Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
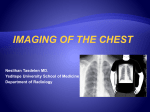
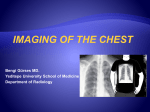
CXR Chest X Ray Tutorial The Retro look This tutorial was created by Dr I Runcie, Princess Royal Hospital, Haywards Heath. It was originally created in 1993 in HyperCard which was just about the first programme to effectively use text hyperlinks. It was monochrome in ‘93 and used the metaphor of file cards rather than slides. The look of the original has been retained along with the rather crude diagrams, poorly reproduced films (digital camera on a viewing box!) and ancient references. Originally the films were separate but they were later photographed and incorporated. The films were everyday examples, some were copies and one is badly scratched. The tutorial is interpretation orientated rather than disease orientated. It was designed for use by anaesthetists but others may find it useful. The lateral features heavily but this is, of course, now largely replaced by CT. Contents basics collapse basics Chest X Ray Tutorial Pulmonary shadows Disease in the different anatomical divisions of the lung give rise to different appearances and it is necessary to distinguish between Interstitial change, air space shadowing (often called consolidation) and pleural abnormalities. All of these frequently co-exist, as in pneumonia & LVF but one type of shadowing will usually dominate. It is then necessary to match up the clinical history with the type and distribution of the shadowing. Basics Chest X Ray Tutorial A PA view is preferable to a AP view because the lung fields are less obscured by the magnified heart and by the projected scapulae. The further away the source the more these advantages will apply. A portable film will always be AP with a short tube- film distance. Basics Chest X Ray Tutorial Take a look at the films Basics Chest X Ray Tutorial Film 1 is PA and film 2 is a AP view of the same patient. Note the difference in the size and shape of the heart shadow and the position of the scapulae. In clinical practice you cannot be sure of the projection unless the radiographer has marked the film. All portable films will be AP. Basics Chest X Ray Tutorial Basics Centring is checked by comparing the medial end of the clavicles with the spinous processes (see inset). As a rule the side to which the patient is rotated becomes more translucent (black). But there are frequent exceptions, often due to failure of precise lateral centering which can give a false impression of rotation. The great majority of cases of unilateral hypertransradient lung are due to technical factors. (ref. Joseph et al Clinical Radiology 1978 29 125-131 ) Film 3 Film 4 Chest X Ray Tutorial Basics Films 3 & 4 are of the same patient. Film 3 is rotated and there is a difference between the distances between the clavicles compared with the spinous process of T3. The distance on the right side is 4 cms and on the left 2.2 cms. There was a minimal difference in density between the two sides on the original film, but this is not easy to see on your copy films. Note therefore that quite noticeable degrees of rotation are required to produce significant changes. Film 4 is very rotated and even on the copy films the left lung appears darker. The left clavicle has rotated so far to the right that it is overlying the spinous process. This film therefore demonstrates that the side to which the patient is rotated becomes hypertransradient. If a film demonstrates the opposite situation there is probably some pathology present. For a technical explanation see Joseph et al Clinical Radiology 1978 29 125-131. Below is an enlargement of film 4. The arrows point to the medial ends of the clavicles Chest X Ray Tutorial Basics Looking at the film Everyone should develop their own system. I leave the lung fields until last. The bones come first, from outside in, ie humeri and scapulae, then the ribs. I look at the posterior ends of the ribs remembering to look straight through the heart to where the ribs meet the spine. I run my eyes down each chest wall and then view the anterior end of each rib. As I do all this I am comparing the two sides. Many radiologists prefer to examine each rib as a whole. The soft tissues come next ie the mediastinal shadows and the diaphragm. Then the lung fields, comparing the two sides by mentally dividing them into; upper, mid and lower zones and looking; rt upper, lft. upper, rt. mid etc. Finally I go back to the difficult areas ; apices, costophrenic angles, hila and through the the heart. There is a lot of lung behind the heart. Try looking at some of the previous films again. Anatomy Chest X Ray Tutorial Anatomy 1 Consideration of the secondary pulmonary lobule assists interpretation of the various types of lung shadowing. This is an area of lung surrounded to a variable extent by a