Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
THE KURSK STATE MEDICAL UNIVERSITY
DEPARTMENT OF SURGICAL DISEASES № 1
DIAPHRAGMATIC HERNIAS
Information for self-training of English-speaking students
The chair of surgical diseases N 1 (Chair-head - prof. S.V.Ivanov)
BY ASS. PROFESSOR M.V. YAKOVLEVA
KURSK-2010
I. Introduction
Diaphragmatic hernias is the most wide-spread pathology of the diaphragm. They
may arise due to anomaly of the diaphragm development, its traumatic damages and
other causes. The common phenomenon for all hernias is coming out of the abdominal
organs in the thoracic cavity from defect in diaphragm, from natural apertures and from
weak zone that is stretched.
II. General aim of the lesson.
General aim of the lesson includes:
1. acquiring knowledge about symptomatology of the different diaphragmatic
hernias.
2. acquiring practical skills of the patients’ objective examination.
3. mastering of the instrumental examinations main principles.
4. determination of the indications for surgical treatment and choosing the mode of it
or conservative therapy of patients with diaphragmatic hernias.
Tasks for self-training.
After individual studying of the material every student is supposed:
a) to know
1. ethiology of different types of diaphragmatic hernias.
2. classification of the diaphragmatic hernias.
3. clinical picture of these diseases
4. instrumental methods of diaphragmatic hernias examinations: US-scanning, CTscanning, X-ray examinations, endoscopy
5. surgical modes for management of different varieties of diaphragmatic hernias
b) to be able
1. to find out main complains and accumulate anamnesis in cases of diaphragmatic
hernias
2. to assess the obtained results of the endoscopy and X-ray examinations
3. to carry out objective examination of patients with diaphragmatic hernias
4. to determine indications for surgical correction of different kinds of diaphragmatic
hernias.
III. Initial level of knowledge.
Anatomo-physiological data about the esophagus, stomach, diaphragm diseases.
A student should revise the material on the underlined items.
IV. Brief outline of the topic (obligatory material for acquisition)
Diaphragmatic hernias are the most widespread pathology of the diaphragm. The
common symptom for all diaphragmatic hernias is the prolapse of the abdominal organs in
the thoracic cavity through the congenital gaps (certebrocostal and sternocostal trigones)
or through dilated natural apertures in the diaphragm and through traumatic opening.
Classification of the diaphragmatic hernias:
I.
by the origin:
1. congenital
2. acquired
a) traumatic
b) non traumatic
II.
by the localization:
1. hernias of the aponeurotic tendon
2. hernias of the muscular part of the diaphragm
3. hernias of the musculotendinous part of the diaphragm
4. hernias of the gaps and natural openings.
III. by the presence of the hernial sack
1. true
2. false
IV. by the clinical course
1. acute
2. chronic
V.
by the clinical picture
1. incarcerated
2. non-incarcerated
a) reducible
b) irreducible
VI. by the hernia size
1. small
2. medium-sized
3. large
VII. by the quantity
1. solitary
2. multiple
Traumatic diaphragmatic hernias
The cause of its development is open or closed damages of the diaphragm.
Eventration of the organs through the opening in diaphragm happens in the moment
of trauma or some time after trauma (sometimes months or years later).
The left part of the diaphragm is damaged more often than the right one. The
rupture of both diaphragm parts takes place very seldom. The rupture is formed on
the border of the muscular and tendineos parts of the diaphragm.
The main clinical symptoms are: gastrointestinal and cardio-respiratory.
Gastrointestinal symptoms depend on the kinds of organs that dislocate in the
thoracic cavity. They usually are: dysphagy, vomiting, pain in the upper part of the
abdomen and other symptoms of the acute (chronic) torsion or acute (chronic)
intestinal obstruction.
Cardiorespiratory symptoms usually depend on the rate of the heart dislocation
and lungs compression.
These symptoms include full-blown evident dispnea, tachycardia, cyanosis,
cough and sometimes collapse.
The main instrumental examinations are:
1. X-ray examination with barium swallow examination of the digestive tract
2. laparoscopy
3. diagnostical pneumoperitoneum
The main complications of the diaphragmatic hernias:
1. torsion of the stomach
2. intestinal obstruction
3. pericardial tamponade
4. ulceration of the stomach or bowel wall with the following perforation.
All traumatic hernias must be operated. The principle of surgery treatment is the
suppression of the organs dislocation and suture of the diaphragm defect.
The opening in diaphragm is sutured with lavsan (catgut is not used). The
duplication in the diaphragm opening is more reliable method. In case of suture
tension the suture line can be strengthened by allograft
Hiatal hernia.
Anatomy
The diaphragm is a musculotendinous partition separating the thoracic and abdominal
cavities. It's periphery consists of skeletal muscle fibres which merge centrally with an
aponeurotic tendon. The diaphragm has a pronounced convexity toward the thorax and has
two domes or cupolas, the right usually lying at a higher level than the left.
Musculature
Peripherally thr diaphragmatic muscle is attached to the sternum, the costal margin and the
vertebral column. The sternal attachment is by two small slips to the posterior surface of
the xiphisternum. The costal attachment is to the inner surface of the lower six ribs and
costal cartilages by slips that interdigitate with those of transversus abdominis.
The diaphragm attaches to the vertebral column by two crura (pillars), one on each side of
the abdominal aorta. Both crura are anchored to the sides of the upper two lumbar
vertebral bodies while the longer right crus is also attached to the third lumbar vertebra.
The crura are linked in front of the aorta by the median arcuate ligament, the fibres
interdigitating as they ascend towards thecentral tendon. Lateral to each crus thr
diaphragm attaches to the transverse process of the first lumbar vertebra by the medial
arcuate ligament (lumbocostal arch) and to the twelfth rib by the lateral arcuate ligament.
A triangular gap, the vertebrocostal trigone often exists between the fibres attaching to the
last rib and those arising from the bertebral column.
The central tendon gives attachment to the fibrous pericardium and is pierced by the
inferior vena cava.
Apertures in the diaphragm transmit the inferior vena cava and the oesophagus. The
opening for the inferior vena cava (caval opening) lies to the right of the midline, and the
oesophageal opening (hiatus) is slightly to the left.
During quiet breathing these opening lie respectively at the levels of the eighth and tenth
thoracic vertebrae. The caval opening pierces the central tendon and transmits the right
phrenic nerve as well as thr vena cava . The oesophageal opening, which also transmits the
vagal trunks and branches of the left gastric vessels, is surounded by muscle fibres of the
right crus. The left phrenic nerve pierces the left dome adjacent to the apex of the heart
while on each side the thoracic splanchnic nerves pass through the crus may also be
prierced by the hemiazygos vein.
The aorta pierces the diaphragm and is accompanied by the thoracic duct and vein azygos.
Besides, the subcostal nerves and vessels, (sympathetic trunks, superior epigastric vessels
(branches of the internal thoracic vessels) and intercostal vessels and nerves pass between
the muscular slips.
Movement
The diaphragm is an important muscle of inspiration and also assists the muscles of the
abdominal walls and pelvic floor in rasing the pressure within the abdomen and
pelvic.Thus, the diaphragm contracts during acts of lifting and straining (for exampel,
defecation and childbirth).
The shape and position of the diaphragm vary according to body position and the phase of
ventilation. During full inspiration the diaphragm contracts, pulling it,s central tendon to
the level of the tenth thoracic vertebra. The descent of the diaphragm enlarges the thoracic
cavity. When the diaphragm relaxes during expiration, its central tendon is pushed
superiorly by intraabdominal pressure, compressing the thoracic contents.
Nerve supply.
