Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
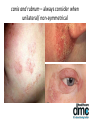
Teledermatology and One Stop Assessment and Treatment Service (OATS) Facial Rashes Dr Tony Downs FRCP Consultant Dermatologist DMC Dermatology lead clinician 020 7635 1019 [email protected] www.dmchealthcare.co.uk Facial Rashes • • • • • • • Contact dermatitis Atopic dermatitis Seborrhoeic dermatitis Discoid lupus Psoriasis Fungal infection Acne • • • • • • • Rosacea Steroid-induced rosacea Dermatomyositis SLE Erysipelas Folliculitis Other infections Seborrhoeic dermatitis • Scaly rash worse in the winter. Feels dry and sore or itchy • Affects the skin around the nose, nasiolabial fold, eyebrows, central (hairy) chest in men and scalp • Scalp variant when mild is called dandruff Seborrhoeic dermatitis • Malassezia species feed off lipids in the skin • The lipid waste products cause irritation • The mild form is called dandruff • Highly sebaceous skin areas and oily skin types are more affected • Drugs (e.g. anti-epileptics) or conditions (e.g. Parkinsonism or CVA) that increase sebum production can aggravate or precipitate the disease • Immuno-suppressed states (e.g. drugs, HIV, old age) can favour Malassezia and promote the disease Treatments for Seborrheic Dermatitis • • • • • • • 1% Hydrocortisone Ketoconazole cream and/or shampoo Daktacort cream or ointment Eumovate cream or ointment 0.1% tacrolimus ointment Short courses of topical mometasone 2% Sulphur in 1% HC cream Complications • HIV patients often are more treatment resistant. Consider HIV test if status not know • Rosacea often seen together with seb dermatitis. Rosacea makes the skin sensitive and so can be aggravated by treatments to control the seb dermatitis • Psoriasis often seen together with seb dermatitis, which can alter the appearance and require addition treatment directed at the psoriasis Facial psoriasis • Virtually always associated with scalp psoriasis • Commoner in children • Like in flexural psoriasis, treatment products can irritate • High DLQI scores Treatment options First line Mild topical steroids Tacalcitol or calcitriol ointment Second line 0.1% tacrolimus ointment Mometasone ointment or cream Hair Margin Dithrocream® Dovobet® gel 0.1% tacrolimus ointment • Off-label 0.1% tacrolimus very effective for facial psoriasis in adults or children • May cause stinging for first two weeks • Theoretical but unproven risk of increased incidence of skin infections or skin cancers Acne Pathogenesis of Acne Pathogenesis of Acne 1. Androgen mediated increased sebum production Pathogenesis of Acne 2. Early inflammation and micro-comedone formation 1. Androgen mediated increased sebum production Pathogenesis of Acne 2. Early inflammation and micro-comedone formation 3. P. acnes colonisation of follicle 1. Androgen mediated increased sebum production Pathogenesis of Acne 2. Early inflammation and micro-comedone formation 4. Late inflammation +++ 3. P. acnes colonisation of follicle 1. Androgen mediated increased sebum production Actions of Anti-Acne Therapies Actions of Anti-Acne Therapies Topical retinoids: Normalize desquamation Reduce inflammatory response Actions of Anti-Acne Therapies Topical retinoids: Normalize desquamation Reduce inflammatory response Antibiotics: Kill microorganisms Reduce inflammatory response Actions of Anti-Acne Therapies Topical retinoids: Normalize desquamation Reduce inflammatory response Antibiotics: Kill microorganisms Reduce inflammatory response Benzoyl peroxide: Kills microorganisms Actions of Anti-Acne Therapies Topical retinoids: Normalize desquamation Reduce inflammatory response Antibiotics: Kill microorganisms Reduce inflammatory response Benzoyl peroxide: Kills microorganisms Hormones: Reduce sebum production Actions of Anti-Acne Therapies Topical retinoids: Normalize desquamation Reduce inflammatory response Antibiotics: Kill microorganisms Reduce inflammatory response Benzoyl peroxide: Kills microorganisms Oral Isotretinoin: Reduces sebum Normalizes desquamation Inhibits P acnes Reduces inflammatory response Hormones: Reduce sebum production Clinical features • • • • • • Blackheads (closed comedones) Whiteheads (open comedones) Inflammatory pustules and papules Inflammatory cysts Acne scars Post-inflammatory hyperpigmentation Acne • Peaks at the age of 19yrs old • Effects the face, upper chest, back and upper arms • Can cause severe psychological trauma leading to depression and a withdrawn personality • Impacts on career choices and job opportunities Treatments • Self-med benzoyl peroxide (BPO) • Prescription topical antibiotics, BPO, retinoids, alazeic acid, nicotinamide and combination products • Prescription anti-androgens (for females) • Prescription oral antibiotics • Dermatology consultant only isotretinoin Resistance of P. acnes to antibiotics 62% 49% 38% 20% 20% 1978 USA Crawford 1988 UK Eady 1993 UK Eady 1995 UK Jones 1996 UK Jones E.C.T E.C.T. E.T.D.Tr. E.C.T. E.C.T. 0% 1976 USA Leyden E= Erythromycin C= Clindamycin D= Doxycycline Tr= Trimethoprim T= Tetracyclines Eady EA. Dermatology. 