Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
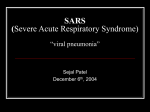
Clinical Science (2006) 110, 193–204 (Printed in Great Britain) doi:10.1042/CS20050188 R E V I E W SARS: clinical presentation, transmission, pathogenesis and treatment options Paul K. S. CHAN∗ †, Julian W. TANG∗ and David S. C. HUI†‡ ∗ Department of Microbiology, Faculty of Medicine, The Chinese University of Hong Kong, Hong Kong Special Administrative Region, People’s Republic of China, †Centre for Emerging Infectious Diseases, School of Public Health, Faculty of Medicine, The Chinese University of Hong Kong, Hong Kong Special Administrative Region, People’s Republic of China, and ‡Department of Medicine and Therapeutics, Faculty of Medicine, The Chinese University of Hong Kong, Hong Kong Special Administrative Region, People’s Republic of China A B S T R A C T SARS (severe acute respiratory syndrome) appeared as the first emerging infectious disease of this century. It is fortunate that the culprit virus can be grown without much difficulty from a commonly used cell line, allowing an unlimited supply of isolates for further molecular studies and leading to the development of sensitive diagnostic assays. How the virus has successfully jumped the species barrier is still a mystery. The superspreading events that occurred within hospital, hotel and high-density housing estate opens a new chapter in the mechanisms and routes of virus transmission. The old practice of quarantine proved to be still useful in controlling the global outbreak. Despite all the available sophisticated tests, alertness with early recognition by healthcare workers and prompt isolation of suspected cases is still the most important step for containing the spread of the infection. Although the rapidly evolving outbreak did not allow the conducting of systematic clinical trails to evaluate treatment options, the accumulated experience on managing SARS patients will improve the clinical outcome should SARS return. Although SARS led to more than 700 deaths worldwide, the lessons learnt have prepared healthcare systems worldwide to face future emerging and re-emerging infections. INTRODUCTION An outbreak of atypical pneumonia of unknown aetiology occurred in November 2002 in Foshan, Guangdong Province in southern China [1,2]. The disease spread to Guangzhou in early 2003. In March 2003, similar outbreaks were noted in Vietnam, Hong Kong and Canada and subsequently involved more than 30 countries [3–6]. In view of the multiregion involvement and the severity of the disease, the WHO (World Health Organization) declared in early March 2003 that a global outbreak was occurring and set up a network of laboratories to investigate the cause as well as means to control the spread of the disease. The disease was officially named ‘severe acute respiratory syndrome’ (SARS). In late March 2003, a few laboratories independently identified Key words: coronavirus, inflammation, respiratory infection, severe acute respiratory syndrome (SARS), viral transmission. Abbreviations: ACE-II, angiotensin-converting enzyme 2; ALT, alanine aminotransferase; ARDS, acute respiratory distress syndrome; FIPV, feline infectious peritonitis virus; huMab, human monoclonal antibody; IFN, interferon; IL, interleukin; IP10, IFN-γ -inducible protein-10; IVIg, intravenous γ -globulin; LDH, lactate dehydrogenase; LPV/r, 400 mg of lopinavir/100 mg of ritonavir; MCP-1, monocyte chemoattractant protein-1; MHV, mouse hepatitis virus; NO, nitric oxide; NPPV, non-invasive positive pressure ventilation; R0 , reproductive number; S protein, spike glycoprotein; SARS, severe acute respiratory syndrome; SARS-CoV, SARS-associated coronavirus; TGEV, transmissible gastroenteritis virus; TNF-α, tumour necrosis factor-α; WHO, World Health Organization. Correspondence: Professor Paul K. S. Chan, Department of Microbiology, The Chinese University of Hong Kong, 1/F Clinical Science Building, Prince of Wales Hospital, Shatin, New Territories, Hong Kong Special Administration Region, People’s Republic of China (email [email protected]). C 2006 The Biochemical Society 193 194 P. K. S. Chan, J. W. Tang and D. S. C. Hui a previously unrecognized coronavirus as the aetiological agent of SARS. The virus was named SARS-CoV (SARS-associated coronavirus). The global outbreak ended in July 2003 with a total of 8098 probable cases and at least 774 deaths recorded (see http://www.who. int/csr/sars/country/table2003 09 23/en for a summary of probable SARS cases with onset of illness from 1 November to 31 July 2003). THE VIRUS The family Coronaviridae contains two separate genera: coronaviruses and toroviruses. Coronaviruses are found in a wide range of animal species. In humans, coronaviruses are mainly respiratory pathogens, although they have been occasionally shown to be the cause of some cases of diarrhoea. Before the SARS epidemic, only two human coronaviruses had been characterized (HuCoV229E and HuCoV-OC43). Both of these usually cause a mild upper respiratory tract infection. Coronaviruses are large lipid-enveloped, positivesense, single-stranded RNA viruses, approx. 30 kb in length and are the largest RNA viruses known. The virus codes for several proteins, including an RNA-dependent RNA polymerase (Pol), a surface spike glycoprotein (S protein), which attaches the virus to a host cell and is the target for neutralizing antibodies [8,9], a small envelope protein (E), a membrane glycoprotein (M) and a nucleocapsid protein (N) complexed with the viral RNA. The haemagglutinin esterase (HE) protein is also coded for in HuCoV-OC43 and some animal coronaviruses, but not in SARS-CoV [10]. There are other ORFs (open reading frames), whose functions are being gradually revealed. Coronaviruses have a unique replication system in that all mRNAs form a nested set with a common polyadenylated 3 -end, with only the unique 5 -end fragment being translated into amino acids [11]. Mutations are common, as for all RNA viruses, and if two coronaviruses infect the same host cell simultaneously genetic recombination is possible [12]. However, no evidence of recombination was found from the SARS-CoV genomes detected during the course of global outbreak in 2003 [13,14]. Animal and human coronaviruses have been classified into three different serologically distinct groups based on their antigenicity [13,14]: Group 1 contains HuCoV229E and porcine [TGEV (transmissible gastroenteritis virus) and PDEV, (porcine diarrhoea epidemic virus)], feline [FIPV (feline infectious peritonitis virus)] and canine coronaviruses; Group 2 contains HuCoV-OC43 along with MHV (mouse hepatitis virus), bovine coronavirus and haemagglutinating encephalomyelitis virus; and Group 3 contains avian coronaviruses, including IBV (infectious bronchitis virus) of chickens and turkey coronavirus. SARS-CoV seems to lie in a group of its own, C 2006 The Biochemical Society based on sequencing studies of its various viral proteins [13,14]. The receptor for the human coronavirus HuCoV229E has been reported to be human aminopeptidase N (CD13) [15]. In Group 2, HuCoV-OC43 may use one of several cell-surface molecules, including 9-O-acetylated neuraminic acid and the HLA-1 molecules [16,17]. It has been shown that SARS-CoV uses ACE-II (angiotensinconverting enzyme 2) as the cellular receptor [18,19]. A good correlation between the expression of ACE-II and tissue tropism has been shown [20]; however, the presence of ACE-II is unlikely to be the sole determinant for tropism [21]. The C-type lectin CD209L (L-SIGN) human cellular glycoprotein may also possibly be a receptor for SARS-CoV [22]. CLINICAL FEATURES SARS-CoV produces an acute viral infection in humans with an incubation period ranging from 2–10 days [3–5]. During the 2003 outbreak, most patients were admitted to hospital between 3–5 days following the onset of illness [23]. The presenting features in adults are pronounced. These include persistent high fever, chills and rigor, malaise, myalgia, headache and dry cough. Most patients had some degree of dyspnoea at presentation, which increased towards the end of the first week of illness. Sputum production, sore throat and rhinorrhoea were less commonly reported symptoms [3–5,24,25]. The reported proportion of patients with gastrointestinal symptoms varies among different clusters. For the first hospital outbreak in Hong Kong, 20 % of patient had diarrhoea at presentation, and another 18 % developed diarrhoea during the course of illness [26]. It is worth noting that in eight of the 138 (5.8 %) patients