Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
UDK 616.36-006.04-07-089
DOI :10.2298/ACI0804023A
/STRU^NI RAD
99m
Tc-Red Blood Cells SPECT and planar
scintigraphy in the diagnosis of hepatic hemangiomas
........
.................................
M.V. Artiko1, P.D. [obi}-[aranovi}1, S.M.Peri{i}-Savi}2,
V.M Stojkovi}2, B.I Radoman3, S.J Kne‘evi}4, S.N Petrovi}1,
B.V Obradovi}1,V. Milovi}5,
1
Institute for Nuclear Medicine, Clinical Center of Serbia
Institute for Digestive Diseases, Clinical Center of Serbia
3
Gastroenterology Dep., Clinical Center of Montenegro
4
Gastroenterology Department, Clinical Center Kragujevac
2
5
rezime
Mediclin Deister Weser Hospitals, Bad Muender, Germani
The aim of the study is the assessment of the value
of SPECT (single photon emission computerized
tomography) using 99mTc-labeled red blood cells
in the detection of liver hemangioma, in comparison to planar imaging. With planar red blood cell
scintigraphy, sensitivity of the method was 76%,
specificity 98%, positive predictive value 98% and
negative predictive value 79%. With SPECT, sensitivity of the method was 95%, specificity 98%, positive
predictive value 98% and negative predictive value
94%. The smallest lesion detected by planar red blood
cell scintigraphy was 1.2 cm, and with SPECT red
blood cell scintigraphy 0.8 cm. The use of 99mTc-labeled red blood cells SPECT improved the sensitivity
much more in smaller lesions (0.8 to 2 cm), than in bigger ones (2-5 cm). SPECT with radiolabeled red blood
cells significantlyy improves the results of scintigraphic findings, especially in the small lesions.
Key words: hemangioma, SPECT, 99mTc-red blood
cells
INTRODUCTION
H
epatic hemangiomas are present in 0.4 -7% of the
population and are the most frequent benign tumors
of the liver. They are usually small, but rarely can be
very large. The vast majority of hemangiomas of the
liver never cause symptoms or health problems. They
are more common and usually larger in women than in
men. Pregnancy and estrogen-based medications can
cause their growth. In most of the patients hemangiomas
are asymptomatic and discovered incidentally during diagnostics procedures (US, CT, MRI), as well as at laparotomy or autopsy. Only 10% of hepatic hemangiomas
reach dimensions that need surgical treatment especially if
they are causing symptoms1. Although benign, they may
influence the organ function, depending on their size and
position, causing pain, nausea or enlargement of the liver.
Rarely, larger hemangiomas can rupture, with severe pain
and bleeding into the abdomen that may be even life
threatening2. Rarely, if thrombocytopenia is present due
to large hemangiomas, laboratory blood tests are required.
When a hemangioma is suspected it must be confirmed, in
order to exclude the presence of another type of tumor,
particularly a malignant one. A biopsy of suspected hemangiomas is avoided because of their benign nature and
the potential risk of bleeding. The most of liver hemangiomas require no treatment. In the diagnosis, ultrasound, 99mTc red blood cell scintigraphy with
single-photon emission computed tomography (SPECT),
CT with contrast, MRI, as well as angiography is performed. Recently, fusion SPECT/CT and SPECT/MRI
imaging as well as imaging with hybrid SPECT/CT cameras are employed.
The aim of the study is the assessment of the value of
SPECT (single photon emission computerized tomography) in the detection of liver hemangioma, in comparison
to planar imaging.
PATIENTS AND METHODS
The study was performed with ECAM Siemens camera.
In all the patients, planar scintigraphy was performed 180
min after red blood cell labeling by i.v. application of Snpyrophosphate and, 20 min after of 740 MBq 99mTc
pertechnetate. Planar imaging was performed in anterior,
posterior and right lateral position, using matrix 128x128,
500 000 imp/view. SPECT (single photon emission computerized tomography) was performed with the same
camera, with non-circular orbit, 360 degrees, 6 degrees
and 30 s per view, step and shoot mode. Reconstruction
was performed using Butterworth filter, order 6, cut off
frequency 0.25. Analysis was performed using slice reconstruction (coronal, transversal, sagital), as well as a
dynamic three-view display of SPECT slices.
We investigated 84 patients, 59 women and 25 men between 20 and 63 years old (mean age, 42 years). There is
a total of 104 liver lesions, 88 in the right (68 single, 20
24
V. Artiko et al.
ACI Vol. LV
multiple) and 16 in the left (12 single, 4 multiple) lobe,
range from 0.5 to 6 cm. The diagnosis was confirmed according to clinical finding (after 1 year of follow up), surgery and biopsy. In the investigation, laboratory liver
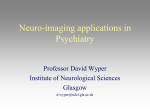
function tests and tumor markers assessment was included, as well as ultrasound (with Doppler) (Figure 1),
planar liver radiocolloid scintigraphy (Figure 2a), CT,
MRI and angiography.