1998;196:59-66. Topical antibiotics • Should not be prescribed in isolation • No evidence that the addition of zinc (eg Zyneryt® lotion) reduces or avoids antibiotic resistance • Evidence that bacteria other than P acnes are acquiring antibiotic resistance with the use of topical and oral antibiotics used in acne Oral Antibiotics Commonly prescribed • Tetracyclines • Erythromycin • Clarithromycin • Trimethoprim Advice • 3 to 6 month courses. Expect 20% improvement at 2 mths • No advantage of one tetracycline over another • Minocycline side-effects outweigh its usefulness • Never prescribe in isolation (monotherapy) • Always prescribe with a nonantibiotic topical to avoid or reduce antibiotic resistance Combination topical therapies • Major advantages over single agents – Better compliance – Treat different stages of pathogenesis – More effective than single agents • Duac®gel twice a day- Clindamycin and BPO (slows antibiotic resistance) • Epiduo® gel daily- Adapalene and BPO (no antibiotic resistance issues) • Treclin®gel daily- Tretinoin and Clindamycin (no effect on preventing antibiotic resistance) • Isotrexin® gel twice a day – Isotretinoin and Erythromycin (no effect on preventing antibiotic resistance) Combination Therapies • Benzoyl peroxide slows the development of P acnes drug resistance • If possible oral or topical antibiotics should be combined with BPO • Beware using different topical products that are not compatible Combinations • Apply topical treatment to whole area prone to acne, not just to the spots • If mixed lesions: – Anti-comedonal therapy at night – Anti-inflammatory therapy in the mornings Topical Retinoids • Should be first line after BPO • Can cause irritation which improves with regular use or initial intermittent use • Use a sunscreen during the day and apply at night • Adapelene less irritant than tretinoin • Avoid in pregnancy but contraception not required • Helpful in resolving acne-induced post-inflammatory hyperpigmentation 20% Alezaic acid • May cause skin irritation • Useful to help resolve acne-induced postinflammatory hyperpigmentation in darker skin types • Anti-bacterial so a BPO alternative Nicotinamide gel • Topical Vit B3 preparation with antiinflammatory effects • Apply twice a day • Can cause skin irritation Benzoyl Peroxide (BPO) • Self-med or on prescription • 2.5%, 5% gels and 10% washes • Ideally used a first line agent for mild to moderate acne • Anti-inflammatory and anti-microbial • Hampered by skin irritation & bleaching of clothes Anti-androgens • Progesterone only and COCs can flare acne • Contraceptive pills that contain synthetic progesterone eg Yasmin® and Loesterin® • Dianette® contraceptive pill and spironolactone (off-label) are both potent anti-androgens. In women, these both work well at controlling acne Isotretinoin • Isotretinoin is the only currently available cure for acne with very high success rates • Sometimes more than one course is required • Post treatment with a topical retinoid can prevent acne relapse • A single course is for 4-6 mths and must be completed or the acne will relapse • The mode of action at preventing relapse remains unknown Indications for referral for isotretinoin • Failure to respond to oral & topical treatments • Chronic acne • Severe acne • Acne where scarring is beginning to develop or is established • Acne where post-inflammatory hyperpigmentation is beginning to develop or is established Light & laser based inflammatory acne treatments • For mild to moderate acne, these can work • Usually provided outside the NHS because of a lack of robust clinical efficacy and cost-benefit Light & laser based post-acne scar and pigmentation treatments • A number of cosmetic and surgical treatments can improve acne scarring and postinflammatory hyperpigmentation • Access as an NHS patient is not always possible • Dermatologists that special in laser treatments would be regarded as the doctor of choice to