Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
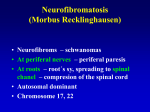
Neurology Board Review November 25, 2008 Neurocutaneous Syndromes Neurofibromatosis 1 AKA Von Recklinghausen Disease 1/3000 individuals Autosomal Dominant 50% sporadic Chromosome 17q Neurofibromin – tumor supressor Diagnostic Criteria NF 1 At least 2 of the following: Café au Lait Macules – 6 or more >5 mm in prepubertal children >15 mm in post pubertal children 2 or more neurofibromas of any type, or one plexiform neurofibroma Axillary or inguinal freckling Optic glioma 2 or more Lisch nodules First degree relative with NF1 Osseous lesion (sphenoid dysplasia, thinning of long bone cortex) Café au Lait Macules Brown hyperpigmented macules with smooth margins Lisch Nodules Hamartomas of the iris Skeletal Abnormalities Short stature Macrocephaly Severe angular scoliosis with dysplasia of the vertebral bodies Defects of posterior-superior wall of the orbit Congenital bowing and thinnning of long bone cortex Pseudoarthrosis of the tibia, fibula, femur, clavicle Disorders of bone growth Erosive bony defects by neurogenic tumor Scalloping of posterior margins of vertebral bodies Skeletal Abnormalities NF 1 Tumors Very common Optic glioma 15% Ependymomas, meningiomas, astrocytomas Intelligence MR is rare Learning disabilities Behavior problems Neurofibromatosis 2 Autosomal Dominant 95% penetrance 1/50,000 Chromosome 22 Merlin or Schwannomin – tumor suppressors Symptoms in teens/twenties Hearing loss, tinnitus, unsteadiness, facial weakness Diagnostic Criteria for NF 2 Bilateral 8th nerve masses seen with imaging OR First degree relative with NF 2 and unilateral 8th nerve mass OR 2 of the following Neurofibroma Meningioma Glioma Schwannoma Juvenile posterior subcapsular lens opacity Tuberous Sclerosis Autosomal Dominant 80% have seizures Infantile spasms TSC1 on Chromosome 9 q Hamartin – tumor suppressor TSC2 on Chromosome 16q Tuberin – tumor suppressor 1/6000-9000 have gene 1/150,000 - full expression of gene Carriers usually only have Ash-leaf macule Major Features Facial angiofibromas (adenoma sebaceum) Nontraumatic ungual fibroma Hypomelanotic macules (Ash leaf spots) Shagreen patch (connective tissue nevus) Multiple retinal nodular hamartomas Cortical tuber Subependymal nodule Subependymal giant cell astrocytoma Cardiac rhabdomyoma Renal angiomyolipoma Lymphangiomyomatosis Minor Features Multiple randomly distributed pits in dental enamel Hamartomatous rectal polyps Bone cysts Cerebral white matter radial migration lines Gingival fibromas Nonrenal hamartoma Retinal achromatic patch “confetti” skin lesions Multiple renal cysts Diagnostic Criteria for Tuberous Sclerosis Definite 2 Major Features 1 Major and 2 Minor Features Probable One Major + One Minor Feature Possible One Major Feature 2 or more Minor Features Sturge – Weber Syndrome Vascular Malformation over the face covering ophthalmic cutaneous distribution of CN V Port wine stain to forehead and upper eyelid Pink – purple and present at birth Sturge – Weber Syndrome Ipsilateral leptomeningeal angiomatosis with intracranial calcifications Seen on CT scan (though often normal at birth) Seizures in 90% Sturge – Weber Syndrome High incidence of mental retardation Cognitive and behavioral problems Ipsilateral ocular complications Buphthalmos – corneal enlargement Colobloma Glaucoma Klippel-Trenaunay Syndrome Port-wine stain over lateral aspect of the leg (arm) Bilateral is rare Underlying vascular lesion increases blood supply hemihypertrophy and lymphedema Ataxia - Telangiectasia Autosomal Recessive Degenerative Ataxia – cerebellar degeneration Oculocutaneous Telangiectasia – seen by age 6 Immunodeficiency Deficient cellular immunity , low IgA and IgM Recurrent sinopulmonary infections Neoplasia ALL or lymphoma Ataxia Stereotypic