connective tissue septum (CTS). Thickening of the CTS produces the honeycombing pattern of some interstitial diseases. The lobules vary in size from 1.2 to 2.5 cms. (for key see following cards.) Basics Secondary Pulmonary Nodule Chest X Ray Tutorial Pulmonary veins and lymphatics (v+l) run within the CTS and engorgement produces the interstitial changes seen in oedema. The acinus (ac) (5-6 mm) arises from the terminal bronchiole (tb) and tends to act as a pathological unit. It is rare for only part of an acinus to be consolidated. Consolidated acini adjacent to non consolidated ones give rise to the "fluffy" appearances at the edge of an area of air space shadowing. Basics Secondary Pulmonary Nodule Chest X Ray Tutorial The primary lobule arises from the last respiratory bronchiole (rb) and appears similar to the terminal respiratory unit (tru) mentioned in some anaesthetic text books. art=pulm. artery (travel with bronchial tree) ven= venules pok= pores of Kohn ad=alveolar duct alv=alveolus Basics Secondary Pulmonary Nodule Chest X Ray Tutorial Knowledge of the anatomy as seen on the 'lateral' is the key to accurate interpretation of the frontal view. Note the position of the fissures. It is worthwhile persevering with the next 5 cards in order to gain an understanding of principles which will allow a logical approach to interpretation of difficult films. Basics spine spine Chest X Ray Tutorial A Normal PA and lateral. Think about the position of the various lobes and segments. Basics Chest X Ray Tutorial On the lateral note that the lung is darkest posteriorly just above the diaphragm.If this is not the case there is probably some basal pathology. Note also the position of the two oblique fissures running from about T6 posteriorly to almost the anterior end of the diaphragm just behind the main bulk of the hila in the centre of the film. Note the shadows of the humeri, glenoids and scapulae which can occasionally be misinterpreted. The scapulae can be seen running downwards just anterior to the vertebral bodies. Look at the diaphragms. Note that you can see almost the whole length of them but not the anterior end of one of them. -Why not and which diaphragm is it? What is the nearly vertical line coming upwards from the middle of the lower diaphragm? Yes its the IVC- but why cant you see the front of it? You will be able to work all of this out if you read on Basics Chest X Ray Tutorial To help you. 1. oblique fissure 2. humerus 3. soft tissue of arm 4. scapulae 5. IVC Basics Chest X Ray Tutorial On the frontal view segments overlap and their positions only become clear when they are consolidated. Basics Chest X Ray Tutorial Film 7 shows consolidation adjacent to the upper left heart border but the heart border remains visible. This means that the consolidation must be posterior. Now look at the next card. Basics Chest X Ray Tutorial The lateral view shows the consolidation to be very posterior, overlying the vertebral bodies . The consolidated segment is below the level of the horizontal fissure, which can just be made out, and therefore must be in the apical segment of the lower lobe. If it were above the oblique fissure it would be in the posterior segment of the upper lobe. Sorry about the scratch. Basics Film 7A silhouette sign Chest X Ray Tutorial Basics The silhouette sign Described by Benjamin Felson this observation was a revelation at the time although it now seems obvious. He observed that the reason that the borders of the mediasinum and the diaphragm are seen on the CXR is that there is air alongside them. Compare this with the viscera on an abdominal film which are just not identified except for those outlined by fat. The inside of the bowel wall may be outlined by the gas in the lumen, but only if there is a large pneumoperitoneum is the outside of the bowel wall seen. Note that not all of the diaphragm is seen on the CXR. The part touching the heart is not visible, either on the frontal view or on the lateral. (This is the best way to identify which hemi- diaphragm is which on the lateral). Another example is a cardiophrenic fat pad which may obscure the heart border and mimic consolidation. The silhouette sign can be used to identify and localise consolidation and masses without a lateral view. Obliteration of the heart border will be due to opacification of the middle lobe on the right and the lingula on the left. Conversely, consolidation seen through the heart but with the heart borders visible will be in the posterior segments. ref. Felson "Chest roentgenology"W. B. Saunders 1973 Chest X Ray Tutorial Basics Films 8 & 8a Film 8 shows consolidation bounded above by the horizontal fissure but without loss of the right heart border.The lateral 8A shows consolidation adjacent to the heart. Try to work this out before clicking here to see the answer. The consolidation is only in the