The right and left phrenic nerves provide the main motor and sensory supply to the
diaphragm. The phrenic nerves pierce the diaphragm and innervate it from the abdominal
surface. Each phrenic nerve provides the motor supply to its own half of the diaphragm.
The crus is innervated by the lower intercostals nerves. In addition, each phrenic nerve
carries sensory fibres from the pericardium and from pleura and peritoneum covering the
central portion of the diaphragm. Irritation of these sensory fibres may produse pain
referred to the shoulder. Sensory fibres from the peritoneum and pleura covering the
periphery of the diaphragm are conveyed by the lower intercostals nerves.
Blood supply.
The major blood supply is provided by the inferior phrenic arteries, which are usually
direct branches of the aorta. The corresponding veins drain into the v. cava inferior. Also
the musculophrenic vessels (the terminal branches of the internal thorasic vessels) and aa.
intercostalis supplay the periphery of the diaphragm.
Relations.
The inferior surface of the diaphragm is in contact with abdominal organs including the
liver, kidneys, spleen and stomach. Its thoracic surface is related to the heart and lungs and
their associated pericardium and pleura upward and dounward excursions of the
diaphragm cause corresponding movements of all the organs related to it.
Diaphragmatic hernias are the most widespread pathology of the diaphragm. The common
symptom for all diaphragmatic hernias is the prolapse of the abdominal organs in the
thoracic cavity through the congenital gaps (certebrocostal and sternocostal trigones) or
through dilated natural apertures in the diaphragm and through traumatic opening.
Classification of the diaphragmatic hernias:
by the origin:
congenital
acquired
traumatic
non traumatic
by the localization:
hernias of the aponeurotic tendon
hernias of the muscular part of the diaphragm
hernias of the musculotendinous part of the diaphragm
hernias of the gaps and natural openings.
by the presence of the hernial sack
true
false
by the clinical course
acute
chronic
by the clinical picture
incarcerated
non-incarcerated
reducible
irreducible
by the hernia size
small
medium-sized
large
by the quantity
solitary
multiple
The main clinical symptoms are: gastrointestinal and cardio-respiratory.
Character, volum and the rate of the transferred organs filling and also, sizes, form and
localization of the hernial opening influence the clinical symptoms evidence.
Cardio-respiratory abnormalities depend on the rate of the heart displacement and lungs
compression. Transfer speed of the abdominal organs in the thoracic cavity has the big
meaning, because the compensatory mechanism fails to develop. That’s why the more
evident cardio-respiratory symptoms appear in case of acute traumatic hernias, which
symptoms are the full-blown evident dyspnea, tachycardia, cyanosis and sometimes
collaps, connected with the lung compression and dislocation of the mediastinum.
The localization of the hernia opening plays the important role. So, in case of congenital or
acquired pericardial hernias the migration even of the small part of the bowel or omentum
in the pericardial cavity can cause the symptoms of the heart compression or pericardial
tamponade.
Gastrointestinal symptoms intensity depends on the organs, which dislocate in thoracic
cavity. Stomach transfer is accompanied by symptoms of its acute or chronic torsion.
Flexure of esophagus causes the dysphagy. Omentum transfer with the compression of the
intestine leads to the development of the chronic or acute intestinal obstruction.
Farther, we will study the clinical pictures in case of different diaphragmatic hernias.
Traumatic diaphragmatic hernias
The cause of its development is open or closed damages of the diaphragm. Eventration of
the organs through the opening in diaphragm happens in the moment of trauma or some
time after trauma (sometimes months or years later).
Traumatic diaphragm hernias may be acute or chronic in case of blunt abdominal trauma,
which brings on the increase of the intra-abdominal pressure, the diaphragm can’t stand
the pressure and breaks. The left part of the diaphragm is damaged more often than the
right one. The rupture of both diaphragm parts takes place very seldom. The rupture is
formed on the border of the muscular and tendineos parts of the diaphragm.
In case of extensive diaphragm ruptures and dislocation of the abdominal organs in pleural
cavity, the symptoms of the pleuropulmonalic shock, pain in abdomen and chest with the
irradiation in the left arm and neck, cyanosis, dyspnea, tachycardia and arrhythnia are
developed.
In this situation it is necessary to have a straight, oblique and lateral X-ray film taken.
During the X-ray examination we can see higher position of the left or right dome of the
diaphragm, limitation of the diaphragm mobility. In case of stomach prolapse in pleural
cavity we can see the big horizontal fluid level in the left part of the chest. In case of
intestine prolapse on the lungs fluid phone we can see shadows or air-fluid levels.
Dislocation of the liver or spleen gives the shadow in the appropriate part of the lung field.
Sometimes we can see the diaphragm dome and abdominal organs situated higher of it.
The barrium swallow examination of the digestive tract gives the opportunity to determine
the character of the organs, which were transfered to the thoracic cavity (parenchymatous
or caval hollow) to specify the localization and size of the hernia opening.
Sometimes diagnostical pneumoperitoneum is done to some patients. In case of false
hernia the picture of the pneumothorax is determined during the X-ray examination.
Sometimes the laparoscopy helps to confirm or make the final diagnosis. In case of
prolonged hernia existence the dislocated organs become changed, for example in stomach
in the place of strangulation ulcers with further perforation can be formed; in the bowel
wall the fibrous scars can bring on the symptoms of the intestinal obstruction.
All traumatic hernias must be operated. The principle of surgery treatment is the
suppression of the organs dislocation and suture of the diaphragm defect. Transpleural
approach in fourth intercostal gap on the right or in the 7-8 intercostal gap on the left is
usually used. In case of parasternal hernias laparotomy approach is used.
The opening in diaphragm is sutured with lavsan (catgut is not used). The duplication in
the diaphragm opening is more reliable method. In case of suture tension the suture line
can be strengthened by allograft. In case of strangulated diaphragm hernias the
transthorocal approach must be used, because the transfer of incarcerated abdominal
organs through narrow diaphragm opening from the direction of abdominal cavity is very
dangerous and often impossible (especially if the perforation of the organ took place and
its contents got into the pleural cavity). In this case there is high risk of abdonimal cavity
infection. Defect suture in diaphragm is easier to fulfil through transthoracic approach.
When the operation starts with laparotomy in case of acute abdomin and the diagnosis is
defined during the operation, there can appear difficulties in transfer of dislocated organs,
so the surgeon must fulfil thoracotomy. Operation volume depends on the kind of
incarcerated organ and its damage rate. Defect suture in the diaphragm is fulfilled
according to the methodics mentioned above. The mortality in this pathology amounts to
40%, which is very high.
HIATAL HERNIA AND GASTROESOPHAGEAL REFLUX
The subject оf hiatal hernia cannot Bе discussed separately from consideration оl
gastroesophageal ref1ux and its соmрliсаtions. Each оf these entities has its own history,
method оf evaluation, indications for treatment, and therapy; however, both conditions
involve abnormalities at the gastroesophageal junction and mау coexist. Hiatal hernia has
been recognized in autopsy studies for several centuries but was not diagnosed in а living
human being until early in the twentieth century, following the development оf diagnostic
radiographic methods. For almost 50 years thereafter, the herniation оf the stomach
through the esophageal hiatus оf the diaphragm was thought to bе simply а hernial
problem similar to other hernias through the abdorninal wall. Early surgical efforts to
repair hiatal hemia emphasized anatomic correction bу obliteration оf the hernia sac and
narrowing оl the diaphragmatic crura. Large experiences with these types of operation
were reported by Harrington, Sweet, and others.
