Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
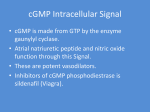
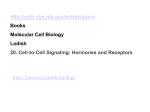
MEDICINE REVIEW ARTICLE Tyrosine Kinases Are the Targets of New Treatments in Oncology Carsten Müller-Tidow, Utz Krug, Uta Brunnberg, Wolfgang E. Berdel, Hubert Serve SUMMARY Introduction: Tyrosine kinases are involved in the pathogenesis of many malignancies. Their inhibition via monoclonal antibodies or small inhibitory molecules is therefore of great interest. This article reviews those tyrosine kinase inhibitors in clinical use, and the problems evolving from their development and use. Methods: Selective review of literature relating to the pathological activation of tyrosine kinases in malignant diseases and the indication, effect and toxicity profile of tyrosine kinase inhibitors. Results and discussion: Inhibitory components have been developed for many tyrosine kinases. These are effective when the tumor is addicted to the tyrosine kinase activity. In addition, tyrosine kinase inhibitors display different, and often unpredictable, toxicity profiles compared to classical cytostatic compounds. Many malignant diseases are heterogeneous at the molecular level. This raises problems in clinical studies with tyrosine kinase inhibitors since they are effective only in molecularly defined subgroups of patients. Dtsch Arztebl 2007; 104:(19) A 1312–9. Key words: tyrosine kinase, cancer therapy, inhibitor of cell signals, monoclonal antibody T yrosine kinases are enzymes that catalyze the modification of substrates by the addition of a phosphate group. Approximately 90 tyrosine kinases are encoded in the human genome, of which 58 are receptor tyrosine kinases on cell surfaces (1). Diagram 1 schematically depicts signal transduction by means of a receptor tyrosine kinase. Activation is induced by the binding of a specific ligand. The ensuing signal transduction leads to cell proliferation and tissue regeneration, or else inhibits programmed cell death and thereby promotes cell survival. The other types of tyrosine kinases are located in the cytoplasm or cell nucleus and are also activated by phosphorylation as part of a signal transduction pathway. Tyrosine kinases are involved in the pathogenesis of malignant tumors through a number of mechanisms. A balanced translocation may cause a tyrosine kinase to fuse with a bridging protein, so that the fusion protein then becomes oligomerized and thereby permanently activated. In diagram 2, this mechanism is illustrated in the specific case of the BCR-ABL fusion protein found in Philadelphia-chromosome-positive chronic myeloid leukemia. Activation can also be caused by mutations, such as the activating Flt3 mutations. These mutations of the Flt3 receptor tyrosine kinase cause permanent, ligandindependent activation. A further way in which tyrosine kinases can be activated in malignant cells is by overexpression, e.g., by gene amplification. In carcinomas, this mechanism is of great importance for the epidermal growth factor receptor (EGFR) and the related ERBB2/Her2/Neu and ERBB3 receptors (table 1). Alternatively, receptor tyrosine kinases can be activated to a greater extent than normal if the ligands that activate them are overexpressed, either in the tumor cells themselves or in the surrounding stromal tissue. Potential means of pharmacological blockade of tyrosine kinases are depicted in diagrams 1 and 2. These include monoclonal antibodies against receptor tyrosine kinases, anti-ligand antibodies, and small molecules that inhibit ATP binding. The rest of this paper will provide an overview of the inhibitors that are currently in clinical use. Universitätsklinikum Münster, Medizinische Klinik und Poliklinik A, Münster: PD Dr. med. Müller-Tidow, Dr. med. Krug, Dr. med. Brunnberg, Prof. Dr. med. Berdel, Prof. Dr. med. Serve Dtsch Arztebl 2007; 104(19): A 1312–9 ⏐ www.aerzteblatt.de 1 MEDICINE Monoclonal antibodies Monoclonal antibodies against receptor tyrosine kinases are directed against the extracellular ligand-binding site and block the binding of the ligand to its receptor (diagram 1). The first effective treatment with tyrosine kinase inhibition involved the monoclonal antibody trastuzumab (2), which binds to the receptor tyrosine kinase ERBB2, to treat women with breast cancer