in the cohort, fever and diarrhoea were their only presenting symptoms. The diarrhoea was mainly watery without blood or mucus, lasting for 3.7 + − 2.7 days. A few patients had mild abdominal pain. In the Toronto outbreak, 24 % of the 144 patients had diarrhoea at presentation [5]. A remarkably high proportion (70 %) of patients in the rapidly evolving community outbreak, which occurred at the Amoy Gardens Residential Estate in Hong Kong, had diarrhoea at presentation. Reactive hepatitis is a common complication of SARSCoV infection with 24 % of patients having elevated ALT (alanine aminotransferase) levels on admission, and 69 % had raised ALT levels during the subsequent course of their illness. Those with severe hepatitis had worse clinical outcome [27]. Lymphopenia, low-grade disseminated intravascular coagulation (DIC-thrombocytopenia, prolonged activated partial thromboplastin time and elevated D-dimers), elevated LDH (lactate dehydrogenase) and CK (creatinine kinase) are common abnormalities detected in SARS patients [3–6,28,29]. SARS: clinical presentation, transmission, pathogenesis and treatment options In general, the radiographical features of SARS are similar to those found in community-acquired pneumonia caused by other organisms [30]. Nevertheless, several characteristic features are frequently observed in SARS, including the predominant involvement of the lung periphery and the lower zones, whereas cavitation, hilar lymphadenopathy and pleural effusion are rarely found [3,30]. Radiographical changes progress from a unilateral focal air-space opacity, to multifocal or bilateral involvement during the later phase of disease. These lesions resolve, naturally or as a response to treatment, in a large proportion of patients (Figure 1) [3,30]. In a case series, 12 % of patients developed spontaneous pneumomediastinum and 20 % of patients developed evidence of ARDS (acute respiratory distress syndrome) over a period of 3 weeks [31]. The reported incidence of barotrauma among patients receiving intensive care was high (26 %), despite using low-volume and low-pressure mechanical ventilation [32]. High-resolution computer tomography of the thorax is useful in detecting lung opacities in cases with a high index of clinical suspicion of SARS, but with unrevealing unremarkable chest radiographs. Remarkable features observed from high-resolution computer tomography include ground-glass opacification, sometimes with consolidation, and interlobular septal and intralobular interstitial thickening, with predominantly peripheral and lower lobe involvement (Figure 2) [33]. SARS-CoV was detected in the cerebrospinal fluid and serum samples of two cases with status epilepticus [34,35]. The data suggest that a severe acute neurological syndrome might occasionally accompany SARS. Older subjects with SARS often show atypical presenting features such as decrease in general well-being, poor feeding and delirium [36–38]. The fact that older SARS patients might be afebrile further hinders early recognition. Young children (< 12 years of age) often run a more benign clinical course mimicking other viral upper respiratory tract infections, whereas teenagers tend to have a clinical course similar to that of adult SARS patients [3,39]. No fatality has been reported in young children and teenage patients [39–42]. A number of studies have been conducted to search for asymptomatic cases of SARS-CoV infection [43,44]. It is now quite certain that asymptomatic infection is very rare in adults; however, data on children and elderly are less comprehensive. TRANSMISSION The origin of SARS-CoV is, at present, thought to be the Himalayan palm civet (Paguma larvata) found in Guangdong province in south China, from which coronaviruses very similar to SARS-CoV isolated from humans have been detected [45–47]. The fact that a much Figure 1 Serial chest radiographs of a 31-year-old healthcare worker infected with SARS in 2003 There was an opacity involving the right upper lobe initially (a), with progression to ARDS during the second week of his illness requiring invasive mechanical ventilation (b). Following intensive care support and treatment with intravenous pulse of steroids, he made an uneventful recovery (c). higher seroprevalence of SARS-CoV was found among wild animal handlers in Guangdong also supports its animal origin. Although it is still a mystery how SARSCoV has crossed the species barrier, a number of reports have provided detailed descriptions on the transmission of SARS-CoV among humans. The transmission of most respiratory viruses is a combination of direct contact (touch), short-range (large C 2006 The Biochemical Society 195 196 P. K. S. Chan, J. W. Tang and D. S. C. Hui Figure 2 High-resolution computer tomography of the thorax taken on day 7 of a patient with SARS Several areas of ground-glass opacities involving predominantly the lower lobes of both lungs were observed. droplet; within 1 m) and long-range (droplet nuclei; beyond 1 m and further) [48,49]. There are several infectious agents that are recognized to be spread by all three routes with equal importance, e.g. tuberculosis, measles and chicken pox [49], but most are transmitted mainly by direct contact and short-range routes, with occasional instances where long-range transmission can be the only explanation, e.g. influenza [50]. The source for such transmission events is normally the infected patient’s upper respiratory tract, and not via the haematogenous or faecal–oral routes. The transmission of SARS-CoV is similar to other respiratory viruses, but with several important differences. A brief summary of the early stage of the SARS epidemic in Hong Kong will highlight this. The first international dissemination of SARS-CoV was related to a ‘superspreader’, a 64-year-old physician from southern China. He visited Hong Kong on 21 February 2003 and stayed in Hotel M. He died 10 days later of severe pneumonia. He spread the infection to at least 16 hotel guests or visitors who had visited the floor where he stayed. The infection was spread subsequently to other parts of Hong Kong, Vietnam, Singapore [4] and Canada [5] within a short period of time [3–6]. The high infectivity of this viral illness is supported by the fact that 138 patients (many of whom were healthcare workers) were infected with SARS-CoV within 2 weeks after the admission of this single index case from Hotel M [3,51]. This superspreading event is thought to be related to the administration of a nebulized bronchodilator to the index case, together with overcrowding and poor ventilation in the hospital ward. Many cases of nosocomial SARS-CoV transmission between healthcare workers and patients occurred in intensive care units, where there is particularly close contact between healthcare workers and patients [52–56]. C 2006 The Biochemical Society Next, there was evidence to suggest that SARS might have spread by long-range airborne transmission in a major community outbreak in a private residential complex in Hong Kong [57]. There are several other hypotheses for this major outbreak, including passive carriage of viruses by pests, drying up of U-shaped bathroom floor drain which allowed the backflow of contaminated sewage or its aerosolized particles and creation of infectious aerosol current by the use of residential exhaust fans in the toilet [58,59]. Other circumstantial evidence are also in line with the airborne transmission hypothesis for SARS-CoV. For instances, air samples obtained from a room occupied by a SARS patient, and swabs taken from frequently touched surfaces in rooms and at a nurse station, were positive for SARS-CoV by PCR [60]. The temporal–spatial spread of SARS among patients in a medical ward where there was a SARS outbreak, at the Prince of Wales Hospital in Hong Kong, was also consistent with airborne transmission [61]. Hence, from this account, one of the main difficulties in controlling SARS transmission during the early stages of the worldwide epidemic is the readiness with which the virus could spread between healthcare workers and their patients (mainly direct or short-range transmission), but also the existence of ‘superspreaders’ who generate a far greater than average number of secondary cases. The reasons for this are still not known for certain, but may be a combination of host and viral factors. The basic R0 (reproductive number) of an infectious agent generally gives an indication of transmissibility of the agent and can also estimate the vaccine coverage required in an otherwise susceptible