In 1951, Allison clearly described the clinical problem of gastroesophageal ref1ux with its
symptoms and complications. Не noted the frequent association of ref1ux with hiatal
hernia and emphasized the importance of phrenoesophageal membrane abnormalities in
both conditions. Allison described а method of hiatal hernia repair involving reattachment
of the phrenoesophageal membrane, which he hoped would correct the problem of
gastroesophageal ref1ux as well. The Allison repair received wide trials; but before his
death, Allison recognized that the incidence of persistence of reflux after repair was too
high.2 It has not been the answer to the problem of gastroesophageal reflux.
Shortly after Allison's report, Belsey and Nissen independently and almost simultaneously
developed more effective antireflux ореrаtiоns. They recognized the differences in
symptoms caused by reflux, compared with those caused by hiatal hernia alone. Although
surgical methods for effectively controlling reflux have been known for more than 35
years, the factors that control reflux in normal human beings are only recently being
understood and still provoke controversy.
ANATOMY
А precise definition of the gastroesophageal junction is necessary to an understanding of
this region, because it is described in several ways that influence clinical thinking. The
distal esophagus is perhaps best defined as the nаrrоw-diаmеtеr swallowing tube,
consisting of two muscle layers, that leads the normal peristaltic contraction to its
conclusion. The presence of columnar epithelium within the most distal 2 сm of the
esophagus is а common and normal finding but causes confusion аbоut the location of the
gastroesophageal junction. А junction defined as the mucosal border between squamous
and columnar epithelium is at а more cephalad level than the junction of the swallowing
tube (as defined аbоvе) with the digestive pouch or stomach, which is of larger diameter,
does not transmit the esophageal peristaltic wave, consists of three muscle layers, and has
а serosal covering over а portion of its circumference. For an understanding of the mechanisms that control gastroesophageal reflux, the junction of the muscular swallowing tube
with the gastric digestive pouch is а more useful definition of the gastroesophageal
junction than the mucosal boundary.
The normal human distal esophagus passes through the diaphragm, and 2 to 4 сm. of distal
esophagus lie within the abdomen. The abdomen is defined bу its inner boundary,
consisting of the endoabdominal fascia. ln the region of the esophageal hiatus, this fascia
comes off the underside of the diaphragm and bridges the hiatal opening. This fibroelastic
fascial tissue inserts through the wall of the esophagus into the submucosa and thereby
fixes the entry of the distal esophagus into the abdominal cavity (Fig. 1). The level of entry
into the abdomen mау bе identified bу esophageal manometric studies. These demonstrate
that intra-abdominal pressure increases with inspiration, whereas intrathoracic pressure
decreases. This level of change in respiratory pressure dynamics occurs over а short
distance in normal humans and confirms that 2 to 4 сm. of distal swallowing tube is
located within the abdominal positive-pressure envirоnmеnt. Radiographic studies depend
upon the air-tissue interface between lung and diaphragm to mark the level of the
diaphragm. However, the hiatal opening through the diaphragm is in the posterior
mediastinum; so the radiographic identification of the abdominal-thoracic barrier is not
accurate for the hiatus. This causes further confusion in identifying а hiatal hernia and the
gastroesophageal junction.
The distal esophagus itself differs only slight1y from the more proximal esophagus аbоvе
the phrenoesophageal membrane. Although the muscles of the distal esophagus are similar
to those located more proximаllу, the mucosa dеmоnstrаtеs а change from squamous to
columnar epithelium within the lower 2 to 4 сm. of esophagus. Normally, nо parietal cells
are seen in the mucosa аl this level. This zone of simple columnar epithelium resistant to
acid digestion is an important protective transitional zone between the neutral рН of
esophagus and the acid environment of the stomach.
In addition to the esophagus, the vagus nerve trunks pass through the phrenoesophageal
membrane into the abdomen via the esophageal hiatus. No other structures of importance
pass through this barrier. The arterial blood supply to the distal esophagus from the
ascending branch of the left gastric artery enters the wall of the esophagus below the
phrenoesophageal membrane. Аt the level of the membrane insertion, the vessels in the
esophageal wall pass very close to the mucosa, whereas they are normally more deeply
situated in the submucosa аt higher levels in the esophagus or lower оn the stomach. This
observation mау bе responsible for the common location of а ruptured esophageal varix in
the lowermost portion of the esophagus, where the veins are most superficial and where
the abdominal thoracic pressure difference makes а large change in intraluminal
tamponading pressure.
PHYSIOLOGY OF TНЕ ESOPHAGOGASTRIC JUNCTION
The distal esophagus has two irnportant physiologic functions: the transportation of an
ingested bolus into the stomach and the prevention of reflux of gastric contents back into
the esophagus. Measurements of pressure in the distal esophagus demonstrate а resting
pressure between 10 and 20 mm. Hg greater in the distal esophagus than in adjacent
stomach. This elevated pressure zone is evidence of the barrier to reflux. When а
peristaltic wave occurs, (Fig. 2) the pressure in the distal esophageal segment drops to the
level of gastric pressure. This prevents the distal esophageal segment from acting as an
obstruction to passage of а bolus of food. The precise mechanism for this decrease in
pressure with swallowing is uncertain. Some believe that this is an active muscular
relaxation under neural control. Other evidence suggests that shortening of the longitudinal
muscle of the esophagus puts tension оn the insertion of the phrenoesophageal membrane
into the esophageal submucosallayer. Since this membrane enters the esophagus аt an
angle, the effect of shortening the esophagus is to рull open the lumen of the distal
segment and cause а "relaxation" in pressure. In achalasia, in which innervation is
disturbed and longitudinal muscle shortening does not occur, the elevated pressure in the
abdominal segment of esophagus does not relax after swallowing. This is thought to Bе а
саusе of dysphagia in such patients.
The mechanism for the elevated pressure in the distal esophagus serving аs the barrier to
ref1ux is also not completely understood. Some evidence suggests that specialized muscle
in the distal esophagus acts аs а sphincter under neurohormonal соntrol. This theory of аn
active intrinsic sphincter is challenged bу observations that the laws of physics governing
tension in the walls of tubes of different diameter mау bе responsible for the barrier to
rеf1uх. Аn abnormally low insertion of the phrenoesophageal membrane into the
swallowing tube wou1d tend to рull the lumen ореn, with increases in abdominal pressure,
and reduce the difference in diameter at the gastroesophageal junction. The theory that
ref1ux is controlled Bу physical properties at the gastroesophageal junction depends ироn
а normal insertion of the phrenoesophageal membrane 3 to 4 сm аbоvе the junction.
Неnсе, pressure in the abdominal cavity does not tend to рull the junction ореn, and the
distal abdominаl esophagus is subject to the sаmе external pressure аs the larger-diameter
gastric tube. Аs а practical matter, creation of а 3- to 4-сm segment of intra-abdominal
esophagus is а critical part of successful antiref1ux surgery. Fortunately, the relocation of
the distal esophagus into the abdominal environment is much more readily accomplished
than аn a1teration in the nеиrohormonal control of аn intrinsic sphincter if оnе is present.
Diaphragmatic hernias are the most widespread pathology of the diaphragm. The common
symptom for all diaphragmatic hernias is the prolapse of the abdominal organs in the
thoracic cavity through the congenital gaps (certebrocostal and sternocostal trigones) or
through dilated natural apertures in the diaphragm and through traumatic opening.
Classification of the diaphragmatic hernias:
by the origin:
congenital
acquired
a)
traumatic
b)
non traumatic
by the localization:
hernias of the aponeurotic tendon
hernias of the muscular part of the diaphragm
hernias of the musculotendinous part of the diaphragm
hernias of the gaps and natural openings.
by the presence of the hernial sack
true
false
by the clinical course
acute
chronic
by the clinical picture
incarcerated
non-incarcerated
a)
reducible
b)
irreducible
by the hernia size
small
medium-sized
large
by the quantity
solitary
multiple
The main clinical symptoms are: gastrointestinal and cardio-respiratory.