in which this receptor is overexpressed. The rationale behind this therapy is that ERBB2 is overexpressed in about 15% to 30% of breast cancers, and overexpression is associated with a poor prognosis (e1). DIAGRAM 1 Signal transduction by receptor tyrosine kinases. After a specific ligand (growth factor, GF) binds to the receptor, the receptor tyrosine kinase is dimerized; activation by autophosphorylation of tyrosine residues then ensues, followed by activation of substrate proteins by tyrosine phosphorylation. Downsteam signal transduction pathways are then activated (left half of diagram at right). Ligand binding can be blocked by monoclonal antibodies directed against either the extracellular domain of the receptor tyrosine kinase or the ligand, while receptor tyrosine kinase inhibitors (RTKI) of low molecular weight inhibit kinase activity by binding to the ATP binding site of the receptor tyrosine kinase (right half of diagram at right). Women with metastatic breast cancer with overexpression of ERBB2 now receive trastuzumab as part of their standard treatment, in combination with chemotherapy, and show an increase of their overall survival of 5 to 10 months as a result. The monoclonal antibody can be given as monotherapy or in combination with cytostatic agents. At present, preliminary analyses are available of four large randomized studies, and one small one, concerning the adjuvant therapy of women with breast cancer with ERBB2 overexpression in combination with, or immediately after, cytostatic treatment. These studies included a total of 14 079 patients (3). Relapse-free survival was found to be significantly increased by trastuzumab in all studies, with median follow-up times of 1 to 3 years. In the National Surgical Adjuvant Breast and Bowel Project (NSABP) B-31 study and the North Central Cancer Treatment Group (NCCTG) N9831 study, taken together, the absolute increase in three-year relapse-free survival was 12%, with a total of 5 535 patients participating. In the Herceptin Adjuvant (HERA) study with 5 090 evaluated patients the absolute increase in two-year relapse-free survival was 8.4%. Data on a possible increase in overall survival are still lacking for this group of patients at relatively low risk because of the short Dtsch Arztebl 2007; 104(19): A 1312–9 ⏐ www.aerzteblatt.de 2 MEDICINE DIAGRAM 2 Signal transduction by BCR-ABL. (a) The balanced translocation t(9;22) leads to the formation of the fusion protein BCR-ABL. (b) The fusion protein becomes dimerized with another fusion protein by the dimerization domain DD. Dimerization activates the ABL kinase, resulting in the phosphorylation of substrate proteins and proteins downstream the signal transduction pathways (left half of diagram). Imatinib, like a low molecular weight receptor tyrosine kinase inhibitor, binds to the ATP binding site of the ABL domain, with resulting active inhibition of substrate protein phosphorylation (right half of diagram). Secondary mutations of the ATP binding site may prevent imatinib binding to the ATP binding site of BCR-ABL, conferring resistance to imatinib (this mechanism is not pictorially shown in the figure). follow-up to date; nonetheless, it can be predicted that a long-term benefit will be demonstrated, and that this substance will therefore become part of the standard adjuvant treatment of women with breast cancer with overexpression of ERBB2. Trastuzumab, like the majority of specific agents, mostly lacks the side effects classically associated with cytostatic drugs, such as hair loss, but antibodies can be expected to induce allergic reactions in some cases. Moreover, antibodies against receptor tyrosine kinases interfere with physiological signal transduction pathways and are therefore likely to cause other, unexpected side effects. In particular, trastuzumab can be toxic to the heart, causing heart failure and arrhythmia; when it is given in combination with anthracyclines – the most effective classic chemotherapeutic agent against breast cancer – these problems arise in up to 30% of patients (table 2). Trastuzumab should therefore not be combined with anthracyclines, except in the framework of clinical studies. Trastuzumab seems to be ineffective against other types of tumor in which ERBB2 is overexpressed, e.g., lung cancer (e2–e4). The