Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Hepatitis B wikipedia , lookup
Anaerobic infection wikipedia , lookup
Oesophagostomum wikipedia , lookup
Clostridium difficile infection wikipedia , lookup
Gastroenteritis wikipedia , lookup
Neonatal infection wikipedia , lookup
Carbapenem-resistant enterobacteriaceae wikipedia , lookup
Hospital-acquired infection wikipedia , lookup
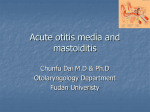
GUIDELINES Guidelines l Upper Respiratory Tract Infections Nadine Butler, MPharm, PhD School of Pharmacy, University of the Western Cape Introduction The most important concern in the management of upper respiratory tract infections (URTIs) is antibiotic resistance. Worldwide evidence suggests that inappropriate antibiotic use for non-severe URTIs, most of which are viral, adds to the overall burden of antibiotic resistance, a phenomenon which is becoming more prevalent.1 This has been the rationale for the compilation of treatment guidelines for the management of URTIs in South Africa. The initial guideline was drawn up following a meeting of the Infectious Diseases Society of Southern Africa in 2003; at this meeting randomised controlled trials, existing URTI treatment guidelines and local antibiotic resistance patterns were examined, culminating in the publication of a consensus document in 2004.2 The same group, including overseas experts, decided in 2008 to update the guideline (published in 2009), which incorporates the following newly available information: •• The introduction of new antibiotics (e.g. gemifloxacin) or new formulations of existing antibiotics (e.g. amoxicillin/ clavulanic acid) •• Trends in antibiotic pharmacokinetic/pharmacodynamic parameters which impact on previous guideline recommendations •• The potential impact of the 7-valent pneumococcal conjugate vaccine on otitis media •• Acute otitis media with otorrhoea in patients with tympanostomy tubes3,4 Low-grade fever, malaise, myalgia, anorexia 46 SAPJAug10pp46-51.indd 46 The guideline specifies first-line antibiotic recommendations for the following conditions: •• Acute pharyngotonsilitis •• Acute otitis media •• Acute bacterial sinusitis Alternative choices of antibiotics are also recommended under one or more of the following conditions: •• Allergy or intolerance to first-line agents •• Recent prior use of first-line agents •• High-risk cases likely or known to be infected with highly resistant organisms (usually ß-lactam and macrolide resistance) •• Failed initial therapy4 Organisms responsible for URTIS Although the term URTI implies a problem located in the upper airways, it is inevitable that both the upper and lower airways would become involved to a variable degree. The majority of URTIs are viral in origin (including the Epstein Barr virus), resulting in damage to the ciliary apparatus and mucosal epithelium. Since the nerve endings are exposed, the airway becomes sensitised to the irritational effect of inhaled substances and to secretions. The clinical symptoms of these viral infections usually resolve within two weeks, but the airway irritability may persist for six to eight weeks.5 Given the viral nature of the majority of the URTIs, it is important that the natural history of the common cold be well recognised, so that the appropriate management can be applied to any deviations from the normal progression of the disease. Figure 1: Natural history of the common cold4 Nasal stuffiness and throat irritation Sneezing and watery nasal discharge Cough in 60–80% (does not imply bacterial disease) Mucopurulent secretions (1–3 d later) Persists up to 10 days in 35% Persists up to 10 days in 31% SA Pharmaceutical Journal – August 2010 8/5/2010 10:12:25 AM GUIDELINES l Of clinical importance in the management of the common cold is the recognition that clear nasal secretions frequently become purulent; this is however not indicative of secondary bacterial infection, thus antibiotic therapy is not automatically indicated. Coughing is a normal accompaniment. Irrespective of age group, URTIs involving bacterial