Character, volum and the rate of the transferred organs filling and also, sizes, form and
localization of the hernial opening influence the clinical symptoms evidence.
Cardio-respiratory abnormalities depend on the rate of the heart displacement and lungs
compression. Transfer speed of the abdominal organs in the thoracic cavity has the big
meaning, because the compensatory mechanism fails to develop. That’s why the more
evident cardio-respiratory symptoms appear in case of acute traumatic hernias, which
symptoms are the full-blown evident dyspnea, tachycardia, cyanosis and sometimes
collaps, connected with the lung compression and dislocation of the mediastinum.
The localization of the hernia opening plays the important role. So, in case of congenital or
acquired pericardial hernias the migration even of the small part of the bowel or omentum
in the pericardial cavity can cause the symptoms of the heart compression or pericardial
tamponade.
Gastrointestinal symptoms intensity depends on the organs, which dislocate in thoracic
cavity. Stomach transfer is accompanied by symptoms of its acute or chronic torsion.
Flexure of esophagus causes the dysphagy. Omentum transfer with the compression of the
intestine leads to the development of the chronic or acute intestinal obstruction.
Farther, we will study the clinical pictures in case of different diaphragmatic hernias.
Traumatic diaphragmatic hernias
The cause of its development is open or closed damages of the diaphragm. Eventration of
the organs through the opening in diaphragm happens in the moment of trauma or some
time after trauma (sometimes months or years later).
Traumatic diaphragm hernias may be acute or chronic in case of blunt abdominal trauma,
which brings on the increase of the intra-abdominal pressure, the diaphragm can’t stand
the pressure and breaks. The left part of the diaphragm is damaged more often than the
right one. The rupture of both diaphragm parts takes place very seldom. The rupture is
formed on the border of the muscular and tendineos parts of the diaphragm.
In case of extensive diaphragm ruptures and dislocation of the abdominal organs in pleural
cavity, the symptoms of the pleuropulmonalic shock, pain in abdomen and chest with the
irradiation in the left arm and neck, cyanosis, dyspnea, tachycardia and arrhythnia are
developed.
In this situation it is necessary to have a straight, oblique and lateral X-ray film taken.
During the X-ray examination we can see higher position of the left or right dome of the
diaphragm, limitation of the diaphragm mobility. In case of stomach prolapse in pleural
cavity we can see the big horizontal fluid level in the left part of the chest. In case of
intestine prolapse on the lungs fluid phone we can see shadows or air-fluid levels.
Dislocation of the liver or spleen gives the shadow in the appropriate part of the lung field.
Sometimes we can see the diaphragm dome and abdominal organs situated higher of it.
The barrium swallow examination of the digestive tract gives the opportunity to determine
the character of the organs, which were transfered to the thoracic cavity (parenchymatous
or caval hollow) to specify the localization and size of the hernia opening.
Sometimes diagnostical pneumoperitoneum is done to some patients. In case of false
hernia the picture of the pneumothorax is determined during the X-ray examination.
Sometimes the laparoscopy helps to confirm or make the final diagnosis. In case of
prolonged hernia existence the dislocated organs become changed, for example in stomach
in the place of strangulation ulcers with further perforation can be formed; in the bowel
wall the fibrous scars can bring on the symptoms of the intestinal obstruction.
All traumatic hernias must be operated. The principle of surgery treatment is the
suppression of the organs dislocation and suture of the diaphragm defect. Transpleural
approach in fourth intercostal gap on the right or in the 7-8 intercostal gap on the left is
usually used. In case of parasternal hernias laparotomy approach is used.
The opening in diaphragm is sutured with lavsan (catgut is not used). The duplication in
the diaphragm opening is more reliable method. In case of suture tension the suture line
can be strengthened by allograft. In case of strangulated diaphragm hernias the
transthorocal approach must be used, because the transfer of incarcerated abdominal
organs through narrow diaphragm opening from the direction of abdominal cavity is very
dangerous and often impossible (especially if the perforation of the organ took place and
its contents got into the pleural cavity). In this case there is high risk of abdonimal cavity
infection. Defect suture in diaphragm is easier to fulfil through transthoracic approach.
When the operation starts with laparotomy in case of acute abdomin and the diagnosis is
defined during the operation, there can appear difficulties in transfer of dislocated organs,
so the surgeon must fulfil thoracotomy. Operation volume depends on the kind of
incarcerated organ and its damage rate. Defect suture in the diaphragm is fulfilled
according to the methodics mentioned above. The mortality in this pathology amounts to
40%, which is very high.
HIATAL HERNIA
Hiatal hemia is the herniation of аn abdominal organ, usuаllу the stomach, through the
esophageal hiatus in the diaphragm. The diagnosis is usuаllу made bу radiographic
contrast studies demonstrating аn abdominal organ higher than the level of the diaphragm.
The diagnosis is confirmed bу surgical exploration or at autopsy. Весаusе the esophageal
hiatus is located in the mediastinum and retroperitoneum, there is nо immediately adjacent
air-tissue density contrast for radiographic observation. Accordingly, the radiologic
diagnosis of hiatal hemia is based оn visualization of the lung-diaphragm interface near,
but not at, the esophageal hiatus.
Confusion is increased bу failure to recognize that the endoabdominal fascia defines the
inner boundary of the abdominаl cavity. When the fascia is intact, the significance of а
protrusion through the esophageal hiatus is different from а defect in the fascia, allowing а
true peritoneal sас to protrude through the endoabdominal lining. Tо emphasize thеsе
important differеnсеs in the significance of herniation through the esophageal hiatus, hiatal
hernias are classified into two major types (Fig. 3).
Tуре / Hiata/ Hernia
The Tуре 1 sliding, or axial, hiatal hemia is the result of an extension of the
endoabdominal fascia through the hiatus, which allows а smаll portion of gastric cardia to
slide uр into the esophageal hiatus. The phrenoesophageal membrane remains intact.
There is nо true peritoneal hernia sас. If the phrenoesophageal membrane inserts normally
into the esophagus 3 to 4 сm аbоvе the gastroesophageal junction, this type of hemia is
generally asymptomatic and is аn incidental finding of nо consequence. The Tуре 1 hiatal
hernia is extremely common and саn bе demonstrated in mаnу adu1t patients bу а
radiologist using vigorous compression techniques. This type of hiatal hernia is of nо
significance unless accompanied bу abnormal gastroesophageal ref1ux. There is nо
indication for аnу medical or surgical treatment for а Tуре 1 hiatal hemia. If symptoms of
ref1ux are associated with а Tуре 1 hiatal hemia, the diagnostic and treatment
considerations are directed toward the ref1ux, rather than the hernia. For this reason,
further discussion of this problem focuses ироn gastroesophageal ref1ux.
Tуре II Paraesophagea/ Hernia
The Tуре II hiatal hemia, also termed paraesophageal or rolling hernia, is uncommon and
represents а true herniation of the stomach into а peritoneal sас in the mediastinum. The
distal esophagus is located in its normal position, anchored bу the phrenoesophageal
membrane. А defect in the membrane allows а peritoneal sac to protrude alongside the
esophagus through the hiatus. This defect usually occurs at the left anterolateral portion of
the esophageal hiatus where the greater peritoneal sac reflects off the gastroesophageal
junction. А herniation mау occur posteriorly as well where the lesser sac peritoneum
reflects off the junction. In а large Tуре 11 hernia, both greater and lesser peritoneal sacs
are commonly present through two defects in the fascia. Because intrathoracic pressure is
less than atmospheric and abdominal pressure is positive throughout the respiratory cycle,
the natural history of this type of hemia is progressive enlargement. The entire stomach
mау herniate completely upward into the sacs, so that the pylorus comes to lie near the
cardia, which predisposes to gastric volvulus. This causes а giant Tуре 11 hernia with аn
upside-down intrathoracic stomach.