epidermal growth factor receptor (EGFR) is overexpressed in many types of carcinoma, and, in many of them, EGFR overexpression is correlated with a poor prognosis (4). Cetuximab, a monoclonal antibody directed against this receptor, has been approved for combination therapy, together with irinotecan, in patients with metastatic colon carcinoma with overexpression of EGFR after failure of chemotherapy including irinotecan. The randomized phase 3 study of Cunningham et al. (5) documented a response rate of 22.9% and a mean survival time of 8.4 months in the combination treatment arm of the study. The study design can be criticized, however, because combination therapy was only compared with cetuximab monotherapy, so that no definite statement can be made regarding a possible Dtsch Arztebl 2007; 104(19): A 1312–9 ⏐ www.aerzteblatt.de 3 MEDICINE prolongation of survival by the use of this substance. About 80% of all patients taking cetuximab develop acne; other undesired side effects are allergic reactions (as with other types of antibodies), including bronchospasm, and abdominal pain in ca. 5% of patients (table 2). Responsiveness to cetuximab is correlated with acne but not with the presence or extent of EGFR expression; therefore, the approval only for the treatment of patients with tumors that overexpress EGFR seems not reasonable. Clinical studies are now in progress to investigate other potential indications for cetuximab, including non-small-cell lung cancer (NSCLC), carcinoma of the pancreas, cervical carcinoma, multiple myeloma, metastatic breast cancer, head and neck tumors (for which the substance has already been approved in the USA), esophageal and gastric carcinoma, glioblastoma multiforme, hepatocellular carcinoma, squamous cell carcinoma of the skin, and soft tissue sarcomas. Receptor tyrosine kinase activity can also be inhibited by neutralization of the ligand (diagram 1). Many studies, with various types of tumor, have revealed a correlation between the serum concentration of vascular endothelial growth factor (VEGF) and tumor stage and/or disease prognosis (6). By activating the VEGF receptor family, VEGF stimulates neoangiogenesis within tumors and thus increases the blood supply of cancerous tissue. Bevacizumab, a monoclonal antibody that neutralizes VEGF, has been approved for the treatment of patients with metastatic colorectal tumors in combination with first-line chemotherapy. When given in combination with chemotherapy including irinotecan, bevacizumab prolongs survival from 15.6 to 20.3 months (7). Furthermore, randomized phase 2 and/or phase 3 studies have shown that bevacizumab prolongs progression-free survival from 2.5 to 4.9 months in patients with metastatic renal cell carcinoma (8), and that it prolongs overall survival by two months in patients with any type of non-small-cell lung cancer (NSCLC) other than squamous cell carcinoma (9). In women with metastatic breast cancer, the addition of bevacizumab to first-line therapy with paclitaxel was found to prolong progression-free survival from 6.1 to 11 months (10). The major side effects of bevacizumab are arterial hypertension and hemoptysis, which can be fatal, in patients with squamous cell carcinoma of the lung. Therefore, patients with the latter type of tumor were excluded from studies of the treatment of NSCLC with bevacizumab (table 2). Small inhibitory molecules In addition to therapeutically effective monoclonal antibodies, specific inhibitors of tyrosine kinase domains are now also available. The prototype of these inhibitor molecules is imatinib, a drug that binds with high specificity to the ATP binding site of the tyrosine kinase abl and also binds to the receptor tyrosine kinases c-kit and PDGFRbeta (11), thereby inhibiting tyrosine kinase activity. The first type of cancer that was found to be treatable in this way was chronic myeloid leukemia (CML); in CML, permanent activation of the abl tyrosine kinase in the BCR-ABL fusion protein is the causative transforming mechanism (diagram 2). More than 95% of patients in the chronic phase of the disease attain a complete hematologic remission when treated with imatinib, and many (ca. 75%) also have a complete cytogenetic remission (12). The common side effects of imatinib include edema (mainly of the eyelids), nausea, and muscle cramps in about 50% of patients and myalgia, arthralgia, abdominal pain, gynecomastia, rash, diarrhea, and weight gain in 10% to <50%. 