lateral segment of the middle lobe which is not in contact with the heart border. Chest X Ray Tutorial Basics Oblique fissure Examples of the sillhouette sign as applied to the lateral. Consolidation seen above the hilum on the PA view without obliteration of the mediastinal border may be in the apical segment of the lower lobe (point Y on the diagram) or in the posterior segment of the upper lobe (Point X) heart consolidation Rt diaphragm lost posteriorly due to contact with consolidated posterior basal segment Left diaphragm lost anteriorly due to contact with the heart. Rt diaphragm is seen through the heart shadow as it is in contact with air. Chest X Ray Tutorial Basics Film 9 Film 9 shows consolidation in the rt. mid zone. It was on both sides of the horizontal fissure and therefore not in the anterior segment of the upper lobe or the middle lobe. It could be in the apical segment of the lower lobe or the posterior segment of the upper lobe. Film 9A shows it to be in the upper lobe, bounded inferiorly by the horizontal fissure. Consolidation in the apical lower would be bounded superiorly by the fissure. Film 9A Chest X Ray Tutorial Basics The silhouette sign 3 The aortic knuckle lies alongside the apicoposterior seg. of the left upper lobe and is therefore lost when this area is opacified. The 'apex' of the lung lies posteriorly and masses which are clearly defined above the level of the clavicle must lie posteriorly. An anterior mass above the clavicle, in contact with soft tissue, may be seen as an increased density but will not be well defined. Film 10 is slightly rotated to the left. There is an apparent mass to the left of the trachea above the medial end of the clavicle. This is due to tortuous vessels made more prominent by the rotation. That the shadow is anterior is evidenced by the lack of a definable lateral edge. Film 10 Chest X Ray Tutorial Basics Film 10A is a more striking example. The lateral border of the tortuous vessels on the right is well seen inferiorly but suddenly disapears superiorly, just above the clavicle, where they are no longer in contact with lung. A similar but less obvious appearance is seen on the left. Film 10A Chest X Ray Tutorial Basics 10 B shows a mass situated more posteriorly on the right.Above the clavicle the edge of the mass could just be made out against the lung. The appearances in this case are subtle and it is possible to see posterior masses much more clearly outlined in the apex than this, but life (and radiology) is not always simple. By now it should not be necessary for me to point out the secondary deposit. Film 10B Chest X Ray Tutorial Basics Well all right then. It’s here Film 10B Collapse Chest X Ray Tutorial Collapse Collapse or atelectasis is reduction in volume of an area of lung. The signs of lobar or segmental collapse are discussed under three categories. 1. Changes in densityA. The collapsing area may appear more dense due to approximation of the vessels within it. This is usually only seen when there is considerable loss of volume. B. There may be compensatory emphysema in the surrounding lung. 2. Changes in position- the hilum & mediastinum may shift towards the side of the collapse. Fissures show characteristic movement depending on which lobe is involved. 3. The silhouette sign may apply to borders adjacent to collapsed airless lung. Consideration of the lateral is the keyto understanding collapse Chest X Ray Tutorial The following descriptions are of classical lobar collapse. Actually this hardly ever happens. There is usually some associated consolidation or preexisting disease which alter appearances. Lung fibrosis particularly restricts the movement of fissures etc. Knowledge of the classical appearances are a guide to interpretation in practice. Total collapse of a lung gives a whiteout on the affected side due to the mediastinum and hemidiaphragm moving over to fill the spac. Ribs on the affected side move closer together. The other lung shows compensatory emphysema and may "herniate' across the midline anteriorly. Compensatory emphysema is usually identified by increased spaces between vessels rather than an obvious decrese in density. Ref ‘Pulmonary collapse’ Seminars in Roentgenology 1980 Vol 15 Collapse Other causes of unilateral whiteout causes signs pneumonectomy sternal clips or deformed or missing ribs. conslidation central mediastinum pleural effusion mediastinum may be shifted (massive) away (but beware of associated collapse) Chest X Ray Tutorial Rt. upper lobe collapse The horizontal fissure pivots on the hilum. Its lateral end moesg upwards and medially and its anterior end moves upwards. The upper half of the oblique fissure moves anteriorly and, in severe collapse, the two meet up against the superior mediastinum. Cont- Collapse Chest X Ray Tutorial Rt. upper lobe collapse Signs 1.A Vessels in the Rt. upper zone (RUZ) get closer together and just before total collapse a density appears alongside the superior mediastinum. B. There may be increased lucency in the mid & lower zones (RMZ&RLZ). 