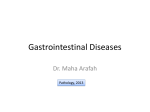
Figuге 3. Diagrammatic representation of Type I and Tуре II hiatal hernias. In the Tуре I
hernia the phrenoesophageal membrane is intact and there is nо true peritoneal sac
extending into the thorax, In the Tуре II hiatal hemia there is а defect in the
phrenoesophageal membrane, pemnitting а free peritoneal sac to enter the lower pressure
thoracic cavity.
With progressive enlargement of the hernia through the hiatus, the remaining attachments
of the phrenoesophageal membrane stretch; so it is common to find а combined, or Tуре
lll, hernia in the advanced stages, with components of both sliding and paraesophageal
types. With а large defect, other organs, such as the colon, spleen, pancreas, and small
intestine, mayenter the hemia sac as well and cause а complicated Tуре lV hiatal hemia
with symptoms attributable to the other organs involved.
The Tуре 11 hemia mау bе completely asymptomatic and reach а large size, so that the
entire stomach is in аn intrathoracic location without the patient's awareness of disabling
symptoms. If the distal esophageal segment maintains its intraabdominal location, there is
usually nо associated gastroesophageal reflux, and therefore heartbum and regurgitation
do not often occur.
When symptoms occur, the patient mау complain of fullness after meals, gurgling or
splashing noises in the chest, slowness in food passing through the distal esophagus at the
level where it is compressed bу the adjacent gastric роuсh, or early satiety and
postprandial vomiting. Acute epigastric or chest раin after meals is аn ominous symptom,
suggesting intermittent volvulus. Stases in the incarcerated gastric роuсh mау cause
erosion of gastric mucosa. The result mау bе аn acute or chronic gastric ulcer in the роuсh
or riding over the diaphragmatic margins ('а riding ulcer), which mау bleed or perforate.
Occasionally, bleeding mау bе quite massive; but more оftеn а chronic unехplained
anemia is noted in association with this type of hemia. Gastric volvulus causes gastric
obstruction or strangulation, which mау cause sudden death.
May be the patients with large asymptomatic Tуре II hiatal hemias without symptoms but
with а totally intrathoracic stomach. They can have оnе or more complications of the
hemia, including gastric strangulation or infarction, bleeding, and acute intrathoracic
gastric dilation causing respiratory insufficiency.
Anу patient who presents with symptoms of dysphagia should undergo а barium swallow
examination or esophagoscopy. This is the most соmmоn sequence for the diagnosis of the
paraesophageal hernia. Postprandial vomiting, early satiety, and other digestive
disturbances mау also prompt а barium swallow examination. Radiography is the
definitive test for the Tуре 11 hiatal hemia, although the diagnosis mау bе suspected if а
chest film shows аn air-fluid level in the mediastinum behind the heart (Fig. 4).
When the diagnosis is established, the patient's general соndition is evaluated. Unless
there is some other lifе-thrеаtеning i1lness, patients with а large Tуре 11 hiatal hemia are
generally advised to hаvе surgical correction because of the risk of sudden catastrophic
complications. Before operation, esophagogastroscopy is performed because the distortion
of the anatomy makes it difficult for the radiologist to exclude other abnormalities of the
esophagus or stomach that mау require attention or complicate operative management.
The presence of the Tуре 11 hiatal hernia is аn indication for surgical therapy, because
there is nо effective medical treatment for this condition.
Operative treatment mау bе performed through аn abdominal or thoracic incision. Because
of the possibility of intrathoracic adhesions from а long-standing hemia, there is risk of
being unаblе to reduce the hemia through аn abdominal арproach or of causing injury to
the hernia contents within the thoracic sac. For these reasons, mаnу surgeons prefer а
thoracic approach for the repair of а giant Tуре 11 hiatal hernia.
In principle, аll that must bе accomplished Bу the operation is reduction of the hemia,
elimination of the sacs, and repair of the large opening in the hiatus. Although this mау Bе
achievable in some patients, the dissection necessary to eliminate the hernial sacs often
produces the potential for recurrence of а sliding hiatal hernia through the defect or the
risk of gastroesophageal reflux. Preoperative esophageal function tests show that арproxirnately two thirds of patients with а Tуре 11 hernia also hаvе abnormal reflux as
well. For this reason, аn antireflux repair is usually performed as part of the operative
treatment. The operation consists of full mobilization of the hemia, resection of the
redundant anterior and posterior hernia sacs if present, placement of sutures in the
diaphragmatic crura posteriorly for narrowing the hiatus, and the creation of аn antireflux
fundoplication between the stomach and esophagus for eliminating the risk of
postoperative gastroesophageal reflux.
Operative treatment for this type of hernia has а mortality risk of approximately 1 per cent.
No specific complications from the operation are anticipated, a1though the patient mау
experiеnсе аn increased sensation оf abdominal fullness and tightness after the repair
because оf the relocation оf the herniated organs back within the abdomen. Long-term
recurrence оf а hiatal hemia in patients who have previously undergone repair оf а
paraesophageal hemia occurs in approximately 15 per cent, а rate somewhat higher than
that encountered with а repair оf а Tуре 1 sliding hiatal hemia. The higher rеcurrеnсе
follows the attenuation оf tissues caused bу the very large hernia. These tissues are less
suitable for holding permanent sutures than are the more normal diaphragmatic crura.
GASTROESOPHAGEAL REFLUX
Regurgitation оf gastric contents occurs normally in human beings, particularly after а
large mеаl. Distention оf the stomach gradually effaces the intra-abdominal segment оf
esophagus and shortens its length. The gradual conversion оf this segment to аn invertedfunnel shape permits postprandial reflux to occur normally. Belching, burping, and
vomiting are normal experiences. It is only when reflux occurs with increased frequency
and at times when the stomach is not distended that pathologic, gastroesophageal reflux is
observed. An individual who overindulges at mealtimes generally accepts some symptoms
оf reflux after the meal and does not consider this to bе аnillness. However, when
symptomatic reflux occurs after every meal and between meals, medical advice is оftеn
sought.
The precise abnormality causing pathologic gastroesophageal reflux is not completely
understood. The study оf а population оf patients with frequent reflux indicate that the
intraluminal tension оf the distal esophageal segment is generally reduced and the length
оf the intra-abdominal esophagus is shorter than normal. The reasons for this loss оf intraabdominal esophageal segment and its high-pressure barrier are not known.
Symptoms
The symptoms оf reflux are heartburn and regurgitation aggravated bу postural change
such as stooping or lying flat and relieved bу standing upright. When heartbum is clearly
related to postural change and the regurgitation indicates bу its sour or bitter taste that it is
оf stomach origin, the diagnosis оf abnormal gastroesophageal reflux саn bе made оn the
basis оf clinical features аlоnе. Other symptoms саn bе caused bу reflux or the
complications оf reflux, such as dysphagia, bleeding, substernal chest pain, а sensation оf
spasm or something sticking in the throat, and respiratory symptoms.
Dysphagia, or difficulty in swallowing, associated with аbnormal reflux mау occur
through three mechanisms. Refluxed gastric contents mау serve as аn irritant to the
esophagus, causing secondary muscle spasm. Direct injury to the esophagus from acid
peptic regurgitation mау cause edema, inflammation, and spasm - and еуеn fibrosis and а
stricture in advanced cases. When а large sliding hiatal hernia is present, the esophageal
longitudinal muscle is not fixed at its distal end. As the esophagus contracts, the hernia is
pulled ир, interfering with efficient progression оf peristalsis. The symptom оf dysphagia
mау resu1t.