population, to prevent person-to-person spread of the agent and an ensuing epidemic. Estimates for the R0 of SARS-CoV have been reported by several authors, but in each case, the superspreaders were left out of the estimates, so as not to skew the results for the majority of SARS-CoVinfected individuals. The R0 for SARS-CoV has been estimated to be between 2 and 3 [62,63]. These two analyses excluded superspreading events in their final value of R0 , because the transmission route for these events were almost certainly atypical of the disease in most cases and may have been assisted in some way [57,61]. This value of R0 puts SARS-CoV quite low down on the scale of transmissibility (Table 1) [64–66]. Thus, in the absence of superspreaders, the transmissibility of SARS-CoV would be lower than poliovirus. PATHOGENESIS After binding to their respective receptors, using the S protein, human coronaviruses (HuCoV-229E, HuCoVOC43 and SARS-CoV) enter their host cell. This is usually a ciliated respiratory tract epithelial cell in the nasopharynx [12,67]. Thereafter, the mechanisms by which SARS-CoV causes disease can be separated into SARS: clinical presentation, transmission, pathogenesis and treatment options Table 1 R0 for various infectious agents Adapted from Mims et al. [64], with additional references: ∗ [62,63]; †[65,66]. Infectious disease Basic R0 Measles Whooping cough Mumps Rubella Diphtheria Poliomyelitis Influenza∗ SARS† 15–17 15–17 10–12 7–8 5–6 5–6 1.68–20 2–3 two: (i) the direct lytic effects of the virus on host cells, and (ii) the host immune response to the infection. The immune response to viral invasion and replication is a combination of early innate and later adaptive responses. Animal and in vitro studies have demonstrated that coronavirus replication within the host cell leads to a variety of effects, such as cellular necrosis or lysis [68,69], apoptosis [68,70] or cell fusion to form syncytia [71]. Studies in mice have shown that there is a potent CD8 T-cell response with acute MHV infection [72], and that fulminant hepatitis can result from induced transcription of a novel fgl2 prothrombinase gene by the MHV nucleocapsid protein [73]. In cats with FIPV, the humoral response and production of antibodies to the S protein induces peritonitis [74]. Human infection with SARS-CoV, similarly, leads to an acute inflammatory response. In humans, SARS-CoV causes diffuse alveolar damage and deposition of fibrin with macrophage and giant cell infiltration in lung tissue [75,76]. Acute hepatitis has been widely reported and may be a result of immune-mediated, rather than direct, SARS-CoV viral damage [27,77,78]. Haematological disturbances have been suspected to be a result of both direct viral and immune-mediated mechanisms affecting haematopoiesis [16]. The S protein may be the main factor in determining the severity of clinical disease, because of its roles in viral entry, pathogenesis, antiviral response, virulence and cellular and species tropism [8,20,45,79]. Again, studies on animal coronavirus S proteins have helped to define this. Mutations in S proteins have been shown to significantly affect the viral virulence and tissue tropism of MHV [80,81] and TGEV [82]. Numerous authors have attempted to determine the role of various cytokines in the pathogenesis of SARSCoV infection, but the picture is still confusing. Most reports describe a change in levels of IL (interleukin)-1, IL-2, IL-4, IL-6, IL-8, IL-10, IL-12, IL-13, IL-16, IL17 and IL-18, TNF-α (tumour necrosis factor-α) and IFN (interferon)-γ and -α, but there is little consistency between the different reports. In one study from Hong Kong, 20 patients with proven SARS-CoV infection demonstrated raised levels of inflammatory cytokines IL-1, IL-6 and IL-12 and the neutrophil chemokine IL-8. The Th1 cytokine IFNγ was also raised; however, the inflammatory cytokine TNF-α was not and neither was the inflammatory cytokine IL-10, the Th1 cytokine IL-2 or the Th2 cytokine IL-4. The picture is one of Th1-cell-mediated immunity [83]. Other cytokines shown to be raised were MCP-1 (monocyte chemoattractant protein-1) and IP-10 (IFNγ -inducible protein-10). Other authors have supported some of these findings. Duan et al. [77] investigated the cytokine profile in Beijing SARS patients with elevated liver enzymes and also reported raised levels of IL-1 (IL1β), IL-6 and IL-8, but also raised levels of IL-2, IL-4 and IL-10, in contrast with Wong et al. [83]. In fact, raised levels of IL-6 and IL-8 have also been reported from SARS patients in Guangzhou [84] and Taiwan [85]. Xie et al. [86] and Zhang et al. [87] report raised levels of IL-8 and IL-6 respectively. Some of these studies [77,87] and others [88] have also reported raised levels of IL-10. However, contrasting results have also been reported between these authors. Zhang et al. [87] reported a fall in IL-8 levels, whereas Wang et al. [89] reported no change in levels. Similarly, Ng et al. [90] and Wang et al. [89] reported no change in IL-6 levels. With TNF-α, the picture is very mixed, with several reports stating an increase in levels [77,86,89], some reporting no significant elevation [83,87,90] and others reporting a fall in levels [85]. The picture for IFN-γ is equally inconsistent with Wong et al. [83] and Huang et al. [85] reporting a rise in levels, but Zhang et al. [87] reporting a fall. The main picture that seems to emerge from the majority of the studies is that IL-6 and IL-8 are raised during SARS-CoV infection. IL-6 is secreted by macrophages and T-lymphocytes and causes fever, induces acute-phase proteins and activates lymphocytes. IL-8 is secreted by monocytes, macrophages, fibroblasts and keratinocytes and is a chemoattractant and enhances access for neutrophils to the site of infection [91]. The reported variations in the levels of all these inflammatory markers may well be because of differences in sample collection times relative to the onset of SARS-CoV infection. Generally, however, the reports agree that SARS-CoV infection produces a strong host immune response and that the complications of SARS may well be a consequence of this. Further studies are necessary to define the role of specific cytokines better, especially if they can lead to an earlier diagnosis or prognosis, or even a specific therapy for SARS [92]. TREATMENT The clinical course of SARS can be divided into two phases: Phase I refers to active viral replication where patients experience high fever, myalgia and other systemic symptoms that generally improve after a few days; and C 2006 The Biochemical Society 197 198 P. K. S. Chan, J. W. Tang and D. S. C. Hui Phase II refers to the stage of immunopathological injury where patients experience a recurrence of fever, increasing hypoxaemia and radiological progression of pneumonia with falls in viral load. The timing of administration of treatment with respect to these two phases needs to be considered when evaluating its efficacy. Ribavirin Ribavirin, a nucleoside analogue that has activity against a number of viruses in vitro, was widely used for treating SARS patients after observing the lack of clinical response to broad-spectrum antibiotics and oseltamivir [3–6,31]. Nevertheless, it is now known that ribavirin has no significant in vitro activity against SARS-CoV [93–95]. Haemoglobin levels in approx. 