimulation of skeletal muscle activates the muscle spindles, thus ensuring that tension is preserved. By contrast, dissipation of tension minimises or terminates muscle spindle activity. Compared to error correction via visual stimuli, which can take up to 200 ms, correction of muscle tension through the gamma feedback loop can be done in 30-80 ms. The location of the Golgi tendon organs is in the tendons, in proximity to the musculotendinous junction and in line with the muscle fibers. The monitoring of muscle tension is the role of these Golgi tendon organs, an increase in muscle tension inducing an increase in the firing rate as well. A reflex decrease in muscle tension occurs when the Golgi tendon organs generate excessive firing rates [5-7]. Joint receptors Joint capsules, ligaments, fat pads, and the periosteum of different joints all contain joint receptors [5]. These are activated by motion-related alterations in the containing structures, their role being to signal joint position and movement. Joint motion is directly recorded by the joint receptors, which thus add to the information produced by the muscle spindles and Golgi tendon organs [11]. The measurement of joint motion is undertaken by both Ruffini endings and pacinian corpuscles, which can be found in the joint capsule. Positioned on the flexion side of the joint capsule, the Ruffini endings react and gradually adjust not to the dislocation of connective tissue, but rather to loads on the area surrounding the connective tissue. The significant joint motion related to the extension with rotation of the capsule stimulates these receptors. It is assumed that their function is to delimit and protect the unstable joint. On the other hand, the Pacinian corpuscles can be found throughout the capsule, joint and periarticular structures. Due to the fact that they are characterised by rapid adaptation, these receptors are believed to be susceptible to compression, particularly during the occurrence of high velocity transformations arising when the joint accelerates or decelerates during movement [5]. However, as argued by some authors, the contribution of joint receptors may be of considerable importance when muscle and skin signals are unavailable [8,12]. Skin Although the hand is the main location of skin subcutaneous proprioceptive afferent receptors, these receptors are also essential for the elbow and other joints. A kinaesthetic function has been tentatively attributed to the skin stretch Type II receptor characterised by slow adaptation and served by Ruffini endings [13]. In the case of kinaesthesia at the forearm, position and movement-related information is provided by the stretch of skin over the elbow when the elbow is flexed. The stretch of skin of the hand and over more proximal joints produced greater movement illusions when applied in association with muscle vibration than during the separate application of the two stimuli [14]. It is important to emphasise that muscle input was not facilitated by skin input, the cutaneous input produced by the skin stretch being actively and independently involved in kinaesthesia. The skin receptors are capable of providing information specific to the joint due to their close location to each joint [14]. The vestibular systems and eye Signals about the position of the body as a whole is generated by the eyes and the vestibular system. These are activated when there is a variation in the upright posture of the body [9]. Information on vertical and horizontal orientation and movement is provided by the vestibular system (located inside the inner ear) which transmits signals to the central nervous system. The head and body’s orientation and movement within its surroundings is facilitated by the eyes. The occulomotor and vestibuler systems provide information on 3 whether it is the surroundings or the body itself that is in motion. Variations in orientations during rapid movements are signalled by the vestibular system which responds very quickly [5]. Assesment of Elbow Joint Proprioception Joint movement and position perception is yet to be appropriately and objectively assessed for large scale clinical application. At present, the clinical assessment of proprioception is conducted via a non-quantitative joint position perception test, in which subjects are required to give a verbal description of the position of the joint following the passive movement of the segment by the examiner into a limited number of predetermined positions. Moreover, in a clinical context, an additional testing method was