2. Fissures move as shown. The trachea moves to the rt. The hilum is elevated and becomes more prominent. Tenting may occur (next) 3. In severe collapse the upper mediastinal border may be lost. Collapse Chest X Ray Tutorial Films11 & 12 (1)There is crowding of vessels in the Rt. upper lobe plus some increase in density which the lateral shows to be due to associated consolidation immediately superior to the oblique fissure in the posterior segment. The anterior segment is not consolidated. (2.)The consolidation demonstrates the anterior position of the oblique fissure. The normally positioned left fissure can be seen more posteriorly. On the PA it can be seen that the hila are at the same level. Normally the rt hilum is positioned slightly below the Lft. Collapse If they are at the same level either the rt is higher or the left is depressed. Frequently in upper lobe collapse the hilum may also be rotated so that the normal pattern of the arteries leaving the hilum is disturbed and the hilum appears to be an unusual shape. In this case there is a mass in the upper half of the hilum. Mediastinal shift and compensatory emphysema are not evident.The rt. hemi diaphragm may be elevated but comparison with previous films would be necessary to be sure. Incidentally the thoracic vertebral bodies are osteoporotic and are beginning to wedge. Chest X Ray Tutorial Tenting' of the diaphragm is usually noted as a feature of long standing upper lobe collapse or fibrosis, particularly following TB. If seen as a new feature it may be diagnostic of upper lobe collapse. It is due to the elevation of the hilum pulling on the pulmonary ligament and accessory fissures. The pulmonary ligament is a strand of fibrous tissue between the hilum and the diaphragm. Collapse Chest X Ray Tutorial film 13 shows loss of volume in the RUL, probably long standing, as evidenced by the peribronchial thickening and some emphysematous change suggesting chronic airways obstruction. There is also apical pleural thickening ( black arrow) by far the commonest cause of this is chronic bronchitis. The horizontal fissure (white arrow) is elevated as is the right hilum the normal position of which is lower than the left because of the anatomy of the pulmonary arteries. There is also a small tent on both hemi diaphragms. Tenting can sometimes be much more gross than this especially in cases of coarse upper zone fibrosis such as occurs in TB. Collapse Chest X Ray Tutorial Left Upper Lobe Collapse On the lateral, the oblique fissure moves bodily forwards (straight arrows) and comes to lie close to the anterior chest wall. In severe collapse the anterior part of the lobe moves backwards away from the chest wall. The lower lobe then comes over the top of the collapsed lobe (curved arrow) and comes to lie against the anterior chest wall. On the frontal view the fissure is not seen but the collapsed lung may become evident against the upper mediastinum. Collapse Chest X Ray Tutorial Left Upper Lobe Collapse 1.A On the frontal view the vessels in the LUL approximate and a density appears around the position of the aortic knuckle. On the lateral the anterior part of the chest becomes increasingly more dense. B There may be compensatory emphysema in the LLL. 2. The fissure moves as shown on the Lat. The Trachea moves to the left. As the LLL expands the diaphragm and the L hilum may elevate & tenting may occur. 3 As the lobe collapses it comes up against the aortic knuckle which lies anteriorly. As it loses air and becomes more dense the aortic knuckle disappears (silhouette sign). Collapse But when it collapses enough to retract from the anterior chest wall, the LLL comes round and lies against the knuckle which then becomes visible again. The density of the collapsed lung continues to be evident adjacent to the knuckle and the hilum. Chest X Ray Tutorial Film 14 is an excellent example of well advanced LUL collapse. The collapsed lobe is closing down onto the hilum and becoming denser causing the veil like shadowing around the hilum. Note that there is no shift of the mediastinum, trachea, hemi diaphragm or hilum. Nor is there any obvious compensatory emphysema. This is because there is no pre existing lung disease and the lower lobe is large enough and flexible enough to fill the available space. In fact it is large enough to have come round medial to and above the collapsing lobe causing the luscency around the aortic knuckle and allowing this structure to be clearly seen. Collapse Chest X Ray Tutorial Film 15 is the lateral. The oblique fissure is seen anterior to the hilar shadows and has moved bodily forwards. The luscency immediately behind the sternum may be due to the enveloping lower lobe. Collapse Chest X Ray Tutorial Rt Middle Lobe Collapse The horizontal & lower half of the oblique fissure move towards each other. The collapsed lobe comes to lie against the heart border.The horizontal fissure is the more mobile. Collapse Chest X Ray Tutorial Rt Middle Lobe Collapse signs 1 Because the lobe is small, compensatory emphysema is rarely seen. There may be a vague density against the heart border best seen on the Lateral. 