60 % of patients fell by 2 g/dl after 2 weeks of oral ribavirin therapy, at a dose of 1.2 g three times/day [96]. The use of ribavirin for SARS in Toronto was based on the higher dosage used for treating haemorrhagic fever, which led to more toxicity, including elevated liver transaminases and bradycardia [5]. Furthermore, addition of ribavirin did not have any useful effect on the serum SARS-CoV viral load in paediatric SARS patients [97]. Therefore it is highly unlikely that ribavirin alone has any significant clinical benefits in the treatment of SARS. Protease inhibitors Genomic analysis of the SARS-CoV has revealed several enzymatic targets including proteases [13,14,98]. Lopinavir and ritonavir in combination is a boosted protease inhibitor regimen widely used in the treatment of HIV infection. In vitro activity against SARS-CoV has been demonstrated for lopinavir and ribavirin at 4 and 50 µg/ml respectively. Inhibition of in vitro cytopathic effects was achieved down to a concentration of 1 µg/ml lopinavir combined with 6.25 µg/ml ribavirin. The data, therefore, suggest that this combination might be synergistic against SARS-CoV in vivo [99]. The addition of LPV/r (400 mg of lopinavir/100 mg of ritonavir) as initial therapy was associated with significant reduction in overall death rate (2.3 % compared with 15.6 %) and intubation rate (0 % compared with 11 %) when compared with a matched historical cohort that received ribavirin alone as the initial antiviral therapy [100]. Other reported beneficial effects include a reduction in corticosteroid use, fewer nosocomial infections, a decreasing viral load and rising peripheral lymphocyte count [99]. In contrast, the subgroup that had received LPV/r as rescue therapy after receiving pulsed methylprednisolone treatment for worsening respiratory symptoms was not better than the matched cohort [100]. The improved clinical outcome in patients that received LPV/r as part of the initial therapy may be due to the fact that both peak (9.6 µg/ml) and trough (5.5 µg/ml) serum concentrations of lopinavir could inhibit the virus [101]. Nelfinavir, another protease inhibitor commonly used for HIV C 2006 The Biochemical Society infection, has been shown to inhibit replication of SARSCoV in Vero cell culture [102]. Further evaluation of this form of therapy is warranted. IFNs Type I IFNs such as IFN-α are produced early as part of the innate immune response to virus infections. Type I IFNs inhibit a wide range of RNA and DNA viruses including SARS CoV in vitro [94,95,103]. Complete inhibition of cytopathic effects of SARS-CoV in culture was observed for IFN subtypes β-1b, α-n1 and α-n3, and human leucocyte IFN-α [94]. IFN-α had an inhibitory effect in vitro on SARS-CoV starting at concentrations of 1000 IU/ml (where IU is international units) [95], whereas recombinant human IFN-β1a potently inhibited SARS-CoVin vitro [104]. IFN-β and IFN-γ can synergistically inhibit the replication of SARS-CoV in vitro [105]. In addition, a combination of ribavirin and IFN-β has been shown to have synergistic effects in inhibiting SARS-CoV in animal and human cell lines [106], and combinations of ribavirin with either IFN-β 1a or IFN-α also show synergistic effects in vitro [107]. In experimentally infected cynomolgus macaques, prophylactic treatment with pegylated IFN-α significantly reduced viral replication and excretion, viral antigen expression by type 1 pneumocytes and pulmonary damage compared with untreated macaques, whereas post-exposure treatment with pegylated IFN-α yielded intermediate results [108]. Use of IFN-α 1 plus corticosteroids was associated with improved oxygen saturation, more rapid resolution of radiographical lung opacities and lower levels of CPK (creatine kinase) in SARS patients [109]. These findings support clinical testing of approved IFNs for the treatment of SARS. huMab (human monoclonal antibody) There is evidence that SARS-CoV infection is initiated through binding of the SARS-CoV S protein to ACE-II [18]. A high-affinity huMab has been identified against the SARS-CoV S protein, termed 80R, that has potent neutralizing activity in vitro and in vivo [110]. huMab 80R efficiently neutralizes SARS-CoV and inhibits syncytia formation between cells expressing the S protein and those expressing the SARS-CoV receptor ACEII. huMab 80R may be a useful viral entry inhibitor for the emergency prophylaxis and treatment of SARS [110]. huMab has been shown to prophylactically reduce replication of SARS-CoV in the lungs of infected ferrets and abolish shedding of viruses in pharyngeal secretions in addition to completely preventing SARS-CoV-induced macroscopic lung pathology [111]. Vaccines Currently, different vaccines, such as whole-killed vaccine, adenovirus vector vaccine and recombinant S SARS: clinical presentation, transmission, pathogenesis and treatment options protein vaccine, are being tested. An adenoviral-based vaccine has been shown to induce strong SARS-CoVspecific immune responses in rhesus macaques and hold promise for the development of a protective vaccine against SARS-CoV [112]. A DNA vaccine based on the S gene has been shown to induce the production of a specific IgG antibody against SARS-CoV efficiently in mice with a seroconversion rate of 75 % after three doses of immunization [113,114]. Recombinant S proteins that exhibit antigenicity and receptor-binding ability are also good candidates for developing a SARS vaccine [115]. It have been shown that a recombinant attenuated vaccinia virus, Ankara, expressing the S protein of SARS-CoV can elicit protective immunity in mice [116]. Another recombinant attenuated parainfluenza virus expressing the S protein also produced immunity following intranasal inoculation to mice [117]. A synthetic peptide derived from the S protein is another target for vaccine development. Promising results have been obtained in vitro [118] and in vivo from rabbit and monkey models [119]. Systemic corticosteroids During the Phase II of clinical course when patients progressed to develop pneumonia and hypoxaemia, intravenous administration of rescue-pulsed methylprednisolone has been shown to suppress cytokine-induced lung injury [3,31,96,99,120]. The rationale could be that the progression of the pulmonary disease is mediated by the host inflammatory response [31]. Corticosteroids significantly reduced IL-8, MCP-1 and IP-10 concentrations from 5–8 days after treatment in 20 adult SARS patients [81]. Induction of IP-10 is thought to be a critical event in the initiation of immune-mediated lung injury and lymphocyte apoptosis [82]. The use of rescue-pulsed methylprednisolone during clinical progression was associated with favourable clinical improvement, with resolution of fever and lung opacities within 2 weeks [3,96,120]. However, a retrospective analysis showed that the use of pulsed methylprednisolone was associated with increased risk of 30 day mortality (adjusted odds ratio, 26.0; 95 % confidence interval, 4.4–154.8) [121]. This retrospective study could not establish whether a causal relationship existed between the use of methylprednisolone and an increased risk of death, as clinicians were more inclined to give pulsed methylprednisolone therapy in deteriorating patients. Nevertheless, complications, such as disseminated fungal disease [122] and avascular necrosis of bone, have been reported following prolonged corticosteroid therapy [123]. With the rescue pulsed steroid approach, avascular necrosis of bone was found in 12 (4.7 %) patients after screening 254 using MTI (magnetic resonance imaging). The risk of avascular necrosis was 0.6 % for patients receiving < 3 g, and was 13 % for those receiving > 3 g of prednisolone-equivalent dose [124]. A randomized placebo-controlled study conducted at Prince of Wales Hospital, Hong Kong showed that plasma SARS-CoV RNA concentrations in the second and third weeks of illness were higher in patients given initial hydrocortisone (n = 10) than those given normal saline (n = 7) during Phase I of the clinical course of illness [125]. Despite the small sample size, the data suggest that pulsed steroid given in the earlier phase may prolong viraemia and thus it should only be given during later phase for rescue purpose. Carefully designed clinical trials, if ever possible, of a larger sample size are required to determine the optimal timing and dosage of systemic steroid in the treatment of the possibly immune-mediated lung injury in SARS. Convalescent plasma Convalescent plasma, donated by patients who had recovered from SARS, contains neutralizing antibodies and may be useful clinically for treating other SARS patients [126,127]. Research work in the preparation of SARS-CoV-specific hyperIg from convalescent plasma donated by patients who have recovered from SARS is currently in progress. Traditional Chinese medicine Glycyrrhizin, an active component of liquorice roots, has been shown to inhibit the replication of SARS-CoV in vitro [93]. A controlled study comparing integrative Chinese and Western medicine compared with Western medicine alone has suggested that the combination treatment given in the Phase I of SARS was more effective in reducing the number of patients with abnormal oxygen saturation [128]. However, it was not clear which of the Chinese medicine components was responsible for the benefit, and the dosage of steroid given to both groups was not clear. IVIg (intravenous γ -globulin) and pentaglobulin IVIg has immunomodulatory properties and may downregulate cytokine expression [129], and was used quite extensively in Singapore during the SARS outbreak in 2003. However, it was noted that one-third of critically ill patients developed venous thromboembolism, including pulmonary embolism, despite prophylactic