applied, which was aimed at determining the extent to which a subject was able to move a joint back into a predetermined position [15]. Both testing methods can be carried out in ipsilateral as well as contralateral matching tasks and with the subject blindfolded. Further methods for assessing proprioception have been employed in a research context. Video cameras, potentiometers and goniometers have been utilised to measure angles when a limb is moved into a fixed position that is intended to match the same position of the limb on the opposite side of the body which has been moved into this position by the examiner. This equipment is also used to measure the extent of kinaesthesia. The conscious recognition of proprioception has been calculated using numerous and varied tools such as electromagnetic tracking mechanisms, commercial isokinetic dynamometers and specially custom-made jigs [15,16]. Methods largely similar to those above have also been employed in the assessment of elbow proprioception. The identification of the most adequate angle for elbow proprioception assessment has constituted the focus of many studies. For instance, elbow position was measured by Brockett et al., [17] with the forearm at angles of 30˚, 60˚ and 90˚ to the horizontal. Walsh et al., [18] selected an angle of 30˚, 60˚ and 90˚ for eccentric movements and an angle of 15˚, 30˚ and 45˚ for concentric movements. Goble et al., [19,20] measured the angle of elbow extension at 15˚ and 30˚, and at 20˚ and 40˚, respectively. However, despite these experiments, no agreement has been reached with regard to the angle of elbow extension or flexion motion that ought to be applied in the evalution of position sense. Based on the response variation exhibited by muscle spindles, Golgi tendon organs, cutaneous afferents and joint afferents as a result of stretch and muscle length, it can be implied that proprioception should also display variation in accordance with joint angles and joint planes. In contrast to joint angles with extreme flexion or extension, enhanced proprioception at the midranges of joint motion has been noted in a horizontal plane [21-24]. In addition, as observed by Gooey et al., [25], unlike an abducted position, the position with the arms in front of the body was more conducive to proprioception. On the other hand, only a handful of assessments have addressed proprioceptive discrepancies across joint angles in a sagittal plane. Nevertheless, recently conducted studies have provided evidence that proprioception in a sagittal plane is not unlike that in a horizontal plane, in that it is optimal at the midranges of joing motion [26-30]. To be more exact, a 90˚ elbow position in relation to the distal segment [26-28,30] is optimal for the joint position sense, the positioning of the joint at different angles being accompanied by a linear increase in errors [26,30]. Joint position sense improvements at angles close to 90˚ were initially attributed to enhanced muscle activation. However, the central role of this mechanism has recently been dismissed on the basis of observations of the same pattern regardless of disruptions to external torque [27] and trunk orientation [28]. It is possible that a position of the hand associated with an elbow flexion of 90˚ facilitates a better adjustment of the neural population vectors. Be that as it may, tasks involving multi-joint movements can determine variation in the precision of the joint position sense, depending on different joint angles. 4 Factors for Affecting Elbow Proprioception Cognition, memory and task matching In an ipsilateral matching task the subject is firstly given a reference joint angle to hold for a few seconds with the joint then being moved back to starting position. The subject is then asked to move the same arm back to the reference joint angle. Memory is clearly a factor in this task as the subject must remember the reference position in order to replicate it. Thus, any memory deficiencies in a subject must be considered when deciding whether to carry out this matching task as it may not accurately reflect the subject’s level of proprioception. In individuals with memory problems, a degree of the perceived failure in proprioception may in truth be indicative of a deficiency in memory [20,31]. In a contralateral matching task the subject must replicate a reference joint angle held by one arm using the opposite arm. In this test the arm holding the reference joint angle remains in this position while the other arm attempts to replicate the angle. The weakness in this