0.1% to 1% of CML patients taking imatinib develop heart failure; this side effect is more common in patients with preexisting hypertension, diabetes mellitus, or coronary heart disease (e5). The major hematologic toxicity of imatinib, occurring in about 10% of patients, is marked neutropenia. Its non-hematologic toxic effects are usually mild, and imatinib is thus both significantly more effective and significantly better tolerated than the standard, conventional treatment of CML with interferon alpha (table 2). Because of this, and because of the markedly higher toxicity of allogenic bone marrow or stem cell transplantation, the use of imatinib has now become the standard initial therapy of CML in chronic phase. In most patients, however, treatment with imatinib does not eradicate the malignant clone. Furthermore, resistance to imatinib can develop through a number of mechanisms, among them point mutations of the tyrosine kinase domain in bcr-abl (13). These mutations render the imatinib molecule unable to bind to the active center, so that it becomes ineffective as an inhibitor. Dasatinib, a further tyrosine kinase inhibitor that is effective despite most of the known point mutations (14), was approved in June 2006 for use in the USA but has not yet been approved in Europe. Dtsch Arztebl 2007; 104(19): A 1312–9 ⏐ www.aerzteblatt.de 4 MEDICINE TABLE 1 Target structures of tyrosine kinases in malignant diseases Tyrosine kinase Diseases Mechanism of activation Specific treatment BCR-ABL ALL, AML, CML t(9;22) imatinib, dasatinib NUP 214-ABL T-ALL episomal fusion and amplification imatinib ABL (9q34) ALK (2p23) NPM-ALK ALCL t(2;5) TPM3-ALK, TPM4-ALK ALCL, IMT t(1;2) ATIC-ALK ALCL inv(2) CARS-ALK IMT t(2;11;2) CLTC-ALK ALCL, IMT t(2;17) TEL-ARG AML t(1;12) imatinib EGFR (7p12) NSCLC, CRC, breast Ca, GBM L858R, L861Q, G719C, G719S, overexpression, deletion cetuximab (only with overexpression), gefitinib, erlotinib ERBB3 (12q13) soft-tissue sarcoma overexpression ZNF198-FGFR1 EMS t(8;13) FOP-FGFR1 EMS t(6;8) CEP110-FGFR1 EMS t(8;9) HERVK-FGFR1 EMS t(8;19) BCR-FGFR1 aCML t(8;22) multiple myeloma overexpression with t(4;14); K650E PD0173074, SU5402 T-cell lymphoma t(4;12) DP0173074, Su5402 FLT3 (13q12) AML internal tandem duplication in the juxtamembranous region; D835X; overexpression PKC412, MLN518, CEP-701, SU5416 c-FMS (5q33) MDS, AML L301F/S; Y969C HER2 (17q21) breast Ca, NSCLC overexpression, activating mutation ARG (1q25) FGFR1 (8p11) FGFR3 (4p16) TEL-FGFR3 JAK2 (9p24) TEL-JAK2 BCR-JAK2 cMPS V617F AML, ALL t(9;12) aCML t(9;22) c-KIT (4q11) AML, GIST, seminoma, activating mutations, sarcomas, SM overexpression c-MET (7q31) musculoskeletal tumors, SCLC, RPC overexpression, expression of a truncated variant, activating mutation gastric carcinoma t(1;7) TPR-MET NTRK1 (1q23) PKC412, PD0173074 trastuzumab, pertuzumab (only with overexpression) imatinib (not for D816X), SU5416, PKC412 PTC, neuroblastoma TPM3-NTRK1 TRP-NTKR1 TFG-NTKR1 PTC t(1;1) t(1;1) t(1;3) AML, CFS, MBN, SJM t(12;15) GBM, osteosarcoma, PAIS, GIST overexpression, activating mutation, deletion NTRK3 (15q25) TEL-NTRK3 α (4q12) PDGFRα Dtsch Arztebl 2007; 104(19): A 1312–9 ⏐ www.aerzteblatt.de 5 MEDICINE TABLE 1 (continuation) Target structures of tyrosine kinases in malignant diseases Tyrosine kinase Diseases Mechanism of activation Specific treatment FIP1L1-PDGFRα HES, GIST interstitial deletion (4q12) imatinib BCR-PDGFRα aCML t(4;22) imatinib COLIα1 DFSP t(17;22) imatinib TEL-PDGFRβ CMML t(5;12) imatinib HIP1-PDGFRβ CMML t(5;7) imatinib Rabaptin5PDGFRβ CMML t(5;17) imatinib H4-PDGFRβ aCML t(5;10) imatinib CEV14-PDGFRβ AML t(5;14) imatinib MEN-2a, MEN-2b, FMTC activating mutation RET-PTC1 PTC inv(10) ZD6474 RET-PTC2 PTC t(10;17) ZD6474 RET-PTC3 PTC inv(10) ZD6474 FIG-ROS GBM, astrocytoma del(6) TEL-SYK MDS t(9;12) RCC, NSCLC, breast Ca, prostate Ca, CRC VEGF overexpression β (5q33) PDGFRβ RET (10q11) ROS (6q22) SYK (9q22) VEGFR bevacizumab, sunitinib aCML, atypical CML; ALCL, anaplastic large-cell non-Hodgkin's lymphoma; ALL, acute lymphoblastic leukemia; AML, acute myeloid leukemia; CFS, congenital infantile fibrosarcoma; CML, chronic myeloid leukemia; CMML, chronic