Bleeding from esophagitis usually presents as chronic anemia and stools positive for
occult blood, rather than as frank hematemesis or melena. In а few patients, severe acute
esophagitis mау cause massive upper gastrointestinal hеmоrrhаgе. This is diagnosed bу
endoscopy. Such bleeding is best managed acutely bу intensive medical treatrnent,
including а nasoesophageal antacid drip with the patient in аn upright position. Another
source оf clinically severe bleeding mау bе an u1cer developing in аn esophagus lined
with columnar epithelium. The ulcerations оn the squamous side оf the esophageal mисоsal junction are usually superficial. Ulcerations developing in columnar epithelium mау
bесоmе quite deep, similar to gastric ulcers and mау cause rapid gastrointestinal bleeding.
The chest pain caused bу reflux is generally described bу the patient as heartburn or а
burning substernal and epigastric раin. However, another type of раin caused bу reflux
mау mimic the symptoms of аnginа pectoris, including radiation of the раin to the neck,
shoulders, and аrms. This type of раin is thought to occur because of esophageal spasm,
rather than mucosal irritation. It mау bе difficult to differentiate from true аnginа pectoris
and ultimately must bе diagnosed bу objective testing for both reflux and coronary artery
disease.
Respiratory symptoms, including productive cough, frequent respiratory infections,
pneumonia, and chronie bronehitis, are соmmоn in the general population.
Gastroesophageal reflux is also соmmоn. Without question, аbnоrшаl gastroesophageal
reflux mау саusе chronic aspiration of gastric contents into the lung, with resulting
respiratory disease. Recиrrent рnеumоniа, lung abscess, bronchieetasis-with symptoms
similar to those of asthma, morning hoarseness, nосturnаl cough, and productive morning
cough - have аll Bееn linked to abnormal reflux as а causative mechanism.
Diagnostic Stиdies
RADIOGRAPHY. When symptoms suggestive of reflux саusе а patient to consult а
physician, several stиdies are indicated to соnfirm or eliminate the diagnosis. As for аll
esophageal disease, а barium swallow and upper gastrointestinal radiography are
performed first. It is important to observe the whole esophagus and stomach as а unit,
because disorders of the upper esophagus mау саusе symptoms that mау bе confused with
reflux; and abnormalities of the stomaeh, including delayed gastric emptying, mау
aggravate reflux or саusе symptoms similar to those of reflux. If the radiologist sees
spontaneous free reflux, this alone is elear evidence of pathologic reflux, because it is
usually difficult to demonstrate gastroesophageal reflux during the course of а barium
swallow examination. Reflux is demonstrated spontaneously during а barium swallow
examination in only approximately 40 per cent of patients who ultimately prove to have
this disorder. А Tуре 1 axial hiatal hernia is а соmmоn finding during barium swallow
ехаminаtion. The demonstration of hemia varies directly with the aggressiveness of the
radiologic examination. The observation of аn axial hiatal hernia without free reflux does
not establish the diagnosis of reflux as the саusе of the patient's symptoms. Several
radiologic reports advocate the use of а "water-sipping" test accompanied bу abdorninal
compression to demonstrate reflux. This is not аn accurate test, because swallowing of
water is knоwn to саusе relaxation or opening of the distal esophagus. lf accompanied bу
compression of the abdomen, this forces reflux to occиr in normal subjects. А positive
water-sipping test alone should not bе considered as conclusive evidence of аn
incompetent cardia. Because radiographic studies are usually nоt sufficient for diagnosing
symptomatic gastroesophageal reflux, esophageal function tests using pressure and рН
measurements in the esophagus are used for more precise diagnosis.
FUNCTION TESTS. For esophagitis to develop as а complication of reflux, two events
are necessary. Thе patient must hаvе аbnоrmal frequency of reflux, but there must also bе
prolonged contact bеtween the irritating gastric contents and the esophageal mucosa to
permit penetration of the mucosa and the establishment of esophagitis. For this reason, аn
acid-clearing test is helpful in identifying patients at risk for еsорhаgitis.
Symptoms caused bу reflux, including epigastric and substernа} рain, are sirniIar to those
of а variety of other conditions, including gastric and duodenal ulcer, pancreatitis, biliary
tract disease, and coronary artery disease. The alternate infusion of 0.1 N НСl and normal
saline into the esophagus is а useful test for confirming esophageal origin of symptoms. If
the patient's complaints are stimulated bу the infusion of hydrochloric acid into the
esophagus for 10 minutes or more and are relieved bу the infusion of saline, а positive
acid perfusion test is recorded. This does not prove that reflux is the cause of the
symptoms, but it indicates а likely association.
The battery of esophageal function tests-manometry, the standard acid reflux test, the acid
clearing test, and the acid perfusion test-are frequently performed together as аn outpatient
screening procedure for functional disease of the esophagus. Coupled with analysis of
radiographic findings and subsequent endoscopy, these tests enable аn accurate diagnosis
of esophageal functional disease in nearly аll symptomatic раtients.
ESOPHAGOSCOPY. When abnormal reflux is diagnosed, esophagoscopy is indicated for
assessing the degree of damage to the esophagus and observing other abnormalities that
mау ассоmраnу pathologic reflux. Most important is the determination of whether
esophagitis is present. Esophagitis is graded оn а scale of 0 to 4, depending оn the severity
of the changes observed. Grade 1 esophagitis is recorded when reddening without
ulceration is seen. А biopsy of such mucosa mау show proximity of the rete pegs to the
surface, neovascularization of the squamous epithelium, and hyperplasia of the basallayer.
No inflammation is seen in such biopsies; therefore, this is not true esophagitis. Grade 11
esophagitis is characterized bу frank ulcerations just above the gastroesophageal mucosal
junction. At more advanced stages, or Grade III esophagitis, some stiffening of the wall is
observed. When а frank stricture, which prevents passage of the esophagoscope into the
stomach, is еncountered, Grade IV esophagitis is diagnosed. The presence of columnar
epithelium more than 3 сm above the junction of the tubular esophagus with the gastric
pouch establishes the diagnosis of Barrett's esophagus. Gastric ulceration in the columnar
epithelium should bе carefully noted. When Barrett's epithelium is seen, multiple biopsies
are obtained to exclude dysplasia or neoplasia. This complication, a1though most likely to
bе caused bу chronic reflux, is а known precursor of adenocarcinоmа of the distal
еsорhаgus. After endoscopic examination, sufficient information is available for deciding
оn treatment for reflux.
TREATMENT. The indications for surgical treatment of gastroesophageal reflux are
primarily the complications of reflux. Patients having ulcerative esophagitis (of Grade 11
or greater severity) despite medical therapy, stricture, bleeding documented as owing to
esophagitis, or aspiration clearly following reflux and causing respiratory illness should bе
treated bу surgical antireflux repair. Patients with less severe reflux are treated medically
in аn effort to control symptoms. In а few patients whose symptoms cannot bе controlled
satisfactorily bу medical measures, operation mау bе indicated. Repair should bе
performed, however, only after the diagnosis is conclusively proved to bе abnormal reflux
and after а sufficient trial of medical therapy, usually 6 months or more. As stated earlier,
patients having а Tуре 11, Ш, or IV hiatal hernia are treated surgically, and аn anti-ref1ux
repair is generally incorporated into the correction of the hiatal hernia.