treat these patient Irritant Dermatitis • Acute • Cumulative • All depends on length or frequency of exposure & skin barrier function Steroid-induced rosacea • Caused by a moderate or potent topical steroid on the face • Stopping the steroid usually worsens the rash • Treat with an 8 week course of an oral tetracycline as well as stopping the topical steroid Facial fungal infections • Tinea faciei (uncommon in adults) • Tinea barbae (often presents as kerion) • Trichophyton rubrum – from other humans or the feet • Microsporum canis – from cats or dogs • Trychophyton verrucosum – from cattle • Trychophyton mentagrophytes – from horses canis and rubrum – always consider when unilateral/ non-symmetrical Treatment • Topical anti-fungal (eg ketoconazole) may be sufficient, but in widespread disease oral itraconazole or terbenafine is more appropriate and effective • Mycology scrapping prior to treatment should be taken to confirm disease, confirm treatment sensitivities and for public health monitoring of different species Kerion • Inflamed & swollen with lymphadenopathy • Can lead to scarring and hair loss • Patients feels well and the areas are not excessively itchy or painful • Usually fungus contracted from an animal • Treat with oral terbenafine for one month Tinea barbae Rosacea Definition of Rosacea • Formal definition difficult1,2 – represents a constellation of clinical symptoms and signs – Pathogenesis complex and illdefined • Chronic inflammatory dermatosis • associated with altered vascular tone leading to vasodilatation & increased blood flow 1.Powell FC. N Engl J Med. 2005; 352(8): 793-803. 2.Liu RH, et al. Arch Dermatol. 2006; 142(8): 1047-52. Rosacea subtypes 1 - 4 • • • • Erythematotelangiectactic ETTR Papulopustular PPR Phymatous PR Ocular OR Nat Ros Soc, JAAD 2002; 46: 584-7 Rosacea:subtype I Erythematotelangiectatic1 • • • • First described at the start of the 19th century Flushing & persistent central facial erythema, +/- telangiectasia (dilated superficial blood vessels) 2 Painful symptomatology2 Sparing of the periocular area and nasolabial region May have associated ocular rosacea Rhinophyma occasionally coexists 1. Wilkin J, et al. J AAD 2002; 46(4): 584-7. 2. Crawford GH, JAAD. 2004; 51(3): 327-41 Rosacea:subtype 2 Papulopustular1,2 • • Central facial erythema with transient pustules and/or dome- shaped papules Frequently accompanied by burning & stinging Can be seen in other sites – Bald heads, pinnae, and chest, response to treatment very slow 1. Wilkin J, et al. J AAD 2002; 46(4): 584-7. 2. Crawford GH, JAAD. 2004; 51(3): 327-41 Rosacea: subtype 3 Phymatous1 Thickened skin with prominent pores, typically on the nose chin (gnathophyma), forehead (metophyma), ears (otophyma) and eyelids (belpharophyma)2 May be no other features of rosacea More common in males 10:1 Sebaceous gland & connective tissue hyperplasia surface irregularities,nodules once fibrosis developed treatment response less good 1. Wilkin J, et al. J AAD 2002; 46(4): 584-7. 2. Crawford GH, JAAD. 2004; 51(3): 327-41 Rhinophyma Commoner in men Resurfacing Laser Surgical Rosacea: subtype 4 Ocular (usually bilateral)1 50% strongly linked to flushing, may precede skin problems Dry eyes (Shirmers dry eye test), irritation, crusting, redness, itching, burning, recurrent styes or infections Watery or bloodshot conjunctivae – Foreign body sensation, irritation, light sensitivity & blurred vision Blepharo-conjuncitivitis2,3 – Telangiectasia /conjunctival injection, swelling and scaling of lid margin Take advice from ophthalmologist for treatment 1. Wilkin J, et al. JAAD 2002; 46(4): 584-7. 2. Akpek EK, et al. Ophthalmology 1997;104:1863-7. 3.Ghanem VC et at. Cornea 2003;22:230-3. Rosacea: subtype 4 Keratitis 5% Severe pain, photophobia and blurred vision may lead to corneal inflitrates, thinning, scarring, vascularisation and perforation more common in males Episcleritis, scleritis, iritis rare1 Sicca syndrome Manifestation of malfunction of the meibomian gland - tear secretion abnormal2 . 