infection are commonly otitis media and sinusitis caused by Streptococcus pneumoniae and pharyngitis caused by Streptococcus pyogenes. Systematic reviews have suggested that using antibiotic therapy for the treatment of pharyngitis and otitis media in developed countries is only of extremely limited benefit. Good data from less developed countries, where there is a greater prevalence of rheumatic fever and suppurative complications, for example mastoiditis, is not available; therefore the doubtful antibiotic benefit cannot be extrapolated globally.6,7 In the underdeveloped rural parts of South Africa, there is evidence of a high prevalence of rheumatic fever, despite poor notification rates. Adherence to antibiotic therapy Although patient non-adherence to prescribed regimens is an important issue throughout clinical practice, the emergence of antibiotic-resistant bacteria implies that patient non-adherence, specifically to antibiotic therapy, is particularly worrying. When a patient with an URTI either delay starting their antibiotic therapy or miss one or more doses, plasma levels of the antibiotic may fall below the minimum inhibitory concentration (MIC), but remain high enough for the development of antibiotic resistance. Since experience has shown that no definitively effective measures to combat non-adherence, via changing patient behaviours, have been identified, the focus has shifted instead to simplifying antibiotic dosage regimens and assessing the comparative efficacy of short-course therapy.8 The guideline includes alternative options of short-course (3–5 days) antibiotic therapy.4 Acute pharyngotonsilitis (sore throat) Definition: Acute pharyngotonsilitis (sore throat) is an inflammatory condition of the wall of the pharynx, sometimes divided into tonsillitis and pharyngitis, most commonly caused by respiratory viruses. 5–30% of cases would be bacterial; caused by S. pyogenes, a group A ß-haemolytic streptococcus (GABHS). Non-infectious causes include allergy or exposure to irritating substances. Most cases of GABHS are self-limiting; antibiotic therapy is however indicated to prevent post-streptococcal sequelae of acute rheumatic fever or glomerulonephritis, common in poor rural and urban areas of South Africa. Evidence suggests that intramuscular (IM) penicillin prevents rheumatic fever; although this route of administration is not popular, it is preferred, particularly there is suspicion that either the patient would not adhere to the oral regimen or would not present for follow-up, if needed. The discomfort associated with the IM injection could be minimised by giving the medication at room temperature. As shown in Figure 2, penicillin is the drug of choice (given orally or IM). Amoxicillin could also be used, having the advantage of no food restrictions; the disadvantage SA Pharmaceutical Journal – August 2010 SAPJAug10pp46-51.indd 47 is that amoxicillin, when used when the infection is due to the Epstein Barr virus, could cause a rash, which could be incorrectly diagnosed as a penicillin allergy. Recommended short-course therapy for bacterial sore throat, intended to maximise patient adherence and so minimise antibiotic resistance, include the following (including the new macrolides and second-generation cephalosporins, which have been found to be equivalent in efficacy to penicillin given three times a day for 10 days): Note: regimens are for five days unless otherwise specified.4 Children: •• Amoxicillin-clavulanate, 40 mg/kg/day in three divided doses •• Azithromycin, 10–20 mg/kg once daily for three days •• Clarithromycin, 7.5 mg/kg twice daily •• Cefpodoxime, 4 mg/kg twice daily •• Cefproxil, 7.5 mg/kg twice daily •• Cefuroxime, 10 mg/kg twice daily Adults: •• Amoxicillin-clavulanate, 375 mg three times daily •• Azithromycin, 500 mg once daily for three days •• Clarithromycin (modified release), 500 mg once daily •• Cefpodoxime, 100 mg twice daily •• Cefproxil, 500 mg twice daily •• Cefuroxime, 250 mg twice daily •• Telithromycin, 800 mg once daily Acute otitis media Acute otitis