RESULTS
With planar blood pool scintigraphy, there were 42 true
positives (TP), 13 false negative (FN), 1 false positive
(FP) and 48 true negative (TN) lesions. Thus, sensitivity
of the method was 76%, specificity 98%, positive predictive value 98% and negative predictive value 79%. With
SPECT, there were 52 TP, 3 FN, 1 FP and 48 TN lesions.
Thus, sensitivity of the method was 95%, specificity 98%,
positive predictive value 98% and negative predictive
value 94%. The smallest lesion detected by planar RBC
scintigraphy was 1.2 cm, and with SPECT RBC 0.8 cm.
The use of SPECT improved the sensitivity 13% for lesions from 0.8 to 2 cm, and 5% in those from 2-5 cm.
Hemangiomas were always presented as hypervascular
lesions (n=52) (Figure 2 b,c,d), although in 3 of them, hypovascular zone was found in the center. From 48 tumors
that were not proved to be hemangiomas, 3 were adenomas (one isovascular and two hypovascular), 2 were focal nodular hyperplasias (one hypovascular and one
isovascular), 15 were hepatocellular carcinomas (11
isovascular or descreetly hipervascular and 4 isovascular
with necrotic lesions). From 28 tumors which proved to
be metastases of carcinomas (colorectal, lung, bronchal,
lymphoma), all the lesions were hypovascular. FP finding
obtained by both methods was caused by the superposition of the activity from the vascular structure.
FIGURE 1.
HEPATIC HEMANGIOMA. ECHOTOMOGRAPHY. A) FOCAL LESION IN THE LEFT LOBE 54 X45 MM B) FOCAL
LESION NEAR BIFURCATION OF THE PORTAL VEIN
DISCUSSION
The majority of the results obtained by both methods
were TP or TN. FP finding obtained by both methods
was caused by the superposition of the activity from the
vascular structure, i.e. small aneurysm. FN findings were
obtained mostly because of the small size of the lesions,
13 with planar scintigraphy and 3 with SPECT (lesions
from 0.5-0.8 mm). According to our investigation, hemangiomas are nearly always presented as hypervascular
lesions, while other liver tumors may be presented as hypovascular and isovascular zones. With SPECT, sensitivity and negative predictive value are improved. Also,
SPECT allows detection of smaller lesions. These parameters are especially improved for lesions from 0.8 to
2 cm. SPECT is a time consuming procedure, including
acquisition and processing, so first, the planar imaging
with radiolabeled red blood cells should be performed.
However it is necessary all the cases when planar imaging
is negative, particularly in smaller lesions.
Literature data are similar to ours. Thus, according to
Tsai et al.2 there was no specific US pattern that would
differentiate giant hepatic hemangioma from other giant
FIGURE 2.
HEPATIC HEMANGIOMA. A) PLANAR LIVER SCINTIGRAPHY SHOWS "COLD" SPOT IN THE LEFT LIVER
LOBE (99MTC - SULPHUR COLLOID).
liver masses, but 99mTc red blood cell SPECT appeared to
separate them clearly. Intenzo et al.3 proved the value of
SPECT in additional diagnosis of cavernous hemangioma
with 99mTc red blood cell imaging, because although fourteen of hemangiomas were detected by planar imaging,
two were detected by SPECT only. However, he also
proved that two patients with large hemangiomas had
false-negative scans. El Desouki et al.4 proved that 99mTc
red blood cell scintigraphy is the noninvasive technique
most helpful in the diagnosis of hepatic hemangioma, especially in those at risk for lesion rupture or bleeding. According to him, SPECT should be performed whenever
planar imaging fails to show the lesion by 2 hours. Also,
US should precede scintigraphy for determination of the
size and the location of the lesion. Location is important
Br. 4
99m Tc-Red Blood Cells SPECT and planar scintigraphy
in the diagnosis of the hepatic hemangiomas
FIGURE 2 B
BLOOD POOL SCINTIGRAPHY WITH 99mTC - RADIOLA-
BELED ERITHROCYTES SHOWS HIPERVASCULARISATION IN THE SAME REGION, WHICH CONFIRMS
FIGURE 2 C
C) AND D) SPECT WITH
99m
TC - RADIOLABELED
ERITHROCYTES SHOWED APART OF LARGE HEMANGIOMA IN THE LEFT LOBE, MULTIPLE SMALL
HEMANGIOMAS IN THE RIGHT LOBE.