myelomonocytic leukemia; cMPS, chronic myeloproliferative syndrome; CRC, colorectal carcinoma; DFSP, dermatofibrosarcoma protuberans; EMS, 8p11 myeloproliferative syndrome; FMTC, familial medullary carcinoma of the thyroid; GBM, glioblastoma multiforme; GIST, gastrointestinal stromal tumor; HES, hypereosinophilic syndrome; IMT, inflammatory myofibroblastic tumor; MBN, mesoblastic nephroma; MDS, myelodysplastic syndrome; MEN, multiple endocrine neoplasia; NSCLC, non-small-cell lung cancer; PAIS, leiomyosarcoma of the pulmonary artery; PTC, papillary carcinoma of the thyroid; RCC, renal cell carcinoma; RPC, renal papillary carcinoma; SJM, secretory juvenile carcinoma of the breast; SCLC, small-cell lung cancer; SM, systemic mastocytosis. Imatinib inhibits not only abl tyrosine kinase, but also the PDGFR tyrosine kinases (alpha and beta) and c-kit (11). Thus, it has been shown that imatinib can be used successfully against hematologic disorders associated with a balanced translocation for PDGFRß (e.g., Tel-PDGFRbeta) or Abl (table 1), as well as in patients with gastrointestinal stromal tumors (GIST), of whom approximately 80% harbor a mutation of the receptor tyrosine kinase c-kit, while 5% to 10% harbor mutations of PDGFRalpha (15). Before imatinib was introduced, there was no good option for the pharmacotherapy of these patients; under treatment with imatinib, 50% achieve full or partial remission and 33% achieve potentially long-lasting stability of their disease. Once the success of imatinib had been demonstrated, many other tyrosine kinase inhibitors were clinically tested, and some were introduced into clinical practice. The EGFR inhibitors gefitinib and erlotinib were tested as a potential second line of therapy for patients with NSCLC but were found to be only mildly effective. For erlotinib, but not for gefitinib, a randomized, placebo-controlled study revealed a small but statistically significant prolongation of survival by two months in patients taking the drug (16). Nonetheless, a small subgroup of tumors (<10% in Europe, 30% in Asia) responds quite favorably to gefitinib and erlotinib. The percentage of responsive tumors is higher among women, nonsmokers, patients with adenocarcinoma, and patients of Asian descent. The response to gefitinib is correlated with the demonstration of activating mutations in the tyrosine kinase domain of the EGF receptor; the response rate in patients whose tumors harbor such mutations is greater than 60% (17). Gefitinib, like the EGFR-antibody cetuximab, causes acneiform skin changes in most patients, as well as diarrhea in ca. 50% (table 2). A rare but Dtsch Arztebl 2007; 104(19): A 1312–9 ⏐ www.aerzteblatt.de 6 MEDICINE severe complication is interstitial pneumonitis, which arises in about 1% of patients treated with gefitinib and is lethal for some 30% of these patients (18). Interstitial pneumonitis is much rarer as a complication of erlotinib or cetuximab. Inhibitors of the tyrosine kinase domain, with varying degrees of specificity, have also been developed for the receptor tyrosine kinases of the VEGF receptor family. The indole derivative SU11248 (sunitinib) inhibits all VEGF receptor subtypes and PDGF receptors (e6). In a recent randomized study of patients with metastatic renal cell carcinoma, sunitinib was found to be superior to the current standard treatment with interferon with respect to the objective response rate (31% vs. 6%) as well as progression-free survival (11 vs. 5 months) (19). Patients with imatinib-resistant gastrointestinal stromal tumors lived longer; this finding led to the approval of the drug for this indication in the USA (20). Typical side effects of sunitinib include diarrhea, stomatitis, and alterations of taste (table 2). Sorafenib (BAY 43-9006), a multi-kinase inhibitor that can be given orally, was originally developed as an inhibitor of the signal transduction molecule Raf-1. It also inhibits subtypes of the VEGF receptor family, the PDGF receptor, Flt3, and c-kit (e7). Sorafenib was approved as a second-line treatment of patients with metastatic renal cell carcinoma after having been found, in a randomized phase 3 study, to double the progressionfree survival time from 12 months (with placebo) to 24 months (21). Its common side effects in this study were rash, a