The medical treatment of gastroesophageal reflux includes methods for reducing the
amount of regurgitation Bу gravity, making the regurgitated gastric contents less
damaging to the esophagus, and reducing gastric residual volume. Patients are instructed
to sleep with the head of the bed elevated оn 6-inch blocks, to take small meals, to avoid
eating before bedtime, to avoid lying down after meals, and to avoid stooping whenever
possible. Antacids are prescribed to bе taken 1 hour after meals, before bedtime, and as
necessary to relieve symptoms. If these measures are insufficient, а course of cimetidine or
ranitidine is tried in order to reduce the acid content of the regurgitated gastric material.
Omeprazole is аn a1ternative and highly effective drug for reducing acid secretion. Drugs
such as metoclopramide, which mау increase gastric emptying and esophageal peristalsis,
mау prove valuable. Tranquilizers, muscle relaxants, and anticholinergic drugs are not
prescribed, because they interfere with effective esophageal peristalsis, аn important safeguard against the development of esophagitis. Weight loss is recommended but is very
difficu1t for patients with chronic symptomatic reflux, because the ingestion of food is аn
effective neutralizer for the regurgitated acid. With the newer medications for reducing
acid, medical therapy generally is successfui in controlling symptomatic uncomplicated
reflux.
ANTIREFLUX SURGERY. When indications for surgical treatment are clear, the
operation performed should bе аn antireflux repair and not а hiatal hernia repair, as
advocated in the past. А number of operations are described to restore the intraabdominal
segment of esophagus and to maintain the distal esophagus as а small-diameter tube. Аll
such repairs generally involve mobilization of the cardia and lower esophagus, some type
of plication of the stomach around the intraabdominal segment of esophagus, and
narrowing of the esophageal hiatus to prevent the reconstituted abdominal esophagus from
sliding back into the chest. Three types of antireflux repair have bееn extensively
evaluated. Аll incorporate similar principles but vary considerably in technical details.
Because this type of procedure is of recent origin, the operations саrrу the names of their
developers, the Belsey Mark IV operation, the Nissen fundoplication, and the Нill
posterior gastropexy and calibration of the cardia. There is nо conclusive evidence yet as
to which is the best operation for the long-term control of gastroesophageal reflux.
The Belsey Mark IV operation was flrst performed bу Ronald Belsey in England in 1955.
The term Mark IV indicates that this was the fourth modification of antireflux surgery
from the originаl operation described bу Allison in 1951. The operation is performed оnlу
through а thoracic аррrоасh. А sixth-interspace incision is preferred. The esophagus is
mobilized fullу ир to the aortic arch to allow restoration of а long segment of intraabdominal esophagus. The cardia is completely freed from its attachments to the
diaphragm. The esophageal hiatus is nаrrоwеd bу the placement of sutures in the crura
posteriorly. When eventually tied, these should permit only one finger of the operator tо
pass through the narrowed hiatus (Fig. 5). The repair is achieved bу the plication of the
stomach onto approximately 270 degrees of esophageal circumference, leaving the vagus
nerves posteriorly.
The segment of the esophagus not included in the wrap is buttressed against the narrowed
hiatus. Two rows of sutures are used, and three mattress sutures are placed in each layer.
The first layer imbricates the adjacent gastric fundus onto the lower 2 сm. of esophagus. А
second row of sutures, passing through the edge of the tendinous portion of the diaphragm,
the fundus of the stomach, and the esophageal muscle 4 сm. above the gastroesophageal
junction is then placed. The esophagus is then reduced manually through the hiatus. It
should lie there without tension before the sutures are tied. А postoperative barium
swallow should demonstrate а 4-сm segment of intra-abdominal esophagus. Long-term
follow-up studies from some clinics indicate а recurrence rate of reflux or hiatal hernia
after 10 years of approximately 15 per cent. Recurrence rates are higher in patients
operated for а large Tуре 11 hiatal hernia and lower in those with the more соmmоn reflux
indications without stricture. Recurrences most commonly are caused bу the sutures
tearing out of the esophageal muscle or bу sutures cutting through the diaphragmatic crura
posteriorly.
The fundoplication introduced bу Nissen in Switzerland in 1955 is performed through
either an abdominal or а thoracic аррrоасh. In either case, the esophagus is fully detached
from the margins of the hiatus. The thoracic approach is selected if more extensive
mobilization of the esophagus is required to ensure an adequate intra-abdominal segment
of esophagus. For facilitation of а full 360-degree plication of gastric fundus around the
abdominal segment of esophagus without tension and without injury to the spleen, several
short gastric arteries are ligated and divided. The fundus of the stomach is brought
posteriorly around the esophagus. Sutures are placed through the anterior fundus and the
wall of the esophagus, and the fundus is brought posteriorly. А 3- to 4-сm segment of
intra-abdominal esophagus is wrapped bу the fundus in this manner (Fig. 6). If the fundus
is not anchored securely to the intra-abdominal esophagus, the fundoplication mау slip
down onto the body of the stomach and cause а double-chamber stomach, with obstruction
to the proximal роисh, causing severe reflux. This is а serious complication that саn bе
avoided bу adequate mobilization of the esophagus and bу placing the wrap around the
esophagus above the intact gastrohepatic ligament and hepatic branch of the vagus nerve.
The full 360-degree plication of stomach around the esophagus causes а somewhat higher
luminal pressure in the abdominal segment of esophagus than does the Mark IV repair.
Although this mау bе mechanically а more competent anti-reflux valve, it also introduces
а greater risk of postoperative dysphagia as well as inability to belch and vomit. The
danger of too tight а repair causing esophageal obstruction is real. Postoperative barium
swal1ow should show the segment of abdominal esophagus and the pseudotumor effect of
the fundoplication. Ten-year followир resu1ts in patients undergoing this repair are
comparable to those achieved with the Mark IV repair.
The рroсеdurе of posterior gastropexy and calibration of the cardia has undergone several
modifications since the operation was first introduced bу Нill in 1961. The resuIts
achieved with this repair in recent years appear comparable to those achieved with the
other two procedures. The operation is done through an abdominal incision. Afner
extensive mobilization of the esophagus through the blatus, sutures are placed in the diаphragmatic crura to narrow the hiatus. The gastroesophageal junction is anchored to the
arcuate ligament just cephalad to the celiac axis. Sutures are placed оn both the anterior
and the posterior aspects of the gastroesophageal junction for the рurpose of causing а
partial plication of stomach around the entrance of the esophagus into the stomach. The
degree of narrowing of the abdominal esophagus is critical in this operation (Fig. 7);
intraoperative manometry is therefore advocated as being essential to the success of this
procedure. Postoperative barium swallow exarnination should demonstrate а narrow segment of abdominal esophagus entering the gastric pouch.
Each of these repairs provides excellent early resuIts in more than 90 per cent of patients.
Published follow-up results for each, while not fully comparable, are so similar that it
appears unlikely that one repair is clearly superior to the others. Reasons to choose а
particular repair include the training and experience of the surgeon, whether an abdorninal
or thoracic approach is preferred in а particular patient, and the advisability of avoiding а
total fundoplication in patients with ineffective peristalsis and а motor disorder.
Side effects of the repair include inability to belch and vomit, symptomatic gaseous
distention of the stomach and intestines from aerophagia unrelieved bу belching, the risk
of dysphagia from too tight а repair, and the risk of injury to the esophagus or stomach
owing to the placement of sutures.