25
for optimal gamma camera acquisition, while lesions less
than 1 cm can hardly be detected, because of the spatial
resolution of gamma cameras. According to Bonanno et
al.5 99mTc red blood cell scanning is considered a highly
specific technique for the study of hepatic hemangiomas,
although planar imaging displays poor sensitivity for the
identification of small lesions. His results confirm a high
specificity of 99mTc red blood cell scanning with SPECT
(100%). SPECT significantly improves the detection of
hemangiomas (71%) compared to the delayed static study
(52%), with the largest gain for lesions between 2-3.5 cm
(83% versus 51%). However, also SPECT has difficulty
in detecting lesions of less than 2 cm. Madacsy et al6 obtained the sensitivity of planar 99mTc red blood cell scintigraphy 75% and the specificity 100%. He concluded that,
although planar imaging is probably sufficient for all
large or superficial hemangiomas, delayed SPECT should
be used with small (2-3 cm) or deeply seated lesions.
Similar to our findings, Krause et al.7 concluded that the
specificity and positive predictive values for hemangioma
was 100%. This study suggests that evaluation of dynamically displayed 99mTc red blood cell SPECT studies is
comparable to MRI in liver hemangioma bigger than 1cm.
Kagei et al.8 obtained in 40 hemangiomas, sensitivity for
planar 99mTc red blood cell imaging 35%, SPECT 50%,
US 53%, dynamic CT 82% and angiography 81%, respectively. When the tumor size was greater than 2.2 cm by
99m
Tc red blood cell SPECT and 2.8 cm by planar imaging, their sensitivity for both methods was 100%. Specificity for planar 99mTc red blood cell imaging was 100%,
SPECT 95%, US 81%, dynamic CT 100% and angiography 83%, respectively. However one patient with hepatocellular carcinoma diagnosed by angiography showed increased uptake on SPECT. Because of the highest accuracy for SPECT in hemangioma greater than 2.0 cm,
SPECT should be considered to be the method of choice
for noninvasive diagnosis of hemangioma.
In order to improve sensitivity and specificity, different
authors proposed improvements. Thus, Zincirkeser et al.9
recommends for the detection of hemangiomas located in
the unusual position, the mismatch of the SPECT delayed
images between the 99mTc-red blood cells and the 99mTc-sulfur colloid scans. Schillaci et al.10 in order to delineate the
activity from vascular system, used red blood cell
SPECT/CT hybrid imaging for accessing at the same time
morphology and function, and proved it to be the feasible
and useful in the identification or exclusion of suspected hepatic hemangiomas located near regions with high vascular
activity. Dwamena et al.11 suggested that increased perfusion
on radionuclide blood-volume imaging of hepatic hemangiomas may be a scintigraphic marker of arterioportal
venous shunting, which may identify patients with increased
risk for spontaneous rupture or identify them for the development of portal hypertension. Although the method is very
specific, some limitations causing FP findings with 99mTc red
blood cell imaging, both planar and SPECT are presented by
some authors. Thus, Ji et al.,12 proved FP finding with 99mTc
red blood cell SPECT in hepatocellular carcinoma, caused
likely by peliosis. Lim et al.13 with 99mTc red blood cell
26
V. Artiko et al.
SPECT, showed that the appearance of hepatic adenomas
can vary on 99mTc red blood cell SPECT, depending on
whether dilated sinusoid and hepatic adenomas show blood
pooling, sometimes mimicking hemangioma. The same
author14 described the case of hepatocellular carcinoma mimicking cavernous hemangioma on 99mTc red blood cell liver
SPECT. Also, Shih et al.,15 showed false-positive results for
hepatic hemangioma on 99mTc red blood cell SPECT caused
by a liver metastasis from small-cell lung carcinoma. Also,
according to Park et al.16, an early "blush" on 99mTc red blood
cell hepatic scintigraphy can be a diagnostic feature of infantile hemangioendothelioma.
CONCLUSION
The main problem for the detection of hepatic hemangioma with 99mTc red blood cell scintigraphy is the size
of the lesion. This may be partly overcome by SPECT. With
SPECT, sensitivity and negative predictive value is improved. These parameters are especially improved for lesions from 0.8 to 2 cm. Thus, SPECT is recommended in all
the cases when planar imaging is negative, particularly in
smaller lesions. The best solution for the detection of liver
hemangioma is hybrid SPECT/CT imaging which combines
anatomic and functional imaging at the same time.
SUMMARY
99m
Tc LEUKOCITA SPECT I PLANARNA SCINTIGRAFIJA U DIJAGNOZI HEMANGIOMA JETRE
Cilj rada je procena vrednosti scintigrafije pomo}u
SPECT-a (single photon emission computerized tomography) 99mTc obele‘enim eritrocitima u otkrivanju hemangioma u poredjenju sa planarnim snimanjem. Planarnom
scintigrafijom, senzitivnost metode je 76%, specifi~nost
98%, pozitivna prediktivna vrednost 98% a negativna
prediktivna vrednost 79%. Primenom SPECT-a senzitivnost
metode iznosi 95%, specifi~nost 98%, pozitivna prediktivna
vrednost 98% i negativna prediktivna vrednost 94%. Najmanja lezija otkrivena pomo}u planarne scintigrafije
obele‘enim eritrocitima iznosi 1.2 cm, a primenom SPECT-a
0.8 cm. Primena SPECT-a pove}ava senzitivnost vi{e kada
su u pitanju manje lezije (0.8 to 2 cm), nego ve}e (2-5 cm).