use of lowmolecular-mass heparin [54]. There was evidence of pulmonary embolism in four out of eight postmortem cases [130]. In addition, there were five cases of large artery ischaemic stroke of which three cases had been given IVIg [131]. Pentaglobulin is IgM-enriched Ig. It was administered to 12 patients with SARS who continued to deteriorate despite pulsed steroid and ribavirin, and its use was associated with subsequent improvement in oxygenation and radiographical scores. It was difficult to judge its effects, as the study was uncontrolled and pulsed steroid C 2006 The Biochemical Society 199 200 P. K. S. Chan, J. W. Tang and D. S. C. Hui was also used concurrently [132]. Pulmonary artery thrombosis has been reported in a patient with SARS who was treated with ribavirin, steroid, lopinavir/ritonavir, IVIg and pentaglobulin [133]. It is possible that the IVIgor pentaglobulin-induced increase in viscosity may be consequential in patients with hypercoagulable states such as SARS [134]. include advanced age [3,23,31,141], chronic hepatitis B treated with lamivudine [31], severe hepatitis [27], high initial LDH [141], high peak LDH [3], high neutrophil count on presentation [3,141], diabetes mellitus or other co-morbid conditions [5,142], low CD4 and CD8 lymphocyte counts at presentation [143] and a high initial SARS-CoV viral load [97,144]. NO (nitric oxide) Long-term outcome Inhaled NO has been reported to have beneficial effects in SARS. In a controlled study comparing the use of NO (n = 6) and supportive treatment (n = 8) for severe respiratory failure, there was improvement in oxygenation after inhaled NO was administered and this allowed ventilatory support to be discontinued. Interestingly, the beneficial effects persisted after termination of NO inhalation [135]. NO has been shown to inhibit the replication cycle of SARS-CoV in vitro [136]. NPPV (non-invasive positive pressure ventilation) Approx. 20 % of SARS patients developed ARDS requiring invasive mechanical ventilation and this incurred a huge demand on intensive care units. Performing endotracheal intubation is a known risk for acquiring SARSCoV from the patient [137]. NPPV via face mask was applied to 20 patients in a hospital ward in Hong Kong which was installed with double exhaust fans and full personal protective equipment. Intubation was avoided in 14 patients and none of the 105 healthcare workers developed SARS clinically. SARS-CoV serology was negative in 102 (97 %), whereas the other three refused blood tests [138]. Although one cannot completely eliminate the possibility of subclinical SARS, it appears that NPPV is safe when applied in a ward environment with adequate air exchange provided the healthcare workers are wellequipped with full personal protective equipment and observe strict contact and droplet precautions [139]. Careful evaluation of the effectiveness of these possible modalities is needed before they can be recommended for treatment. Significant impairment of diffusing capacity occurred in 15.5 and 23.7 % of SARS survivors at the Prince of Wales Hospital cohort at 6 and 12 months respectively [145,146]. Although significant improvement in serial chest radiography was observed among the SARS survivors, 27.8 % of them still had abnormal radiographical scores at 12 months [146]. Despite the presence of extensive parenchymal changes revealed by computer tomography during the early convalescent period, surprisingly most SARS survivors had lung function test indices within normal limits. However, their exercise ability (6 min walk distance) at 12 months after illness onset was remarkably lower than the general population [146]. The functional disability appears out of proportion to the degree of lung function impairment and may be due to extrapulmonary factors such as muscle deconditioning and steroid myopathy [145,146]. Critical-illness-associated polyneuropathy/myopathy has also been observed in a few SARS survivors [147]. The reported incidence rates of avascular necrosis of bone among different cohorts in Hong Kong range from 4.7–15 % [124,148,149], whereas one study from Beijing reported a high incidence of 42 % [123]. In addition, there was significant impairment of healthrelated quality of life in our patients at 6 and 12 months [145,146]. The results are not surprising as, in addition to the physical impairment, the long period of isolation and extreme uncertainty during the SARS illness had created enormous psychological stress [150] and mood disturbances [151]. Furthermore, steroid toxicity, personal vulnerability and psychosocial stressors might have contributed to the development of psychosis in some patients [152]. Longer term follow-up is needed to assess if these deficits are persistent. OUTCOMES Short-term outcome Based on the data received by the WHO (http://www. who.int/csr/sars/archive/2003 05 07a/en/print.html), the case fatality rate for SARS was < 1 % for patients aged 24 years or younger, 6 % for 25–44 years, 15 % for 45–64 years, and > 50 % for patients aged 65 years or older. There is no evidence to suggest that a difference in mortality rate exists between different ethnic groups. A number of clinical/laboratory parameters have been shown have a prognostic value. Poor prognostic factors C 2006 The Biochemical Society SUMMARY AND CONCLUSIONS SARS is a highly infectious disease with a significant morbidity and mortality. Respiratory failure is the major complication and 20 % of patients may progress to ARDS. Healthcare workers are particularly vulnerable to SARS as the viral load of SARS-CoV in patients increase to peak levels during the second week when patients are hospitalized [21,31]. Since there is currently no proven effective treatment for SARS, early recognition, isolation and stringent infection-control measures SARS: clinical presentation, transmission, pathogenesis and treatment options are the key to controlling this highly contagious disease. Isolation facilities, strict droplet and contact precautions (hand hygiene, gown, gloves, N95 masks and eye protection) for healthcare workers managing SARS patients, avoid using nebulizers on general wards [3,51], contact tracing and quarantine isolation for close contacts are all important measures in controlling the spread of the infection in hospital and community. ACKNOWLEDGMENTS We are grateful to all healthcare workers and research staff of the Chinese University of Hong Kong for their dedication to the work on SARS. REFERENCES 1 Zhao, Z., Zhang, F., Xu, M. et al. (2003) Description and clinical treatment of an early outbreak of severe acute respiratory syndrome (SARS) in Guangzhou, PR China. J. Med. Microbiol. 52, 715–720 2 Xu, R. H., He, J. F., Evans, M. R. et al. (2004) Epidemiologic clues to SARS origin in China. Emerg. Infect. Dis. 10, 1030–1037 3 Lee, N., Hui, D. S., Wu, A. et al. (2003) A major outbreak of severe acute respiratory syndrome in Hong Kong. N. Engl. J. Med. 348, 1986–1994 4 Hsu, L. Y., Lee, C. C., Green, J. A. et al. (2003) Severe acute respiratory syndrome in Singapore: Clinical features of index patient and initial contacts. Emerg. Infect. Dis. 9, 713–717 5 Booth, C. M., Matukas, L. M., Tomlinson, G. A. et al. (2003) Clinical features and short-term outcomes of 144 patients with SARS in the greater Toronto area. JAMA, J. Am. Med. Assoc. 289, 2801–2809 6 Tsang, K. W., Ho, P. L., Ooi, G. C. et al. (2003) A cluster of cases of severe acute respiratory syndrome in Hong Kong. N. Engl. J. Med. 348, 1977–1985 7 Reference deleted 8 Keng, C. T., Zhang, A., Shen, S. et al. (2005) Amino acids 1055 to 1192 in the S2 region of severe acute respiratory syndrome coronavirus S protein induce neutralizing antibodies: implications for the development of vaccines and antiviral agents. J. Virol. 79, 3289–3296 9 Zhong, X., Yang, H., Guo, Z. F. et al. (2005) B-cell responses in patients who have recovered from severe acute respiratory syndrome target a dominant site in the S2 domain of the surface spike glycoprotein. J. Virol. 