form of test is that determining the source of proprioception mistakes is problematic as they may be caused by the arm forming the reference angle or the matching arm. A further problem is that, as opposed to ipsilateral matching tasks, contralateral matching tasks demand a higher level of communication between the two hemispheres of the brain because of the anatomical networks involved in communicating peripheral proprioceptive signals. Thus, in individuals with orthopaedic issues who also suffer from a neurological condition, contralateral matching tasks are not necessary [31]. Affected Extremities - Dominance It is believed that approximately nine out of ten people are right-handed. Various researchers have illustrated that there is no variation in proprioception acuity between the non-dominant and dominant sides of the body [32-34]. This has been shown by comparing joints on either side of the body using a hand repositioning exercise using movements from the shoulder and elbow. More recently, however, it has been illustrated that, particularly when tasks require communication between brain hemispheres, the non-dominant elbow has a particular advantage [19,20,35,36]. It had been identified that, in right-handed individuals, the right arm showed a position-matching advantage over the non-dominant left arm yet the non-dominant left arm showed an accuracy advantage illustrated by a lower number of absolute matching errors than seen in the dominant right arm [20]. For bigger movements this advantage was even more distinct and the nature of the matching motions showed that it was not linked to any variations in the movement strategies of particular limbs. These studies have enriched the understanding of dominant and non-dominant arms and proprioception showing that in right-handed people the left arm and side is better able to interpret proprioceptive data. Furthermore, studies also indicate that proprioception in the dominant right arm does not recover as well after injury as it does in the non-dominant left arm [19,20]. Thus, therapy to improve proprioception in the dominant right elbow following injury should be more extensive than that engaged in for the non-dominant left arm. Age One effect of the aging process is changes in the central and peripheral nervous systems. For example, teenagers are better at matching tasks than children and can more effectively employ kinematic procedures to complete these tasks. In comparison to teenagers, children make a higher number of absolute errors in matching tasks. A child’s matching motions are shorter and less consistent in terms of the speed of such movements. The correlation between mistakes in position replication and age is nonmotonic. From the age of eight, position matching continues to improve until the child is grown [31]. The component of memory in the evaluation of proprioception ability in the elderly, when using matching task models based on memory, is a significant consideration and common daily actions may be 5 performed less successfully [36]. However, it has been argued that it is in fact an inactive lifestyle that contributes more to a decrease in proprioception than memory deficiencies [37]. A fair conclusion to draw would be that proprioceptive information is received quicker in younger people than it is in older people. Visual or proprioseptive feedback Based on the variations between the dominant and non-dominant arms during tasks requiring both arms, it can be seen that the non-dominant arm better processes proprioceptive responses than the dominant arm which may be more dependent on visual information. When an action involving both arms takes place, visual responses are focused on the dominant arm as this is the arm that usually carries out detailed tasks like the manipulation of items, for example, sharpening a pencil, while the non-dominant arm is charged with stabilising objects, for example, holding the pencil-sharpener steady, and thus depends upon proprioceptive information in completing these actions. This clearly shows that the dominant arm is better at processing visual feedback and the non-dominant arm has the edge when it comes to proprioceptive information processing. These differences may illustrate essential variations between the dominant and non-dominant arms and hemispheres when carrying out actions involving both sides and where the non-dominant side must stabilise an item using proprioception and the dominant side must manoeuver an item with the aid of visual information [19,35]. Thus, it can be concluded that to develop