SPECT pomo}u obele‘enih eritrocita zna~ajno pove}ava
preciznost scintigrafskog ispitivanja, posebno kod manjih
lezija.
Klju~ne re~i: hemangiom, SPECT, 99mTC crvena krvna
zrnca
REFERENCES
1. De Blasio R, Avallone U, Donisi M, Pigna F, Di Tora
A, Sordino D, Panico C.. Hepatic hemangioma: diagnosis
and treatment. Ann Ital Chir 1996;67:233-237.
2. Tsai CC, Yen TC, Tzen KY. The value of Tc-99m red
blood cell SPECT in differentiating giant cavernous hemangioma of the liver from other liver solid masses. Clin
Nucl Med 2002; 27:578-581.
ACI Vol. LV
3. Intenzo C, Kim S. Madsen M, Desai A, Park C. Planar and SPECT Tc-99m red blood cell Imaging in hepatic
cavernous hemangiomas and other hepatic lesions. Clin Nucl
Med 1988; 13:237-240.
4. El-Desouki, M Mohamadiyeh, M al-Rashed, R Othman, S al-Mofleh I. Features of hepatic cavernous hemangioma on planar and SPECT Tc-99m-labeled red blood
cell scintigraphy. Clin Nucl Med 1999;24:583-589.
5. Bonanno N, Baldari S, Cerrito A, Zimbaro G, Restifo G, Blandino A, Freni O. Diagnosis of hepatic hemangiomas with 99mTc-labeled red blood cell scanning:
value of SPECT. J Nucl Biol Med 1991; 35:135-140.
6. Mad csy L, Kuba A, Bali I, Kalm r NK, Csernay L.
The role of SPECT-supported three-phase scintigraphy of
red blood cells in the diagnosis of liver hemangioma. Orv
Hetil 1990; 8;131:1469-1470.
7. Krause T, Hauenstein K, Schuemichen C, Moser E.
Improved evaluation of technetium-99m-red blood cell
SPECT in hemangioma of the liver. J Nucl Med 1993;
34:375-380.
8. Kagei K, Itoh K ,Tsukamoto E, Nakada K, Fujimori
K, Nagao K, Kanegae K, Furudate M. Role of 99mTc-labeled RBC SPECT in the diagnosis of hepatic hemangioma-comparison with US, CT and angiography. Kaku Igaku
1993;30:171-180.
9. Zincirkeser S, Celen ZY, Yilmaz M, Topalhan F, Sahin E. A false negative by planar scintigraphy liver hemangioma, diagnosed by technetium-99m-red blood cells
and technetium-99m-sulfur colloid single photon emission tomography scan. Hell J Nucl Med 2006;9:109-112.
10. Schillaci O, Danieli R, Manni C, Capoccetti F, Simonetti G. Technetium-99m-labelled red blood cell imaging
in the diagnosis of hepatic haemangiomas: the role of
SPECT/CT with a hybrid camera. Eur J Nucl Med Mol Imaging. 2004;31:1011-1015.
11. Dwamena BA, Belcher KK, Dasika N, Frey KA.
Focal hyperemia on RBC blood-flow imaging. A scintigraphic marker of arterioportal venous shunting in hepatic
cavernous hemangiomas? Clin Nucl Med 1997; 22:542545.
12. Ji EK, Ryu JS, Kang GH, Moon DH, Auh YH. Pelioid-type hepatocellular carcinoma masquerading as a hepatic hemangioma on technetium-99m red blood cell scintigraphy. Clin Nucl Med 2001;26:33-35.
13. Lim ST, Sohn MH, Kwak JY, Yim CY. Multiple hepatic adenomas: Tc-99m RBC liver SPECT findings with
pathologic correlation. Clin Nucl Med 2002;27:270-274.
14. Lim ST, Sohn MH. A case of hepatocellular carcinoma mimicking cavernous hemangioma on Tc-99m RBC
liver SPECT. Clin Nucl Med 2001;26:253-254.
15. Shih WJ, Lee JK, Mitchell B. False-positive results
for hepatic hemangioma on Tc-99m RBC SPECT caused by
a liver metastasis from small-cell lung carcinoma. Clin Nucl
Med 1996; 21:898-899.
16. Parl CH, Hwang HS, Hong J, Pak MS. Giant infantile hemagioendothelioma of the liver. Scintigraphic diagnosis. Clin Nucl Med 1996;21:293-295