79, 3401–3408 10 Xu, J., Hu, J., Wang, J. et al. (2003) Genome organization of the SARS-CoV. Genomics, Proteomics Bioinformatics 1, 226–235 11 Lai, M. M. and Holmes, K. V. (2001) Coronaviridae: the viruses and their replication, In Fields Virology, 4th edn (Knipe, D. M., Howley, P. M., Griffin, D. E. et al., eds.) pp. 1163–1186, Lippincott Williams & Wilkins, Philadelphia 12 McIntosh, K. and Andersen, L. J. (2005) Coronaviruses, including severe acute respiratory syndrome (SARS)associated coronavirus. In Principles and Practice of Infectious Diseases, 6th edn (Mandell, G. L., Bennett, J. E. and Dolin, R., eds.), pp. 1990–1997, Churchill Livingstone, Philadelphia 13 Marra, M. A., Jones, S. J., Astell, C. R., et al. (2003) The genome sequence of the SARS-associated coronavirus. Science 300, 1399–1404 14 Rota, P. A., Oberste, M. S., Monroe, S. S. et al. (2003) Characterization of a novel coronavirus associated with severe acute respiratory syndrome. Science 300, 1394–1399 15 Yeager, C. L., Ashmun, R. A., Williams, R. K., Cardellichio, C. B., Shapiro, L. H., Look, A. T. and Holmes, K. V. (1992) Human aminopeptidase N is a receptor for human coronavirus 229E. Nature (London) 357, 420–422 16 Vlasak, R., Luytjes, W., Spaan, W. and Palese, P. (1988) Human and bovine coronaviruses recognize sialic acid-containing receptors similar to those of influenza C viruses. Proc. Natl. Acad. Sci. U.S.A. 85, 4526–4529 17 Collins, A. R. (1994) Human coronavirus OC43 interacts with major histocompatibility complex class I molecules at the cell surface to establish infection. Immunol. Invest. 23, 313–321 18 Li, W., Moore, M. J., Vasilieva, N. et al. (2003) Angiotensin-converting enzyme 2 is a functional receptor for the SARS coronavirus. Nature (London) 426, 450–454 19 Wang, P., Chen, J., Zheng, A. et al. (2004) Expression cloning of functional receptor used by SARS coronavirus. Biochem. Biophys. Res. Commun. 315, 439–444 20 Nie, Y., Wang, P., Shi, X. et al. (2004) Highly infectious SARS-CoV pseudotyped virus reveals the cell tropism and its correlation with receptor expression. Biochem. Biophys. Res. Commun. 321, 994–1000 21 Chan, P. K., To, K. F., Lo, A. W. et al. (2004) Persistent infection of SARS coronavirus in colonic cells in vitro. J. Med. Virol. 74, 1–7 22 Jeffers, S. A., Tusell, S. M., Gillim-Ross, L. et al. (2004) CD209L (L-SIGN) is a receptor for severe acute respiratory syndrome coronavirus. Proc. Natl. Acad. Sci. U.S.A. 101, 15748–15753 23 Donnelly, C. A., Ghani, A. V., Leung, G. M. et al. (2003) Epidemiological determinants of spread of causal agent of severe acute respiratory syndrome in Hong Kong. Lancet 361, 1761–1766 24 Twu, S. J., Chen, T. J., Chen, C. J. et al. (2003) Control measures for severe acute respiratory syndrome (SARS) in Taiwan. Emerg. Infect. Dis. 9, 718–720 25 Hui, D. S., Wong, P. C. and Wang, C. (2003) SARS: Clinical features and diagnosis. Respirology 8, S20–S24 26 Leung, W. K., To, K. F., Chan, P. K. et al. (2003) Enteric involvement of severe acute respiratory syndromeassociated coronavirus infection. Gastroenterology 125, 1011–1017 27 Chan, H. L., Kwan, A. C., To, K. F. et al. (2005) Clinical significance of hepatic derangement in severe acute respiratory syndrome. World J. Gastroenterol. 11, 2148–2153 28 Hui, D. S. and Sung, J. J. (2003) Severe acute respiratory syndrome. Chest 124, 12–15 29 Wong, G. W. and Hui, D. S. (2003) Severe acute respiratory syndrome: epidemiology, diagnosis and treatment. Thorax 58, 558–560 30 Wong, K. T., Antonio, G. E., Hui, D. S. et al. (2003) Severe acute respiratory syndrome: radiographic appearances and pattern of progression in 138 patients. Radiology 228, 401–406 31 Peiris, J. S., Chu, C. M., Cheng, V. C. et al. (2003) Clinical progression and viral load in a community outbreak of coronavirus-associated SARS pneumonia: a prospective study. Lancet 361, 1767–1772 32 Gomersall, C. D., Joynt, G. M., Lam, P. et al. (2004) Short-term outcome of critically ill patients with severe acute respiratory syndrome. Intensive Care Med. 30, 381–387 33 Wong, K. T., Antonio, G. E., Hui, D. S. et al. (2003) Thin section CT of Severe Acute Respiratory Syndrome: evaluation of 73 patients exposed to or with the disease. Radiology 228, 395–400 34 Hung, E. C., Chim, S. S., Chan, P. K. et al. (2003) Detection of SARS coronavirus RNA in the cerebrospinal fluid of a patient with severe acute respiratory syndrome. Clin. Chem. 49, 2108–2109 35 Lau, K. K., Yu, W. C., Chu, C. M., Lau, S. T., Sheng, B. and Yuen, K. Y. (2004) Possible central nervous system infection by SARS coronavirus. Emerg. Infect. Dis. 10, 342–344 C 2006 The Biochemical Society 201 202 P. K. S. Chan, J. W. Tang and D. S. C. Hui 36 Wong, K. C., Leung, K. S. and Hui, M. (2003) Severe acute respiratory syndrome (SARS) in a geriatric patient with a hip fracture. A case report. J. Bone Joint Surg. 85A, 1339–1342 37 Tee, A. K., Oh, H. M., Lien, C. T., Narendran, K., Heng, B. H. and Ling, A. E. (2004) Atypical SARS in a geriatric patient. Emerg. Infect. Dis. 10, 261–264 38 Fisher, D. A., Lim, T. K., Lim, Y. T., Singh, K. S. and Tambyah, T. A. (2003) Atypical presentations of SARS. Lancet 361, 1740 39 Hon, K. L., Leung, C. W., Cheng, W. T. et al. (2003) Clinical presentations and outcome of severe acute respiratory syndrome in children. Lancet 561, 1701–1703 40 Sit, S. C., Yau, E. K., Lam, Y. Y. et al. (2003) A young infant with severe acute respiratory syndrome. Pediatrics 112, e257 41 Bitnun, A., Allen, U., Heurter, H. et al. (2003) Children hospitalized with severe acute respiratory syndromerelated illness in Toronto. Pediatrics 112, e261 42 Chiu, W. K., Cheung, P. C., Ng, K. L. et al. (2003) Severe acute respiratory syndrome in children: Experience in a regional hospital in Hong Kong. Pediatr. Crit. Care Med. 4, 279–283 43 Chan, P. K., Ip, M., Ng, K. C. et al. (2003) Severe acute respiratory syndrome-associated coronavirus infection. Emerg. Infect. Dis. 9, 1453–1454 44 Ip, M., Chan, P. K., Lee, N. et al. (2004) Seroprevalence of antibody to severe acute respiratory syndrome (SARS)associated coronavirus among health care workers in SARS and non-SARS medical wards. Clin. Infect. Dis. 38, e116–e118 45 Song, H. D., Tu, C. C., Zhang, G. W. et al. (2005) Cross-host evolution of severe acute respiratory syndrome coronavirus in palm civet and human. Proc. Natl. Acad. Sci. U.S.A. 102, 2430–2435 46 Guan, Y., Zheng, B. J., He, Y. Q. et al. (2003) Isolation and characterization of viruses related to the SARS coronavirus from animals in southern China. Science 302, 276–278 47 The Chinese SARS Molecular Epidemiology Consortium (2004) Molecular evolution of the SARS coronavirus during the course of the SARS epidemic in China. Science 303, 1666–1669 48 Aitken, C. and Jeffries, D. J. (2001) Nosocomial spread of viral disease. Clin. Microbiol. Rev. 14, 528–546 49 Siegel, J., Strausbaugh, L., Jackson, M., Rhinehart, E. and Chiarello, L. A. (2004) Draft guidelines for isolation precautions: preventing transmission of infectious agents in healthcare settings. Recommendations of the Healthcare Infection Control Practices Advisory Committee, (http://hica.jp/cdcguideline/ 2004DraftIsoGuideline.pdf) 50 Hammond, G. W., Raddatz, R. L. and Gelskey, D. E. (1989) Impact of atmospheric dispersion and transport of viral aerosols on the epidemiology of influenza. Rev. Infect. Dis. 11, 494–497 51 Wong, R. S. and Hui, D. S. (2004) Index patient and SARS outbreak in Hong Kong. Emerg. Infect. Dis. 10, 339–341 52 Manocha, S., Walley, K. R. and Russell, J. A. (2003) Severe acute respiratory distress syndrome (SARS): a critical care perspective. Crit. Care Med. 31, 2684–2692 53 Fowler, R. A., Lapinsky, S. E., Hallett, D. et al. (2003) Critically ill patients with severe acute respiratory syndrome. JAMA, J. Am. Med. Assoc. 290, 367–373 54 Lew, T. W., Kwek, T. K., Tai, D. et al. (2003) Acute respiratory distress syndrome in critically ill patients with severe acute respiratory syndrome. JAMA, J. Am. Med. Assoc. 