media (AOM) is one of the most common childhood diseases; by the time a child has reached three years of age, it is estimated that 75% would have had more than one episode. Higher prevalence rates are recorded in children less than two years of age, attending a day-care facility and/or exposed to passive smoking.9 Typical causative bacteria for AOM are S. pneumoniae, nontypable Haemophilus influenzae and Moxarella catarrhalis. Infections caused by the last two bacteria typically show a high rate of spontaneous resolution (around 60–70%) but the S. pneumoniae infections are the least likely to resolve spontaneously, thus represent the most important target for antibiotic therapy. A particular concern in the antibiotic treatment of AOM is the poor permeability of the middle ear fluid to antibiotics and the ensuing higher risk of development of antibiotic resistance. The recommended treatment options given for AOM in Figure 3 mostly refer to the treatment of the condition in children. In adults, the treatment recommendations for AOM are exactly the same as for acute bacterial sinusitis (see Figure 4). Particularly for older infants, a recommendation has been made that antibiotic therapy for AOM should be postponed for 48 hours in favour of analgesic and decongestant treatment. The rationale for this lies in both the fact that the infection could probably be of viral origin, and in the high rates of spontaneous resolution of AOM.10 The guideline, while acknowledging that this approach is reasonable, still recommends that in South Africa, given the risks of a serious infection with S. pneumoniae and the reality that many patients would not return for follow-up after the 48hour period, that all cases of 47 8/5/2010 10:12:26 AM GUIDELINES Guidelines l Figure 2: Recommended treatment for sore throat4 SORE THROAT Clinical diagnosis of streptococcal pharyngotonsillitis Symptom cluster = Points in favour of empiric antibiotic therapy • Acute onset • Temperature > 38o • Tender anterior cervical nodes • Tonsilar erythema or exudates • Age 3–15 years • Previous rheumatic fever or rheumatic heart disease BACTERIAL INDICATIONS FOR REFERRAL Local complications: • Peritonsillar sepsis and/or asymmetric peritonsilar swelling • Recurrent infections (≥ 4 x /year) • No response to initial Tx Systemic complications: • Acute rheumatic fever • Severe systemic illness Symptom cluster = Points against empiric antibiotic therapy • Rhinorrhoea • Cough • Diarrhoea • Conjunctivitis • Age > 45 years VIRAL Treat symptomatically No empiric antibiotics indicated (unless +ve throat swab) REFER IF COMPLICATIONS OCCUR TREATMENT OF CHOICE (if no reason to refer) DRUG OF CHOICE: Penicillin Children: Oral Penicillin VK •≤ 27 kg: 250mg bd, x10d (30 min before meals) •> 27 kg: 500mg bd, x10d (30 min before meals) OR Intramuscular Benzathine penicillin; •3–5 yrs: 600 000 U •> 5 yrs: 1,2 MU Adults and adolescents: • Oral: 500mg Pen VK bd, 10d OR • IM: 1,2 MU benzathine penicillin OR • IM: 900 000 U benzathine penicillin PLUS 300 00 U procaine penicillin ALTERNATIVE TREATMENTS PATIENTS with SEVERE BETA LACTAM ALLERGY Children: •Erythromycin estolate, 40 mg/kg bd, x 10d •Azithromycin, 10–20 mg/kg once daily, x 3d •Clarithromycin, 7.5–15 mg/kg bd, x 5d Adults: •Erythromycin estolate, 500 mg bd, x 10d •Azithromycin, 500 mg once daily, x 3d •Clarithromycin (modified release), 500 mg once daily, x 5d •Telithromycin, 800 mg once daily, x 5d SPECIAL INVESTIGATIONS Throat swabs should be reserved for patients with recurrent sore throats 48 SAPJAug10pp46-51.indd 48 SA Pharmaceutical Journal – August 2010 8/5/2010 10:12:26 AM GUIDELINES l Figure 3: Recommended treatment for acute otitis media4 ACUTE OTITIS MEDIA (AOM) Clinical diagnosis of AOM • • • Visualisation of tympanic membrane essential for diagnosis Bulging, red or yellow tympanic membrane Ancillary features include: – Otalgia – Temperature > 38o • NOTE: Effusion alone is not an indication for antibiotic therapy INDICATIONS FOR REFERRAL • • • • • If tympanic membrane not visualised Non-responsive AOM (after 3d Tx) Suspected intracranial extension Lower motor neuron VIIth nerve palsy Suspected mastoiditis TREATMENT OF CHOICE DRUG OF CHOICE: Oral amoxycillin Children: • 90 mg/kg/day in 2–3 divided doses, x 5–7d • If < 2 years, recurrent or chronic AOM or complicated cases, x 7–10d Adults: • 1000 mg tds x 5d ALTERNATIVE TREATMENTS ALTERNATIVE ANTIBIOTIC CHOICES Children: • Amoxicillin-clavulanate, plus additional amoxicillin (to a total dose of amoxicillin 90 mg/kg/day in 2–3 divided doses, x 5–7d) • Cefpodoxime proxetil, 8–16 mg/kg bd, x 5–7d • Cefproxil, 15–30 mg/kg, bd, x 5–7d • Cefuroxime axetil, 15–30 mg/kg bd, x 5–7d PATIENTS with SEVERE BETA LACTAM ALLERGY Children: • Erythromycin estolate, 40 mg/kg bd, x 5–7d • Azithromycin, 10 mg/kg once daily, x 3d • Clarithromycin, 7.5–15 mg/kg bd, x 5–7d • Cefpodoxime proxetil, Cefproxil, Cefuroxime axetil. As above FAILED THERAPY Children: • Amoxicillin-clavulanate, plus additional amoxicillin (to a total dose of amoxi cillin 90 mg/kg/day in 2–3 divided doses, x 5–7d) for failed therapy with amoxicillin alone • Ceftriazone, IV or IM, 50–75 mg/kg once daily x 3d. (Also recommended for known high-level antibiotic resistance) SPECIAL INVESTIGATIONS None recommended SA Pharmaceutical Journal – August 2010 SAPJAug10pp46-51.indd 49 definitively diagnosed AOM be initiated on antibiotic treatment immediately. Of importance here is the diagnosis; the AOM must be differentiated from otitis media with effusion (glue ear). Antibiotic therapy is considered essential in the following patients: •• Recurrent AOM •• Immunocompromised •• Neonates •• Structural ENT or immunological abnormalities •• Fever (temperature > 38o) or pain > 48 hours •• Day-care attendees or their siblings. Paracetamol (10–15 mg/kg 4–6 hourly) or ibuprofen (10 mg/kg 8 hourly) are recommended for pain. The use of decongestants in the treatment of AOM is controversial. If used, topical administration for not more than three days is preferred to the oral route. An addition to the current guideline is information pertaining to the treatment of acute otitis media in patients with tympanostomy tubes (AOMT). This has not previously been considered as a separate clinical entity in the treatment of URTIs. It has been found that, unlike AOM, the otorrhoea fluid is likely to contain other bacteria – Psuedomonas aeruginosa or S. aureus – in addition to the usual pathogens. The recommended treatment is ciprofloxacin 0.3%/ dexamethasone 0.1% otic suspension, four drops twice daily for seven days. In addition to the installation of the eardrops, it is recommended that the external ear canal/s be suctioned, using a disposable nasal aspirator, prior to use of the drops. Tragal (on the cartilage projection anterior to the external opening of the ear) pressure should be applied after the drops are instilled in order to push the drops through the tympanostomy tubes into the middle ear. Acute bacterial sinusitis Acute bacterial sinusitis (ABS) is commonly preceded by a viral URTI. Inflammation of the nose and paranasal sinuses, caused by allergy, trauma or dental infection, typically predispose patients to ABS. ABS is similar to AOM in terms of the typical causative bacteria and in terms of S. pneumoniae being most problematic, thus occasioning antibiotic therapy. Other streptococcal species, anaerobic bacteria and S. aureus occur in a small percentage of cases. Atypical pathogens, for example Chlamydia pneumonia or even fungi, have been known to be the causative organisms.r References 1. Jacobs MR. World trends in antimicrobial resistance among common respiratory tract pathogens in children. Pediatr Infect Dis J 2003; 22: S109 – s119. 2. Working Group of the Infectious Diseases Society of Southern Africa. Guideline for the management of upper respiratory tract infections. SAMJ 2004: 94(6):475–483. 3. Editorial. Revised guideline for the management of upper respiratory tract infections. South Afr J Epidemiol Infect. 2008;23(4):3. 4. Working Group of the Infectious Diseases Society of Southern Africa. Updated guideline for the management of upper respiratory tract infections in South Africa:2008. SA Fam Pract. 