hand-foot syndrome, and chronic exhaustion (table 2). The possibility of inhibiting multiple receptor tyrosine kinases with a combination of drugs is of particular interest. Initial phase 1 and phase 2 studies of erlotinib combined with TABLE 2 Side effects of tyrosine kinase inhibitors Substance Side effects (frequency) Bevacizumab Hemorrhage1 (20–40%), hypertension (9–27%)2, including hypertensive encephalopathy, diarrhea (8%)2, arterial thromboembolism (2%)2, venous thrombosis (2%)2, gastrointestinal perforation (2–6%), reversible posterior leukoencephalopathy syndrome, wound healing disorders3 Cetuximab Rash (80%), hypomagnesemia (48%), pain incl. abdominal pain (ca. 40%), infusion reaction, fever (ca. 40%), constipation (30%), nausea/vomiting (20–30%), anorexia (20%), infections (10%), conjunctivitis (5%) Erlotinib Rash (75%), diarrhea (54%), anorexia (52%), dyspnea (41%), nausea/vomiting (33%), infections (24%), stomatitis (17%), conjunctivitis, keratocojunctivitis sicca (12%), abdominal pain (11%), interstitial pneumonitis (0.6–0.8%) Gefitinib Rash (45–62%), diarrhea (40–57%), nausea (12%), anorexia (7%), interstitial pneumonitis (1%) Imatinib Nausea/vomiting (50–60%), edema, weight gain (ca. 50%), muscle cramps/myalgia (ca. 50%), diarrhea (25%), rash (25%), gynecomastia (ca. 20%), chronic fatigue (15%), abdominal pain (14%), myelosuppression (10–15%), headache (11%), heart failure (0.1–1%), liver failure4 (case reports), intratumoral hemorrhage (very rare, only in GIST), hypothyroidism (only in patients who have undergone thyroidectomy and are receiving hormone substitution) Sorafenib Hypophosphatemia (45%), rash (43%), diarrhea (38%), chronic exhaustion (37%), alopecia (25%), leucopenia (23%), hand-foot syndrome (19%), hypertension (17%), nausea/vomiting (16%), hemorrhage (15%), myocardial infarction (3%) Sunitinib Fatigue (48%), diarrhea (39%), nausea/vomiting (35%), skin discoloration (29%), abnormal taste (28%), stomatitis (27%), hypertension (22%), anorexia (21%), hand-foot syndrome (17%), rash (17%), myelosuppression (10-15%), chest pain (11%), constipation (10%), intratumoral hemorrhage (2% of GIST tumors) Trastuzumab Pain (head, abdomen, back) (47%), nausea/vomiting (5–33%), fever, shaking chills (5–30%), diarrhea (7–25%), heart failure (7–21%)5, pulmonary reactions incl. dyspnea, bronchospasm, pleural effusion, pneumonitis, ARDS6 (8–22%), infections (20%), rash (3–18%), leucopenia (3–18%)2, paresthesiae (6–11%)2, absolute tachyarrhythmia (5–8%)2, hypersensitivity reaction (3–6%)2 1Mainly epistaxis, pulmonary hemorrhage (sometimes fatal); not to be used in patients with squamous cell carcinoma of the lung 2Excess toxicity compared to a control group (chemotherapy alone) 3No major surgery from 28 days before to 28 days after treatment with bevacizumab 4Not to be given in combination with paracetamol 5Careful monitoring of cardiac function, not to be combined with anthracyclines 6Trastuzumab should not be given to patients with dyspnea at rest ARDS = acute respiratory distress syndrome Dtsch Arztebl 2007; 104(19): A 1312–9 ⏐ www.aerzteblatt.de 7 MEDICINE bevacizumab have already been carried out in patients with advanced, refractory NSCLC (22) and renal cell carcinoma (23). The combined use of two therapeutic agents can circumvent mechanisms of drug resistance, as for example when an inhibition of EGFR is met with increased activity of VEGF signal transduction. Combination therapy can, however, cause unexpected and greater than merely additive toxicity because of the increased interference with the normal pathways of signal transduction. Problems and prospects Special considerations relating to tailored treatment with tyrosine kinase inhibitors require that studies be designed more carefully than classic clinical studies of chemotherapy (24, 25). For example, because of the low toxicity of imatinib in phase 1 studies, its maximal tolerable dose (MTD) could not be determined. Instead, studies of in vivo inhibition of the target tyrosine kinase, e.g., in tissue specimens, offer a way to determine the optimal biological dose (OBD). In phase 2 and phase 3 studies, the medication should ideally be given only to patients whose tumors are addicted to the activity of the target molecule. The disappointing results of EGFR inhibition in tumors that overexpress