290, 374–380 55 Lapinsky, S. E. and Hawryluck, L. (2003) ICU management of severe acute respiratory syndrome. Intensive Care Med. 29, 870–875 56 Tang, J. W. and Chan, R. C. (2004) Severe acute respiratory syndrome (SARS) in intensive care units (ICUs): Limiting the risk to healthcare workers. Curr. Anaesth. Crit. Care 15, 143–155 57 Yu, I. T., Li, Y., Wong, T. W. et al. (2004) Evidence of airborne transmission of the severe acute respiratory syndrome virus. N. Engl. J. Med. 350, 1731–1739 C 2006 The Biochemical Society 58 Ng, S. K. (2003) Possible role of an animal vector in the SARS outbreak at Amoy Gardens. Lancet 362, 570–572 59 Lee, S. H. (2003) The SARS epidemic in Hong Kong. J. Epidemiol. Community Health 57, 652–654 60 Booth, T. F., Kournikakis, B., Bastien, N. et al. (2005) Detection of airborne Severe acute respiratory syndrome (SARS) coronavirus and environmental contamination in SARS outbreak units. J. Infect. Dis. 191, 1472–1477 61 Yu, I. T., Wong, T. W., Chiu, Y. L., Lee, N. and Li, Y. (2005) Temporal-spatial analysis of severe acute respiratory syndrome among hospital inpatients. Clin. Infect. Dis. 40, 1237–1243 62 Riley, S., Fraser, C., Donnelly, C. A. et al. (2003) Transmission dynamics of the etiological agent of SARS in Hong Kong: impact of public health interventions. Science 300, 1961–1966 63 Lipsitch, M., Cohen, T., Cooper, T. et al. (2003) Transmission dynamics and control of severe acute respiratory syndrome. Science 300, 1966–1970 64 Mims, C., Playfair, J., Roitt, I., Wakelin, D. and Williams, R. (1998) Epidemiologic aspects of the control of infection and disease. In Medical Microbiology, 2nd edn (Mims, C., Playfair, J., Roitt, I., Wakelin, D. and Williams, R., eds.), pp. 467–480, Mosby, London 65 Fraser, C., Riley, S., Anderson, R. M. and Ferguson, N. M. (2004) Factors that make an infectious disease outbreak controllable. Proc. Natl. Acad. Sci. U.S.A. 101, 6146–6151 66 Mills, C. E., Robins, J. M. and Lipsitch, M. (2004) Transmissibility of 1918 pandemic influenza. Nature (London) 432, 904–906 67 Afzelius, B. A. (1994) Ultrastructure of human nasal epithelium during an episode of coronavirus infection. Virchows Arch. 424, 295–300 68 Liu, C., Xu, H. Y. and Liu, D. X. (2001) Induction of caspase-dependent apoptosis in cultured cells by the avian coronavirus infectious bronchitis Virus. J. Virol. 75, 6402–6409 69 Mossel, E. C., Huang, C., Narayanan, K., Makino, S., Tesh, R. B. and Peters, C. J. (2005) Exogenous ACE2 expression allows refractory cell lines to support severe acute respiratory syndrome coronavirus replication. J. Virol. 79, 3846–3850 70 Yan, H., Xiao, G., Zhang, J. et al. (2004) SARS coronavirus induces apoptosis in Vero E6 cells. J. Med. Virol. 73, 323–331 71 Lavi, E., Wang, Q., Weiss, S. R. and Gonatas, N. K. (1996) Syncytia formation induced by coronavirus infection is associated with fragmentation and rearrangement of the Golgi apparatus. Virology 221, 325–334 72 Marten, N. W., Stohlman, S. A. and Bergmann, C. C. (2001) MHV infection of the CNS: mechanisms of immune-mediated control. Viral Immunol. 14, 1–18 73 Ning, Q., Liu, M., Kongkham, P. et al. (1999) The nucleocapsid protein of murine hepatitis virus type 3 induces transcription of the novel fgl2 prothrombinase gene. J. Biol. Chem. 274, 9930–9936 74 Weiss, R. C. and Scott, F. W. (1981) Antibody-mediated enhancement of disease in feline infectious peritonitis: comparisons with dengue hemorrhagic fever. Comp. Immunol. Microbiol. Infect. Dis. 4, 175–189 75 Nicholls, J. M., Poon, L. L., Lee, K. C. et al. (2003) Lung pathology of fatal severe acute respiratory syndrome. Lancet 361, 1773–1778 76 Antonio, G. E., Wong, K. T., Hui, D. S. et al. (2003) Thin-section CT in patients with severe acute respiratory syndrome following hospital discharge: preliminary experience. Radiology 228, 810–815 77 Duan, Z. P., Chen, Y., Zhang, J., Zhao, J., Lang, Z. W., Meng, F. K. and Bao, X. L. (2003) Clinical characteristics and mechanism of liver injury in patients with severe acute respiratory syndrome. Zhonghua Ganzangbing Zazhi 11, 493–496 78 Chan, H. L., Leung, W. K., To, K. F. et al. (2004) Retrospective analysis of liver function derangement in severe acute respiratory syndrome. Am. J. Med. 116, 566–567 SARS: clinical presentation, transmission, pathogenesis and treatment options 79 He, Y., Lu, H., Siddiqui, P., Zhou, Y. and Jiang, S. (2005) Receptor-binding domain of severe acute respiratory syndrome coronavirus spike protein contains multiple conformation-dependent epitopes that induce highly potent neutralizing antibodies. J. Immunol. 174, 4908–4915 80 Sperry, S. M., Kazi, L., Graham, R. L., Baric, R. S., Weiss, S. R. and Denison, M. R. (2005) Single-amino-acid substitutions in open reading frame (ORF) 1b-nsp14 and ORF 2a proteins of the coronavirus mouse hepatitis virus are attenuating in mice. J. Virol. 79, 3391–3400 81 Leparc-Goffart, I., Hingley, S. T., Chua, M. M., Phillips, J., Lavi, E. and Weiss, S. R. (1998) Targeted recombination within the spike gene of murine coronavirus mouse hepatitis virus-A59: Q159 is a determinant of hepatotropism. J. Virol. 72, 9628–9636 82 Ballesteros, M. L., Sanchez, C. M. and Enjuanes, L. (1997) Two amino acid changes at the N-terminus of transmissible gastroenteritis coronavirus spike protein result in the loss of enteric tropism. Virology 227, 378–388 83 Wong, C. K., Lam, C. W., Wu, A. K. et al. (2004) Plasma inflammatory cytokines and chemokines in severe acute respiratory syndrome. Clin. Exp. Immunol. 136, 95–103 84 Jiang, Y., Xu, J., Zhou, C. et al. (2005) Characterization of cytokine/chemokine profiles of severe acute respiratory syndrome. Am. J. Respir. Crit. Care Med. 171, 850–857 85 Huang, K. J., Su, I. J., Theron, M., Wu, Y. C., Lai, S. K., Liu, C. C. and Lei, H. Y. (2005) An interferon-γ -related cytokine storm in SARS patients. J. Med. Virol. 75, 185–194 86 Xie, J., Han, Y., Li, T. S. et al. (2003) Dynamic changes of plasma cytokine levels in patients with severe acute respiratory syndrome. Zhonghua Neike Zazhi 42, 643–645 87 Zhang, Y., Li, J., Zhan, Y. et al. (2004) Analysis of serum cytokines in patients with severe acute respiratory syndrome. Infect. Immun. 72, 4410–4415 88 Li, Z., Guo, X., Hao, W. et al. (2003) The relationship between serum interleukins and T-lymphocyte subsets in patients with severe acute respiratory syndrome. Chin. Med. J. (Engl). 116, 981–984 89 Wang, C., Pang, B. S. and National Research Project for SARS, Beijing Group (2003) Dynamic changes and the meanings of blood cytokines in severe acute respiratory syndrome. Zhonghua Jiehe He Huxi Zazhi 26, 586–589 90 Ng, P. C., Lam, C. W., Li, A. M. et al. (2004) Inflammatory cytokine profile in children with severe acute respiratory syndrome. Pediatrics 113, e7–e14 91 Lydyard, P. M., Whelan, A. and Fanger, M. W (2004) Molecules of the innate immune system. Instant Notes in Immunology, 2nd edn, pp. 23–32, BIOS Scientific Publishers, New York 92 Openshaw, P. J. (2004) What does the peripheral blood tell you in SARS? Clin. Exp. Immunol. 136, 11–12 93 Cinatl, J., Morgenstern, B., Bauer, G., Chandra, P., Rabenau, H. and Doerr, H. W. (2003) Glycyrrhizin, an active component of liquorice roots, and replication of SARS-associated coronavirus. Lancet 361, 2045–2046 94 Tan, E. L., Ooi, E. E., Lin, C. Y., Tan, H. C., Ling, A. E., Lim, B. and Stanton, L. W. (2004) Inhibition of SARS coronavirus infection in vitro with clinically approved antiviral drugs. Emerg. Infect. Dis. 10, 581–586 95 Stroher, U., DiCaro, A., Li, Y. et al. (2004) Severe acute respiratory syndrome-related coronavirus is inhibited by interferon-α. J. Infect. Dis. 189, 1164–1167 96 Sung, J. J., Wu, A., Joynt, G. M. et al. (2004) Severe Acute Respiratory Syndrome: report of treatment and outcome after a major outbreak. Thorax 59, 414–420 97 Ng, E. K., Ng, P. C., Hon, K. L. et al. (2003) Serial analysis of the plasma concentration of SARS coronavirus RNA in pediatric patients with severe acute respiratory syndrome. Clin. Chem. 49, 2085–2088 98 Anand, K., Ziebuhr, J., Wadhwani, P., Mesters, J. R. and Hilgenfeld, R. (2003) Coronavirus main proteinase (3Clpro) structure: basis for design of anti-SARS drugs. Science 300, 1763–1767 99 Chu, C. M., Cheng, V. C., Hung, I. F. et al. (2004) Role of lopinavir/ritonavir in the treatment of SARS: initial virological and clinical findings. Thorax 59, 252–256 100 Chan, K. S., Lai, S. T., Chu, C. M. et al. (2003) Treatment of severe acute respiratory syndrome with lopinavir/ritonavir: a multicenter retrospective matched cohort study. Hong Kong Med. J. 9, 399–406 101 Hurst, M. and Faulds, D. (2000) Lopinavir. Drugs 60, 1371–1381 102 Yamamoto, N., Yang, R., Yoshinaka, Y. et al. (2004) HIV protease inhibitor nelfinavir inhibits replication of SARS-associated coronavirus. Biochem. Biophys. Res. Commun. 318, 719–725 103 Cinatl, J., Morgenstern, B., Bauer, G., Chandra, P., Rabenau, H. and Doerr, H. W. (2003) Treatment of SARS with human interferons. Lancet 362, 293–294 104 Hensley, L. E., Fritz, L. E., Jahrling, P. B., Karp, C. L., Huggins, J. W. and Geisbert, T. W. (2004) Interferon-β1a and SARS coronavirus replication. Emerg. Infect. Dis. 10, 317–319 105 Sainz, Jr, B., Mossel, E. C., Peters, C. J. and Garry, R. F. (2004) Interferon-β and interferon-γ synergistically inhibit the replication of severe acute respiratory syndrome-associated coronavirus (SARS-CoV). Virology 329, 11–17 106 Morgenstern, B., Michaelis, M., Baer, P. C., Doerr, H. W. and Cinatl, Jr, J. (2005) Ribavirin and interferon-beta synergistically inhibit SARS-associated coronavirus replication in animal and human cell lines. Biochem. Biophys. Res. Commun. 