Progression Infant – tremors of head Toddler- unsteady gait School age child – global ataxia and scanning, slurred, dysarthric speech By 10 yo – loss of deep tendon reflexes, impared position and vibratory sense Adolescence – choreoathetosis, dystonic posturing, gaze apraxia, progressive dementia Linear Sebaceous Nevus Present at birth Can be anywhere Yellow – tan waxy linear lesion Excess of pappillomatous sebaceous glands 15-20% risk of malignant degeneration Association with seizure and mental retardation CNS Malformations Macrocephaly > 2 standard deviations above the mean head circumference for age, gender, gestation Causes Hydrocephalus Intracranial mass Thickening of the skull Megalencephaly – increased brain substance Evaluation Series of measurements of head circumference Measurement of parental head circumference Developmental history Family history CT or MRI- assessment of ventricular size, intracranial masses, chronic subdural effusions, calcifications, blood Hydrocephalus Imbalance between CSF production and resorption that results in a significant net accumulation of fluid in the ventricular system Choroid plexus papilloma – CSF overproduction Non-communicating Hydrocephalus Obstruction of CSF pathways within the ventricular system Aqueductal Stenosis, tumors of posterior fossa, other congenital malformations Communicating Hydrocephalus Obstruction of CSF pathways in the subarachnoid space Intracranial hemorrhage, meningitis Clinical Manifestations of Hydrocephalus Excessively large head at birth OR rapidly growing Forehead is disproportionately large Face appears small Scalp is thin with distended veins Anterior fontanelle - large and tense Sutures split Ocular findings Impaired upward gaze Sunsetting sign Divergent strabismus Abducens nerve paresis Hydrocephalus Dandy-Walker Malformation Progressive cystic enlargement of the fourth ventricle Enlarged posterior fossa Upward displacement of the tentorium and transverse sinuses Hydrocephalus – universal 60% with increased ICP by age 2 Bulging occiput, posterior fossa cyst Ataxia, nystagmus, cranial nerve deficits Dandy-Walker Malformation Hydrancephaly Characteristics Absence of cerebral hemispheres Intact meninges Normal skull Appear normal at birth First few weeks Developmental arrest, hypertonia, hyperreflexic Seizures Die between 6-12 months Hydrancephaly Pictures Microcephaly Head circumference more than 2 standard deviations less than the mean for gender, age, gestation Neurologic manifestations Minor Motor skills, mild MR Major Vegetative state Diagnostic evaluation Family, prenatal history Karyotype Inborn error of metabolism Serologic studies for TORCH infections Imaging Causes of Microcephaly Genetic defects Trisomies Deletions Translocations Antenatal Irradiation Intrauterine infections Rubella CMV Toxoplasmosis Congenital syphilis HSV Exposure to drugs or chemicals during gestation Fetal alcohol syndrome Phenytoin exposure Trimethadione exposure Methyl mercury exposure Maternal PKU Perinatal Insults Trauma Anoxic Metabolic infectious Microcephaly Midline Defects/ Occult Spinal Dysraphism Midline spinal cord and vertebral skeletal defects Encephalocele Defective closure of caudal portion of neural tube Myelomeningocele spina bifida occulta Occult Spinal Dysraphism Cutaneous/subcutaneous defects Hairy patch Lipoma Skin tag Port-wine stain Hemangioma Sacral dimples Radiologic Screening for Cutaneous Stigmata Ultrasound Vertebrae do not ossify until 3 months Can assess cord motion MRI Neurosurgery referral Early intervention can prevent progression of defects Clinical Symptoms Symptom-free interval 3 years- school age (periods of rapid growth) Leg stiffness Clumsiness Weakness/numbness Bowel/bladder dysfunction Physical exam Decreased tone Decreased reflexes Decreased sensation Foot deformities Pictures