elbow joint proprioception in the dominant arm following an elbow injury, proprioceptive information is less valuable that visual information. Task difficulty Overall, for more complex Contralateral Remembered (CR) rather than Ipsilateral Remembered (IR) tasks with a higher target velocity, more matching errors occurred. For IR tasks, a matching advantage in the non-dominant arm in terms of velocity discrimination and matching has been identified. This illustrates that a number of elements, namely task complexity, maximum velocity and favoured limb, affects matching performance in terms of dynamic proprioceptive response. When the velocity of motions was increased and more was required in terms of proprioceptive processing, matching errors also went up. Additionally, in regards to the number of errors in average acceleration in IR tasks, a distinct variation between the dominant and non-dominant arms has equally been identified [35]. Proprioceptive Exercise Proprioception exercise have been found improve function, decrease of the risk of injury and improvement of normal movement pattern. The objective of such activities is for individuals to complete them as precisely as possible. Thus, the activities should start simple and increase in complexity over time. Furthermore, these activities should come early on in the programme during therapy sessions when the individual is not yet too tired to perform them well. Depending on when the injury occurred, proprioception activities start simple and become more difficult. An initial proprioception task will demand sufficient muscle movement to generate the required outcome and are carried out at a relaxed speed and in controlled conditions. Increasing the pace of these exercises or requesting they be carried out in a more controlled way makes them more difficult to complete. Another option when seeking to increase the difficult of such exercises is to require that two or more tasks be carried out at the same time. Problems with the joint capsule, ligaments, tendons and muscles are the main cause of elbow complaints and result in loss of proprioception. Therefore, any therapeutic programme should include activities designed to improve proprioception. The type of activities required will vary depending on the age of the individual concerned and their profession, the nature of 6 the injury and when the injury occurred. Proprioceptive activities may be open kinetic chain exercises or closed kinetic chain exercises and should be selected based on the previously listed factors. Excersie 1: Rolling the ball on the wall or surface [38]. Excersie 2: Rolling the ball on the wall or surface [38]. Excersie 3: Transfering exercise ball [38]. 7 Excersie 4: Weight bearing exercise uneven ground [38]. Excersie 5: Proprioceptive exercise on balance board [38]. Excersie 6: Proprioceptive exercise on unstable moving surface [38]. 8 Excersie 7: Catching a ball [38]. Excersie 8: Throwing and catching a ball [38]. 9 Excersie 9: Transfering body weight on swiss ball in prone position [38]. References 1. Prentice WE (2011) Rehabilitation Techniques for Sports Medicine and Athletic Training. (5thedition), The McGraw-Hill company, New York, USA. 2. Kisner C, Colby LA (2002) Therapeutic Exercise. (5th edition), F.A. Davis company, Philadelphia, United States of America. 3. Morrey BF, An K (2000) Functional evaluation of the elbow. In Morrey, BF (ed.). The Elbow and Its Disorders (3rdedition). WB Saunders company, Philadelphia, USA. 4. Norkin CC (2005) The elbow complex. In: Levangie PK, Norkin CC (eds.). Joint Structure and Function: A Comprehensive Analysis. FA Davis company, Philadelphia, USA. 5. Houglum PA (2005) Therapeutic Exercise For Musculoskeletal Injuries. (2nd edition), Edwards Brothers company, United States of America. 6. Goodwin GM, McCloskey DI, Matthews PB (1972) Proprioceptive illusions induced by muscle vibration: contribution by muscle spindles to perception? Science 175: 1382-1384. 7. Burke D, Hagbarth KE, Löfstedt L, Wallin BG (1976) The responses of human muscle spindle endings to vibration of non-contracting muscles. J Physiol 261: 673-693. 8. Ferrell WR, Gandevia SC, McCloskey DI (1987) The role of joint receptors in human kinaesthesia when intramuscular receptors cannot contribute. J Physiol 386: 63-71. 