2009: 51(2):105–114. 5. Bösenberg AT. The child with a runny nose! Upper respiratory tract infection in children: the impact on anesthesia. SAJAA 2007;13(2):33–35. 6. Del Mar C. Managing sore throat: a literature review. Med J Aust 1992;156: 572–575. 7. Del Mar CB, Glasziou PP, Spinks AB. Antibiotics for sore throat (Cochrane Review). In: The Cochrane Library, Issue 4, 2003. Chichester, UK: John Wiley & Sons, 2003. 8. Jones S. Respiratory tract infections and high-dose short-course antibiotic therapy. SA Pharm J.2009; Apr: 26–28. 9. Hoppe HL, Johnson CE. Otitis media: focus on antimicrobial resistance and new treatment options. Am J Health Syst Pharm 1998;55(18):1881–1897. 10. Del Mar C, Glasziou P, Hayem M. Are antibiotics indicated as initial treatment for children with acute otitis media? A meta-analysis. BMJ 1997;314: 1526–1529. 49 8/5/2010 10:12:27 AM Guidelines GUIDELINES l Figure 4: Recommended treatment for acute bacterial sinusitis4 ACUTE BACTERIAL SINUSITUS (ABS) Clinical diagnosis of ABS ALTERNATIVE TREATMENTS Consider in adults or children with an URTI that is NOT improving after 10d OR worsens after 5–7d and is accompanied by some or all of the following symptoms: • Fever • Facial tenderness, particularly unilateral or focused in the region of a sinus group – Peri-orbital – Maxillary – Frontal – Ethmoidal • Dental tenderness • Nasal discharge, nasal congestion, anosmia (loss of sense of smell), cough, ear fullness and pressure ALTERNATIVE ANTIBIOTIC CHOICES NOTE: Frontal sinusitis does not occur in toddlers < 4 years because of delayed development of the frontal sinuses PATIENTS with SEVERE BETA LACTAM ALLERGY INDICATIONS FOR REFERRAL • • • • • Non-responsive ABS (after 72 hr Tx) Peri-orbital swelling Evidence of CNS extension (meningism, focal neurological signs, altered level of conciousness) Suspected systemic illness Chronic sinusitis – symptomatic for > 30d TREATMENT OF CHOICE DRUG OF CHOICE: Oral amoxicillin Children: • 90 mg/kg/day in 2–3 divided doses, x 10d Adults: • 1000 mg tds, x 10d 50 SAPJAug10pp46-51.indd 50 Children: • Amoxicillin-clavulanate, plus additional amoxicillin (to a total dose of amoxicillin 90 mg/kg/day) in 2–3 divided doses, x 10d • Cefpodoxime proxetil, 8–16 mg/kg bd, x 10d • Cefuroxime axetil, 15–30 mg/kg bd, x 10d Adults: • Amoxicillin-clavulanate, 1 g bd plus amoxicillin 500 mg OR 2 g sustained release (SR) bd x10d • Cefpodoxime proxetil, 200–400 mg bd, x 10d • Cefuoxime axetil, 500 mg – 1 g bd, x 10d Children: • Erythromycin estolate, 40 mg/kg bd, x 10d • Azithromycin, 10 mg/kg once daily, x 3d • Clarithromycin, 7.5–15 mg/kg bd, x 10d • Cefpodoxime proxetil, Cefuroxime axetil. As above Adults: • Erythromycin, 500 mg qid, x 10d • Azithromycin, 500 mg once daily, x 3d • Clarithromycin (modified release), 1g once daily, x10d • Telithromycin, 800 mg once daily, x 5–10d • Gemifloxacin, 320 mg daily, x 5–10d • Levofloxacin, 500 mg bd or 750 mg once daily, x 5–10d • Moxifloxicin, 400 mg once daily, x 5-10d • Clindamycin, 450 mg tds, x10d • Cefpodoxime proxetil, Cefuroxime axetil. As above FAILED INITIAL THERAPY Children: • Amoxicillin-clavulanate, plus additional amoxicillin (to a total dose of amoxycillin 90 mg/kg/day) in 2–3 divided doses, x 10d – for failed therapy with amoxicillin alone • Ceftriazone, IV or IM, 50–75 mg/kg once daily, x 3–5 days. Also recommended for known high-level antibiotic resistance Adults: • Amoxicillin-clavulanate, 1g plus additional amoxicillin 500 mg, bd OR 2 g SR, x 10d – for failed therapy with amoxicillin alone • Gemifloxacin, levofloxacin, moxifloxacin, telithromycin As above • Cefriazone, IV or IM, 1–2 g once daily for 3–5 d SPECIAL INVESTIGATIONS • • • • X-rays are of limited value CT scans should be reserved for cases in which surgery is considered Nasal swabs for microbiological investigation are of no value Specimens for culture and microscopy should be collected from sinus puncture SA Pharmaceutical Journal – August 2010 8/5/2010 10:12:27 AM