1. Akpek EK, Ophthalmology 1997;104:1863-7 Bron AJ, Ocul Surf. 2004 Apr;2(2):149-65 Treatment • Define the various subtypes and treat them accordingly • Sunblock is important • Avoid triggers that flare the rosacea (eg alcohol, spicy food, sunlight, specific cosmetics) • Treat co-existing seborrhoeic dermatitis Treating inflammatory rosacea • • • • • • • • Topical 0.75% & 1% metronidazole Topical 15% alezaic acid Topical 1% ivermectin (Soolantra®) Oral tetracyclines Low dose Doxycycline MR Oral erythromycin or clarithromycin Oral metronidazole (max 3 mths) Oral isotretinoin Topical agents • Metronidazole & alezaic acid may cause irritation • Use for 12-16 wks for maximum response • If clear at this point, stop treatment and restart if rosacea returns • Some patients require continuous use Topical Ivermectin (Soolantra®) • Anti-inflammatory • Use daily for 16 wks • More effective than topical metronidazole or alezaic acid • Longer remission after 16 week daily course than topical metronidazole • Low irritancy Oral antibiotics • No clinical efficacy advantage of different options • Low dose 40mg slow-release doxycycline cause the least GI irritation and is the only oral agent actually licensed for rosacea • Treat for at least 12 weeks and stop to see if condition is in remission. Re-start as required • For non-responsive/aggressive disease, add in a topical agent and continue that topical agent long-term, after the oral antibiotic has been stopped • Oral metranidazole can cause peripheral nerve damage with prolonged use, so should be limited to 3 mth maximum • Oral minocycline has a side-effect profile that should limit its use Isotretinoin • Requires referral to community or hospital dermatology for consultant dermatologist prescribing • Long –term remission unlikely. Usual objective is to modify severe rosacea into mild or moderate rosacea that this more treatment responsive • Length of isotretinoin course and dose is variable Treatment of facial erythema • If confluent and re-active (still flushing and blushing) then consider 0.03% brimomidine gel daily • Intense Pulsed Light (IPL) also works well for those (but not normal available to NHS patients) • If static with visible blood vessels then vascular laser or IPL indicated (also not readily available to NHS patients) Topical 0.03% Brimonidine • • • • • • Effective for rosacea erythema Last for about 12 hours Not effective for fixed redness and visible thread veins Inflammation (papules and pustules) must be treated first Any dry skin or facial eczema must be treated first Regular application applied thinly is better tolerated than intermittent application – at least for the first two months • About 20% of patients experience rebound erythema Treatment for rhinophyma • Surgical debridement or CO2 laser ablation • The inflammatory condition must be controlled first and long-term oral antibiotics prescribed after, to prevent re-growth • Often only done on NHS patients if there is proof of sleep apnoea Rosacea:Conclusions • Enigmatic disease of uncertain pathophysiology • Diverse spectrum of signs and symptoms • Inflammation plays an important role • Causes significant psychosocial morbidity • Consideration of clinical subtypes should be considered in any management approach • Refer patients with aggressive and nonresponsive disease Dermatomyositis- connective tissue disorder Dermatomyositis Discoid lupus (DLE) • Cheeks, nose & ears (also upper back, scalp, neck & hands) • Red scaly patches, white scarring, post-inflammatory hyperpigmentation and scarring alopecia • Flares caused by sunlight exposure • An aggressive inflammatory condition of unknown cause DLE dermoscopy images DLE Differential diagnosis • • • • • • Tinea Mycosis fungoides Psoriasis Sarcoidosis (lupus pernio) Jessner’s infiltrate Cutaneous TB (lupus vulgaris) • Lichen planus Investigations • Biopsy is essential, given the differential diagnosis • Biopsy for normal H&E staining, but ideally also for IMF. Therefore, consider referring to the community or hospital dermatology team for this • ANA and C3 & C4 to exclude SLE Treatment • • • • Total sunblock is essential Topical steroids (eg mometasone) 0.1% tacrolimus ointment Tapering course of oral steroids Second line hospital treatments • Hydroxychloroquine • Methotrexate • Dapsone • Oral gold • Acitretin • Azathioprine In conclusion • There are many potential facial rashes that require careful consideration from the patient’s history and clinical features • In some cases a skin biopsy is necessary • Many effective treatments are off-label or need to be used cautiously on the facial skin • GPs should be aware of the profound psychological and social impact of facial rashes. Treatment and review of that treatment as well as onward referral should be prompt and efficient Resources For the doctor • www.bad.org.uk For the patient • www.rosacea.org • www.pcds.org.uk • www.lupus.org.uk Thank you Contact details: 020 7635 1019 [email protected] www.dmchealthcare.co.uk