EGFR imply that verexpression cannot be taken to imply a dependence of tumor growth on the overexpressed enzyme (25). Genetically defined subclasses of tumors, if these have been discovered at all, often include only a small minority of patients with any particular type of tumor. Two further problems result from this. First, when the indication for a new substance is restricted to a small subset of patients with a specifically defined genetic lesion, the high costs of the drug development and approval process make research into the substance financially unattractive for the pharmaceutical industry, whose interest lies in obtaining approval for its use in as many patients as possible, i.e., in a large, relatively unselected patient population. Second, an adequate number of patients with rare, specific genetic lesions can only be recruited in the context of multicenter, international studies. The current preference for tailored therapeutic approaches will require both a better understanding of tumor biology and a closer cooperation of teams from multiple disciplines, including molecular biologists. The successful treatment of patients with balanced translocations and mutations in the tyrosine kinase domain with tyrosine kinase inhibitors is an encouraging start. Cancer biology currently needs new, productive synergies between molecular diagnosis and treatment design. Tyrosine kinase inhibitors represent one step toward the ultimate goal of better tailored, safer, and more effective pharmacological treatment of malignant disease. Conflict of Interest Statement Prof. Serve has received study support from Bayer AG. PD Dr. Müller-Tidow was supported in his research by Novartis. Prof. Berdel has received support for studies and research, as well as lecture and consulting fees, from AstraZeneca, Merck Germany, Bayer, Pfizer, Novartis, Roche/Genentech, and Amgen. Dr. Krug and Dr. Brunnberg state that they have no conflict of interest as defined by the Guidelines of the International Committee of Medical Journal Editors. Manuscript received on 26 April 2006, final version accepted on 29 January 2007. Translated from the original German by Ethan Taub, M.D. REFERENCES For e-references please refer to the additional references listed below. 1. Robinson DR, Wu YM, Lin SF: The protein tyrosine kinase family of the human genome. Oncogene 2000; 19: 5548–57. 2. Emens LA, Davidson NE: Trastuzumab in breast cancer. Oncology (Williston Park) 2004; 18: 1117–28; discussion 31–2, 37–8. 3. Baselga J, Perez EA, Pienkowski T, Bell R: Adjuvant trastuzumab: a milestone in the treatment of HER-2-positive early breast cancer. Oncologist 2006; 11(Suppl 1): 4–12. 4. Salomon DS, Brandt R, Ciardiello F, Normanno N: Epidermal growth factor-related peptides and their receptors in human malignancies. Crit Rev Oncol Hematol 1995; 19): 183–232. 5. Cunningham D, Humblet Y, Siena S, et al.: Cetuximab monotherapy and cetuximab plus irinotecan in irinotecan-refractory metastatic colorectal cancer. N Engl J Med 2004; 351: 337–45. 6. Poon RT, Fan ST, Wong J: Clinical implications of circulating angiogenic factors in cancer patients. J Clin Oncol 2001; 19: 1207–25. 7. Hurwitz H, Fehrenbacher L, Novotny W, et al.: Bevacizumab plus irinotecan, fluorouracil, and leucovorin for metastatic colorectal cancer. N Engl J Med 2004; 350: 2335–42. 8. Yang JC, Haworth L, Sherry RM, et al.: A randomized trial of bevacizumab, an anti-vascular endothelial growth factor antibody, for metastatic renal cancer. N Engl J Med 2003; 349: 427–34. Dtsch Arztebl 2007; 104(19): A 1312–9 ⏐ www.aerzteblatt.de 8 MEDICINE 9. Sandler AB, Gray R, Brahmer J, et al.: Randomized phase II/III Trial of paclitaxel (P) plus carboplatin (C) with or without bevacizumab (NSC # 704865) in patients with advanced non-squamous non-small cell lung cancer (NSCLC): An Eastern Cooperative Oncology Group (ECOG) Trial - E4599. J Clin Oncol 2005; ASCO Annual Meeting Proceedings Part I. 23(16S): abstract 4. 10. Miller KD: E2100: a phase III trial of paclitaxel versus paclitaxel/bevacizumab for metastatic breast cancer. Clin Breast Cancer 2003; 3: 421–2. 11. Buchdunger E, Cioffi CL, Law N, et al.: Abl protein-tyrosine kinase inhibitor STI571 inhibits in vitro signal transduction mediated by c-kit and platelet-derived growth factor receptors. J Pharmacol Exp Ther 2000; 295: 139–45. 