9. Schmidt RA (1991) Motor Learning Performance. (2nd edition), Human Kinetics company, Champaign, IL, USA. 10. Day RW, Wildermuth BP (1988) Proprioceptive training in rehabilitation of lower extremity injuries. In: Grana WA, Lombardo JA, Sharkey BJ, Stone JA (eds.). Advances in Sport Medicine and Fitness. Chicago, IL, USA. 11. Sage GH (1984) Motor Leaning and Control: A NeuropsychologicalApproach. Wm C Brown Publishers, Dubuque, IA. 12. Burke D, Gandevia SC, Macefield G (1988) Responses to passive movement of receptors in joint, skin and muscle of the human hand. J Physiol 402: 347-361. 13. Chambers MR, Andres KH, von Duering M, Iggo A (1972) The structure and function of the slowly adapting type II mechanoreceptor in hairy skin. Q J Exp Physiol Cogn Med Sci 57: 417-445. 14. Collins DF, Refshauge KM, Todd G, Gandevia SC (2005) Cutaneous receptors contribute to kinesthesia at the index finger, elbow, and knee. J Neurophysiol 94: 1699-1706. 15. DeLisa Joel A, Gans Bruce M, Walsh Nicolas E, Bockenek William L, Frontera Walter R, et al. (2005) Physical Medicine & Rehabilitation: Principles and Practice (4thedition), Lippincott Williams & Wilkins company, Melbourne, Victoria, Australia. 16. Riemann BL, Lephart SM (2002) The sensorimotor system, part I: the physiologic basis of functional joint stability. J Athl Train 37: 71-79. 17. Brockett C, Warren N, Gregory JE, Morgan DL, Proske U (1997) A comparison of the effects of concentric versus eccentric exercise on force and position sense at the human elbow joint. Brain Res 771: 251-258. 10 18. Walsh LD, Hesse CW, Morgan DL, Proske U (2004) Human forearm position sense after fatigue of elbow flexor muscles. J Physiol 558: 705-715. 19. Goble DJ, Brown SH (2008) Upper limb asymmetries in the matching of proprioceptive versus visual targets. J Neurophysiol 99: 3063-3074. 20. Goble DJ, Lewis CA, Brown SH (2006) Upper limb asymmetries in the utilization of proprioceptive feedback. Exp Brain Res 168: 307-311. 21. Wolpert DM, Ghahramani Z, Jordan MI (1995) An internal model for sensorimotor integration. Science 269: 1880-1882. 22. Lönn J, Crenshaw AG, Djupsjöbacka M, Pedersen J, Johansson H (2000) Position sense testing: influence of starting position and type of displacement. Arch Phys Med Rehabil 81: 592-597. 23. Gritsenko V, Krouchev NI, Kalaska JF (2007) Afferent input, efference copy, signal noise, and biases in perception of joint angle during active versus passive elbow movements. J Neurophysiol 98: 1140-1154. 24. Poulton EC (2011) Human manual control. In: comprehensive physiology. Wiley-Blackwell, Hoboken, NJ. 25. Gooey K, Bradfield O, Talbot J, Morgan DL, Proske U (2000) Effects of body orientation, load and vibration on sensing position and movement at the human elbow joint. Exp Brain Res 133: 340-348. 26. Suprak DN, Osternig LR, van Donkelaar P, Karduna AR (2006) Shoulder joint position sense improves with elevation angle in a novel, unconstrained task. J Orthop Res 24: 559-568. 27. Suprak DN, Osternig LR, van Donkelaar P, Karduna AR (2007) Shoulder joint position sense improves with external load. J Mot Behav 39: 517-525. 28. Chapman J, Suprak DN, Karduna AR (2009) Unconstrained shoulder joint position sense does not change with body orientation. J Orthop Res 27: 885-890. 29. Hung YJ, Darling WG (2012) Shoulder position sense during passive matching and active positioning tasks in individuals with anterior shoulder instability. Phys Ther 92: 563-573. 30. King J, Harding E, Karduna A (2013) The shoulder and elbow joints and right and left sides demonstrate similar joint position sense. J Mot Behav 45: 479-486. 31. Goble DJ (2010) Proprioceptive acuity assessment via joint position matching: from basic science to general practice. Phys Ther 90: 1176-1184. 32. Chapman CD, Heath MD, Westwood DA, Roy EA (2001) Memory for kinesthetically defined target location: evidence for manual asymmetries. Brain Cogn 46: 62-66. 33. Roy EA, MacKenzie C (1978) Handedness effects in kinesthetic spatial location judgements. Cortex 14: 250258. 34. Imanaka K, Abernethy B, Yamauchi M, Funase K, Nishihira Y (1995) Hemispace asymmetries and laterality effects in arm positioning. Brain Cogn 29: 232-253. 35. Goble DJ, Brown SH (2007) Task-dependent asymmetries in the utilization of proprioceptive feedback for goaldirected movement. Exp Brain Res 180: 693-704. 36. Goble DJ, Noble BC, Brown SH (2009) Proprioceptive target matching asymmetries in left-handed individuals. Exp Brain Res 197: 403-408. 37. Suetterlin KJ, Sayer AA (2013) Proprioception: where are we now? A commentary on clinical assessment, changes across the life course, functional implications and future interventions. Age Ageing 14:1-6. 38. Berker N, Canbulat N, Demirhan M (2009) Shoulder, Elbow, Knee and Ankle Rehabilitation Protocols (1st edition), Nobel Tip company, Turkey. 11