326, 905–908 107 Chen, F., Chan, K. H., Jiang, Y. et al. (2005) In vitro susceptibility of 10 clinical isolates of SARS coronavirus to selected antiviral compounds. J. Clin. Virol. 39, 69–75 108 Haagmans, B. L., Kuiken, T., Martina, B. E. et al. (2004) Pegylated interferon-α protects type 1 pneumocytes against SARS coronavirus infection in macaques. Nat. Med. 10, 290–293 109 Loutfy, M. R., Blatt, L. M., Siminovitch, K. A. et al. (2003) Interferon Alfacon-1 plus corticosteroids in severe acute respiratory syndrome: a preliminary study. JAMA, J. Am. Med. Assoc. 290, 3222–3228 110 Sui, J., Li, W., Murakami, A. et al. (2004) Potent neutralization of severe acute respiratory syndrome (SARS) coronavirus by a human mAb to S1 protein that blocks receptor association. Proc. Natl. Acad. Sci. U.S.A. 101, 2536–2541 111 ter Meulen, J., Bakker, A. B., van den Brink, E. N. et al. (2004) Human monoclonal antibody as prophylaxis for SARS coronavirus infection in ferrets. Lancet 363, 2139–2141 112 Gao, W., Tamin, A., Soloff, A. et al. (2003) Effects of a SARS-associated coronavirus vaccine in monkeys. Lancet 362, 1895–1896 113 Zhao, P., Ke, J. S., Qin, Z. L. et al. (2004) DNA vaccine of SARS-CoV S gene induces antibody response in mice. Acta Biochim. Biophys. Sin. (Shanghai) 36, 37–41 114 Yang, Z. Y., Kong, W. P., Huang, Y. et al. (2004) A DNA vaccine induces SARS coronavirus neutralization and protective immunity in mice. Nature (London) 428, 561–564 115 Ho, T. Y., Wu, S. L., Cheng, S. E., Wei, Y. C., Huang, S. P. and Hsiang, C. Y. (2004) Antigenicity and receptorbinding ability of recombinant SARS coronavirus spike protein. Biochem. Biophys. Res. Commun. 313, 938–947 116 Bisht, H., Roberts, A., Vogel, L. et al. (2004) Severe acute respiratory syndrome coronavirus spike protein expressed by attenuated vaccinia virus protectively immunizes mice. Proc. Natl. Acad. Sci. U.S.A. 101, 6641–6646 117 Bukreyev, A., Lamirande, E. W., Buchholz, U. J. et al. (2004) Mucosal immunisation of African green monkeys (Cercopithecus aethiops) with an attenuated parainfluenza virus expressing the SARS coronavirus spike protein for the prevention of SARS. Lancet 363, 2122–2127 118 Bosch, B. J., Martina, B. E., van der Zee, R. et al. (2004) Severe acute respiratory syndrome coronavirus (SARS-CoV) infection inhibition using spike protein heptad repeat-derived peptides. Proc. Natl. Acad. Sci. U.S.A. 101, 8455–8460 C 2006 The Biochemical Society 203 204 P. K. S. Chan, J. W. Tang and D. S. C. Hui 119 Choy, W. Y., Lin, S. G., Chan, P. K. et al. (2004) Synthetic peptide studies on the severe acute respiratory syndrome (SARS) coronavirus spike glycoprotein: perspective for SARS vaccine development. Clin. Chem. 50, 1036–1042 120 Ho, J. C., Ooi, G. C., Mok, T. Y. et al. (2003) High dose pulse versus non-pulse corticosteroid regimens in severe acute respiratory syndrome. Am. J. Respir. Crit. Care Med. 168, 1449–1456 121 Tsang, O. T., Chau, T. N., Choi, K. W. et al. (2003) Coronavirus-positive nasopharyngeal aspirate as predictor for severe acute respiratory syndrome mortality. Emerg. Infect. Dis. 9, 1381–1387 122 Wang, H., Ding, Y., Li, X., Yang, L., Zhang, W. and Kang, W. (2003) Fatal aspergillosis in a patient with SARS who was treated with corticosteroids. N. Engl. J. Med. 349, 507–508 123 Hong, N. and Du, X. K. (2004) Avascular necrosis of bone in severe acute respiratory syndrome. Clin. Radiol. 59, 602–608 124 Griffith, J. F., Antonio, G. E., Kumta, S. M. et al. (2005) Osteonecrosis of hip and knee in patients with severe acute respiratory syndrome treated with steroids. Radiology 235, 168–175 125 Lee, N., Allen Chan, K. C., Hui, D. S. et al. (2004) Effects of early corticosteroid treatment on plasma SARSassociated Coronavirus RNA concentrations in adult patients. J. Clin. Virol. 31, 304–309 126 Cheng, Y., Wong, R., Soo, Y. O. et al. (2005) Use of convalescent plasma therapy in SARS patients in Hong Kong. Eur. J. Clin. Microbiol. Infect. Dis. 24, 44–46 127 Soo, Y. O., Cheng, Y., Wong, R. et al. (2004) Retrospective comparison of convalescent plasma with continuing high-dose methylprednisolone treatment in SARS patients. Clin. Microbiol. Infect. 10, 676–678 128 Liu, B. Y., Hu, J. Q., Xie, Y. M. et al. (2004) Effects of integrative Chinese and Western medicine on arterial oxygen saturation in patients with severe acute respiratory syndrome. Chin. J. Integrative Med. 10, 117–122 129 Ballow, M. (1997) Mechanisms of action of intravenous immune serum globulin in autoimmune and inflammatory diseases. J. Allergy Clin. Immunol. 100, 151–157 130 Chong, P. Y., Chui, P., Ling, A. E. et al. (2004) Analysis of deaths during the severe acute respiratory syndrome (SARS) epidemic in Singapore: challenges in determining a SARS diagnosis. Arch. Pathol. Lab. Med. 128, 195–204 131 Umapathi, T., Kor, A. C., Venketasubramanian, N. et al. (2004) Large artery ischaemic stroke in severe acute respiratory syndrome (SARS). J. Neurol. 251, 1227–1231 132 Ho, J. C., Wu, A. Y., Lam, B. et al. (2004) Pentaglobin in steroid-resistant severe acute respiratory syndrome. Int. J. Tuberc. Lung Dis. 8, 1173–1179 133 Ng, K. H., Wu, A. K., Cheng, V. C. et al. (2005) Pulmonary artery thrombosis in a patient with severe acute respiratory syndrome. Postgrad. Med. J. 81, e3 134 Dalakas, M. C. and Clark, W. M. (2003) Strokes, thromboembolic events, and IVIg: rare incidents blemish an excellent safety record. Neurology 60, 1763–1767 135 Chen, L., Liu, P., Gao, H. et al. (2004) Inhalation of nitric oxide in the treatment of severe acute respiratory syndrome: a rescue trial in Beijing. Clin. Infect. Dis. 39, 1531–1535 136 Akerstrom, S., Mousavi-Jazi, M., Klingstrom, J., Leijon, M., Lunddvist, A. and Mirazimi, A. (2005) Nitric oxide inhibits the replication cycle of severe acute respiratory syndrome coronavirus. J. Virol. 79, 1966–1969 137 Fowler, R. A., Guest, C. B., Lapinsky, S. E. et al. (2004) Transmission of severe acute respiratory syndrome during intubation and mechanical ventilation. Am. J. Respir. Crit. Care Med. 169, 1198–1202 138 Cheung, T. M., Yam, L. Y., So, L. K. et al. (2004) Effectiveness of noninvasive positive pressure ventilation in the treatment of acute respiratory failure in severe acute respiratory syndrome. Chest 126, 845–850 139 Hui, D. S. and Sung, J. J. (2004) Treatment of Severe acute respiratory syndrome. Chest 126, 670–674 140 Reference deleted 141 Tsui, P. T., Kwok, M. L., Yuen, H. and Lai, S. T. (2003) Severe acute respiratory syndrome: clinical outcome and prognostic correlates. Emerg. Infect. Dis. 9, 1064–1069 142 Chan, J. W., Ng, C. K., Chan, Y. H. et al. (2003) Short term outcome and risk factors for adverse clinical outcomes in adults with severe acute respiratory syndrome (SARS). Thorax 58, 686–689 143 Wong, R. S., Wu, A., To, K. F. et al. (2003) Haematological manifestations in patients with severe acute respiratory syndrome: retrospective analysis. Br. Med. J. 326, 1358–1362 144 Chu, C. M., Poon, L. L., Cheng, V. C. et al. (2004) Initial viral load and the outcomes of SARS. Can. Med. Assoc. J. 171, 1349–1352 145 Hui, D. S., Joynt, G. M., Wong, K. T. et al. (2005) Impact of severe acute respiratory syndrome (SARS) on pulmonary function, functional capacity and quality of life in a cohort of survivors. Thorax 60, 401–409 146 Hui, D. S., Wong, K. T., Ko, F. W. et al. (2005) The one-year impact of severe acute respiratory syndrome (SARS) on pulmonary function, exercise capacity and quality of life in a cohort of survivors. Chest 128, 2247–2261 147 Tsai, L. K., Hsieh, S. T., Chao, C. C. et al. (2004) Neuromuscular disorders in severe acute respiratory syndrome. Arch. Neurol. 61, 1669–1673 148 Yu, W. C., Hui, D. S. and Chan-Yeung, M. (2004) Antiviral agents and corticosteroids in the treatment of SARS. Thorax 59, 643–645 149 Tsang, K. W., Ooi, G. C. and Ho, P. L. (2004) Diagnosis and pharmacotherapy of severe acute respiratory syndrome: what have we learnt? Eur. Respir. J. 24, 1025–1032 150 Chua, S. E., Cheung, V., McAlonan, G. M. et al. (2004) Stress and psychological impact on SARS patients during the outbreak. Can. J. Psychiatry 49, 385–390 151 Cheng, S. K., Wong, C. W., Tsang, J. and Wong, K. C. (2004) Psychological distress and negative appraisals in survivors of severe acute respiratory syndrome (SARS). Psychol. Med. 34, 1187–1195 152 Lee, D. T., Wing, Y. K., Leung, H. C. et al. (2004) Factors associated with psychosis among patients with severe acute respiratory syndrome: a case-control study. Clin. Infect. Dis. 39, 1247–1249 Received 13 June 2005/21 June 2005; accepted 4 July 2005 Published on the Internet 17 January 2006, doi:10.1042/CS20050188 C 2006 The Biochemical Society