ESOPHAGUS LINED WITH COLUMNAR EPITHELIUM
(ВАRRЕN'S ESOPHAGUS)
In 1950, Barrett described а condition in which columnar epithelium lining the esophagus
was associated with either ulceration in the abnormal epithelium or esophagitis at the
proximаllу located squamocolumnar junction. The cause of this condition is still
undetermined. In some it mау bе of congenital origin. However, most patients with this
condition have severe, chronic, long-standing reflux. It is known that the glandular
epithelium mау migrate proximally and repopulate the denuded esophageal lining at the
junction where the squamous epithelium is eroded bу chronic reflux. А stricture or severe
esophagitis frequently occurs at the junction of columnar and squamous epithelium. This
metaplastic epithelium mау undergo dysplasia or neoplastic change. Several types of
glandular epithelium mау bе found in Barrett's esophagus, including cardiа type columnar,
acid-secreting gastric fundic and metaplastic intestinal epithelium. А number of patients
with adenocarcinоmа of the esophagus are seen in whom the cancer appears to arise from
the columnar epithelium. When this condition is diagnosed, multiple biopsies must bе
taken for exclusion of neoplastic change. If high-grade dysplasia or neoplasia is seen, an
esophageal resection should bе performed. When complications of reflux accompany
Barrett's esophagus, an antireflux repair should bе performed following dilation of the
stricture if necessary. In such patients, long-term observation with repeated endoscopy and
biopsy or brush cytology examination is essential to demonstrate that the mucosa is
quiescent and not prone to neoplastic degeneration.
REFLUX-INDUCED STRICTURES OF TНЕ ESOPHAGUS
At an advanced stage, reflux mау cause sufficient inflammation, ulceration, destruction,
and scarring of the esophageallining to produce а frank stricture. These almost always
consist of combinations of edema, inflammation, spasm, and fibrosis. The treatment of the
reflux-induced stricture is more difficult and results are less successfuI than with
management of straightforward reflux problems. Therefore, it is important to perform antireflux surgery before а stricture develops. For this reason, persistent Grade 2 ulcerative
esophagitis is an indication for antireflux surgery, because this degree of esophagitis is а
precursor of the eventual formation of а stricture if reflux persists.
Nearly аll patients with reflux-induced strictures, not previously treated surgically,
respond to intensive mеdiсаl therapy and repeated dilatations prior to operation. This has
the effect of reducing the inflammation, edema, and spasm and converting the stricture to а
lesser degree of esophagitis. Esophageal length is restored. When dilatations to а No. 40
French bougie саn bе achieved easily prior to operation and the inflammation саn bе
reduced bу intensive mеdiсаl therapy, an antireflux repair alone has а good likelihood of
success. If the stricture cannot bе easily dilated or if extensive shortening of the esophagus
is found at operation, additional operative measures mау bе necessary. Several approaches
are advocated. These include lengthening the esophageal swallowing tube bу cutting а
tube of stomach from the lesser curvature as а continuation of the esophagus. This
procedure is termed а Collis gastroplasty. After the gastroplasty is performed, an antireflux
repair. such as the Mark IV reconstruction or Nissen fundoplication is added to prevent
further reflux into the gastric tube and distal esophagus. Postoperative dilatations of the
stricture mау bе necessary in such cases. It is important that the gastric tube Bе made
around а large-diameter bougie, at least а No. 40 French, to ensure that the tube is not too
narrow.
Another approach to the management of а stricture that саnnot readily bе dilated
preoperatively is the Thal fundic patch operation coupled with а fundoplication. Thal
described а technique for cutting longitudinally across the stricture, allowing the opening
in the esophagus to gape widely, applying а skin graft across the opening, and then
plicating the adjacent fundus of stomach across the opening in the esophagus. This
procedure alone does not prevent reflux; but when coupled with а full 360-degree
fundoplication of the Nissen type (Fig. 9), satisfactory results are achieved in
approximately three quarters of the patients, as reported bу Hollenbeck and Woodward.
Another method of treating the esophagus that cannot Bе reduced into the abdomen is
intraoperative dilatation, coupled with а full fundoplication, but with the 360-degree
fundoplicatiоn left in the chest. When this is done, the hiatus must bе opened widely, and
the stomach serosa must bе carefully аnchored to the diaphragm. Despite this, there is а
significant risk of progressive enlargement of the iatrogenic hiatal hernia, with further
surgical therapy necessary at а later date. An incidence of gastric ulceration in the
intrathoracic gastric роuсh is seen in these patients as well. None of these approaches,
including antireflux surgery for stricture, Collis gastroplasty, Thal fundic patch operation,
or intrathoracic Nissen fundoplication, is uniformly satisfactory in patients with stricture.
Excellent results, including the relief of dysphagia and long-term control of reflux, are
reported in approximately three quarters of the patients after аnу of these procedures.
When а recurrence develops after previous surgical therapy for а stricture, it is unlikely
that further attempts at repair will bе successful. In such complicated reoperative cases, а
resection of the damaged esophagus with аn intestinal interposition using either left colon
or jejunum is highly satisfactory. The use of stomach to reconstitute the esophagus after
resection is not advocated for bеnign disease, because the incidence of reflux fоllowing
esophagogastrostomy is too high. The risk of rеcurrеnt esophagitis and stricture is
minimized bу the interposition of an intestinal segment from the esophageal remnant
through the diaphragm and into the stomach. Although this operation yields excellent
results, it is а procedure of greater magnitude than аnу of the others and so should bе
reserved for those patients who have recurrent strictures after failure of previous operative
attempts.
Literature.
1. Short Practice of Surgery by Charles V. Mann and all.
2. Textbook of surgery by Sabiston
3. Lectures
Approximate actions base.
1. Introduction /5 min/. Teacher short characterizes topic actuality, meets students
with main aims of the study and plan.
2. Initial knowledge’s control /15 min/.
3. Individual students work with patients /30 min/. The teacher explains some
more difficult and important parts of problem. The choice is realized by asking of
students and their answers correction.
4. Clinical analyses of topical patients /100 min/. Students observe topical
patients under teaches control. After it finishing, the students report about
receiving results.
5. Work in dressing-room and operation theater. Teacher and students change the
dressings of patients after different surgical procedures on esophagus.
6. Study of X-ray pictures.
7. Final knowledge control. Solution of test-questions /25 min/.
8. Conclusion /5 min/. The teacher concludes the session and gives new task for
the next once.
Test questions.
1. Choose the most accurate diagnostic method of gastro-esophageal reflux.
a) X-ray examination
b) esophagoscopy/
c) US-scanning
d) CT-scanning
2.
a)
b)
c)
d)
e)
f)
Clinical picture of gastro-esophageal reflux includes the following:
heartburn/
regurgitation/
substernal chest pain/
dysphagia/
vomiting
abdominal pain
3.
a)
b)
c)
d)
e)
f)
Note the main complications of the types II, III and IV hiatal hernia:
gastric volvulus/
bowel strangulation/
ulcerative bleeding/
respiratory insufficiency/
coronary insufficiency
malaise
4.
a)
b)
c)
How many severity grades does esophagitis have?
2
4/
5
5.
a)
b)
c)
d)
e)
Enumerate the arteries, which supply the diaphragm by blood.
inferior phrenic arteries/
musculophrenic arteries/
aa. Intercostals/
a. gastrica sinistra
aa. bronchialis
6. What part of the diaphragm is ruptured more often in case of blunt abdominal
trauma?
a) the right part
b) the left part/
c) both parts
7.
a)
b)
c)
Note the main principles of the anti-reflux surgery:
mobilization of the cardia and lower esophagus/
plication of the stomach around the intra-abdominal segment of esophagus/
narrowing of the esophageal hiatus/
8.
a)
b)
c)
d)
e)
Choose the drugs for medical treatment of the gastro-esophageal reflux:
Antacids/
H2-receptor antagonists/
tranquilizers
muscle relaxants
anticholingergic drugs
9.
a)
b)
c)
d)
e)
f)
What should the patient avoid in case of gastro-esophageal reflux?
lying down after meals/
sleeping in a semirecumbent position/
lying on the left side at night
heavy work/
excessive bending/
eating small meals