2 Fissure movement as described. Best seen on the lateral. On the frontal view if the Horizontal fissure is not seen the other changes may be difficult to spot. 3 In the late stages the rt. heart border may be lost. Collapse Chest X Ray Tutorial Collapse Rt Middle Lobe Collapse 16. There is loss of the right heart border. The horizontal fissure cannot be seen. !7. The horizontal fissure and the oblique fissure have approximated to each other leaving the middle lobe as a linear density overlying the heart shadow (arrowed). Film 16 Film 17 Chest X Ray Tutorial Lower Lobe Collapse The pattern is similar on both sides. The oblique fissure moves backwards and also medially so that the fully collapsed lobe becomes a wedge of tissue lying up against the posterior mediastinum. The middle and upper lobes expand to fill the space lateral and anterior to the collapsing lobe. Collapse Chest X Ray Tutorial Lower Lobe Collapse signs 1A As the lobe moves posteriorly it becomes more and more dense on the Lat. On the AP view it may be seen as a wedge shape through the heart shadow. B Compensatory emphysema may be noted when vessel density is compared with the other side. 2 The oblique fissure moves back. On the rt the horizontal fissure moves in a similar way to RML collapse but the lung underneath it becomes less rather than more dense. There is movement of the heart shadow towards the side of the collapse and the hemidiaphragm may elevate especially if there is pre-existing lung disease limiting the compensatory emphysema. The hilum becomes depressed. Collapse PA Lat 3 The silhouette sign operates in reverse ie there is a shadow behind the heart but the heart shadow is still seen. The part of the diaphragm in contact with the dense lung may be lost (curved arrows). Chest X Ray Tutorial Lower Lobe Collapse Film 18 . 1.There is a hint of a triangular opacity behind the heart on the left. Compensatory emphysema can be identified on the left by comparing the number of vessels on the two sides. 2 The heart shadow has moved to the left. The left hilum is depressed as can be seen by the angle of the left main bronchus seen through the heart shadow. Collapse Chest X Ray Tutorial Lower Lobe Collapse Film 19 Little in the way of density change can be identified. One oblique fissure has moved backwards slightly and can be seen behind the hilum. The other can still be seen in front of the hilum. There is an excellent example of the silhouette sign. The posterior part of the left diaphragm cannot be identified although the stomach bubble shows you where it should be. Its anterior part can be identified in front of the little diaphragmatic "tent" near to the inferior insertion of the oblique fissure. The right hemi-diaphragm can be clearly seen. This must mean that there is a considerable increase in the density of the collapsing lung possibly with some associated consolidation. Collapse Chest X Ray Tutorial Lingular collapse Often involved in upper lobe collapse, but occaisionally the lingula may collapse on its own. Features are identical to RML collapse except that the horizontal fissure is not there to help you. On the frontal view the only evidence may be a subtle loss of the Lft. heart border. Collapse Chest X Ray Tutorial Plate atelectasis or Linear collapse. Areas of subsegmental collapse appearing as lines, usually horizontal, of variable thickness. Often long standing and fibrotic. May be referred to as scarring. Common. Round atelectasis Of little pathological interest and rare, but may be mistaken for a mass. An area of lung rolled up like a Swiss Roll containing rolled up vascular structures. Always touching pleura and associated with pleural thickening. About 5cm in diameter. Diagnosed by CT. Collapse Chest X Ray Tutorial Film 20 shows a vertical band shadow at the right base, film 20A taken a few days later shows that it has disappeared and was therefore an area of subsegmental collapse. Such band shadows are often horizontal. They may be associated with infection or embolus and are not uncommon in post op. patients due to poor aeration. Permanent bands are usually due to areas of fibrotic scarring. Collapse Similar shadows may be seen due to fluid filled bronchi and thickened fissures often due to pleural effusions. Ref Heitzman E. R. “The Lung. Radiologicpathologic correlation.” 1974, Mosby Pulmonary collapse ‘Seminars in Roentgenology” 1980 Vol 15