12. O'Brien SG, Guilhot F, Larson RA, et al.: Imatinib compared with interferon and low-dose cytarabine for newly diagnosed chronic-phase chronic myeloid leukemia. N Engl J Med 2003; 348): 994–1004. 13. Shah NP, Sawyers CL: Mechanisms of resistance to STI571 in Philadelphia chromosome-associated leukemias. Oncogene 2003; 22: 7389–95. 14. Talpaz M, Shah NP, Kantarjian H, et al.: Dasatinib in imatinib-resistant Philadelphia chromosome-positive leukemias. N Engl J Med 2006; 354: 2531–41. 15. Corless CL, Fletcher JA, Heinrich MC: Biology of gastrointestinal stromal tumors. J Clin Oncol 2004; 22: 3813–25. 16. Shepherd FA, Rodrigues Pereira J, Ciuleanu T, et al.: Erlotinib in previously treated non-small-cell lung cancer. N Engl J Med 2005; 353: 123–32. 17. Chan SK, Gullick WJ, Hill ME: Mutations of the epidermal growth factor receptor in non-small cell lung cancer – search and destroy. Eur J Cancer 2006; 42: 17–23. 18. Sandler AB: Nondermatologic adverse events associated with anti-EGFR therapy. Oncology (Williston Park) 2006; 20(5 Suppl 2): 35–40. 19. Motzer RJ, Hutson TE, Tomczak P, et al.: Phase III randomized trial of sunitinib malate (SU11248) versus interferon-alfa (IFN-a) as first-line systemic therapy for patients with metastatic renal cell carcinoma (mRCC). J Clin Oncol 2006; ASCO Annual Meeting Proceedings Part I. 24(18S): abstract LBA3. 20. New targeted therapy for rare stomach, kidney cancers. FDA Consum 2006; 40: 5. 21. Escudier B, Szczylik C, Eisen T, et al.: Randomized phase III trial of the Raf kinase and VEGFR inhibitor sorafenib (BAY 43-9006) in patients with advanced renal cell carcinoma (RCC). J Clin Oncol 2005; ASCO Annual Meeting Proceedings Part I. 23(16S): abstract 4510. 22. Herbst RS, Johnson DH, Mininberg E, et al.: Phase I/II trial evaluating the anti-vascular endothelial growth factor monoclonal antibody bevacizumab in combination with the HER-1/epidermal growth factor receptor tyrosine kinase inhibitor erlotinib for patients with recurrent non-small-cell lung cancer. J Clin Oncol 2005; 23: 2544–55. 23. Hainsworth JD, Sosman JA, Spigel DR, Edwards DL, Baughman C, Greco A: Treatment of metastatic renal cell carcinoma with a combination of bevacizumab and erlotinib. J Clin Oncol 2005; 23: 7889–96. 24. Krause DS, Van Etten RA: Tyrosine kinases as targets for cancer therapy. N Engl J Med 2005; 353: 172–87. 25. Arteaga CL, Baselga J: Tyrosine kinase inhibitors: why does the current process of clinical development not apply to them? Cancer Cell 2004; 5: 525–31. ADDITIONAL REFERENCES e1. Borg A, Tandon AK, Sigurdsson H, et al.: HER-2/neu amplification predicts poor survival in node-positive breast cancer. Cancer Res 1990; 50: 4332–7. e2. Bookman MA, Darcy KM, Clarke-Pearson D, Boothby RA, Horowitz IR: Evaluation of monoclonal humanized anti-HER2 antibody, trastuzumab, in patients with recurrent or refractory ovarian or primary peritoneal carcinoma with overexpression of HER2: a phase II trial of the Gynecologic Oncology Group. J Clin Oncol 2003; 21: 283–90. e3. Hirsch FR, Langer CJ: The role of HER2/neu expression and trastuzumab in non-small cell lung cancer. Semin Oncol 2004; 31(1 Suppl 1): 75–82. e4. Ziada A, Barqawi A, Glode LM, et al.: The use of trastuzumab in the treatment of hormone refractory prostate cancer; phase II trial. Prostate 2004; 60: 332–7. e5. Kerkela R, Grazette L, Yacobi R, et al.: Cardiotoxicity of the cancer therapeutic agent imatinib mesylate. Nat Med 2006;12: 908–16. e6. Sun L, Liang C, Shirazian S, et al.: Discovery of 5-[5-fluoro-2-oxo-1,2- dihydroindol-(3Z)-ylidenemethyl]-2,4dimethyl-1H-pyrrole-3-carboxylic acid (2-diethylaminoethyl)amide, a novel tyrosine kinase inhibitor targeting vascular endothelial and platelet-derived growth factor receptor tyrosine kinase. J Med Chem 2003; 46: 1116–9. e7. Wilhelm SM, Carter C, Tang L, et al.: BAY 43-9006 exhibits broad spectrum oral antitumor activity and targets the RAF/MEK/ERK pathway and receptor tyrosine kinases involved in tumor progression and angiogenesis. Cancer Res 2004; 64: 7099-109. Corresponding author PD Dr. med. Carsten Müller-Tidow Medizinische Klinik A – Hämatologie und Onkologie Universitätsklinikum Münster Albert-Schweitzer-Str. 33 48129 Münster, Germany [email protected] Dtsch Arztebl 2007; 104(19): A 1312–9 ⏐ www.aerzteblatt.de 9