Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
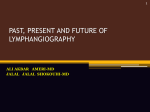
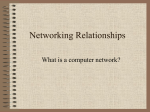
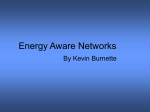
eau-ebu update series 5 (2007) 223–231 available at www.sciencedirect.com journal homepage: www.europeanurology.com Sentinel Node Evaluation in Prostate Cancer Willem Meinhardt * Netherlands Cancer Institute/Antoni van Leeuwenhoek Hospital, Plesmanlaan 121, 1066 CX Amsterdam, The Netherlands Article info Abstract Keywords: Lymph nodes Lymphadenectomy Prostate cancer Radioguided surgery Sentinel node Objectives: Provide an overview of the use of the sentinel node (SN) technique in prostate carcinoma. The relevance of nodal staging in the several stages of prostate carcinoma, technical aspects of the SN technique, indications, and lessons learned from it are discussed. Introduction: The lymph node status is relevant in all M0 tumour stages. In early prostate cancer the changes of nodal involvement are so low that invasive diagnostics are superfluous. However, the definition of this early stage is narrowing since the results of extensive node dissection have shown that previously assumed low-risk patients may harbour positive lymph nodes. On the other hand, in locally advanced cases, if the decision for external-beam radiation on the lymph node basins in combination with radiation of the prostate and 3 yr of hormonal therapy has been made, a lymph node dissection seems superfluous. Methods: SN dissection may be performed in open surgery or as a laparoscopic technique. A radioactive tracer is injected into the prostate and on g-camera imaging it is decided which lymph nodes are the possible first landing zones for the prostate tumour. During the radioguided surgery, the excision of the SNs, a handheld g probe is used to identify the radioactive nodes. On introducing the method in a clinic, it is important to do a conformal extensive pelvic lymph node dissection as well to ensure that logistics and the performance are reliable. Results: SN dissection is as reliable as a diagnostic tool as extended pelvic lymph node dissection. Because it may show cancer-bearing nodes outside of the region of the extended lymph node dissection, such as the presacral area, it may on occasion be even more sensitive. Discussion: The SN technique is likely to have fewer complications compared to the extended lymph node dissection. On the other hand, an extended lymph node dissection may still be indicated when the SN procedure yields only a few positive lymph nodes and definite cure is still the aim. Weighing the advantages and disadvantages of the laparoscopic versus the open SN technique is not different than in any other procedure. In the near future, sophisticated imaging techniques will identify nodes that are suspicious for micrometastases. This will make minimal invasive methods to confirm the nodal status not superfluous, but more in demand. Conclusion: When the nodal stage is important for treatment decisions, only extended dissections or the SN method will provide accurate staging. The SN procedure is less invasive and will avoid an extensive node dissection in the majority of cases. # 2007 European Association of Urology and European Board of Urology. Published by Elsevier B.V. All rights reserved. * Tel. +031 (0) 205129111; Fax: +031 (0) 205122554. E-mail address: [email protected]. 1871-2592/$ – see front matter # 2007 European Association of Urology and European Board of Urology. doi:10.1016/j.eeus.2007.07.003 Published by Elsevier B.V. All rights reserved. 224 eau-ebu update series 5 (2007) 223–231 1. Introduction 1.1. Brief history Even 30 yr ago studies showed that prostate carcinoma lymph node metastases have their first landing zones in lymph node areas around the internal iliac artery, obturator fossa, external iliac artery, common iliac artery, and presciatic and presacral areas [1]. However, this was the era of rather late diagnosis and most men with positive nodes had involvement of more than one area. When diagnostic methods improved, the attention shifted towards risk assessment and defining a group of patients in whom a node dissection could be avoided [2]. For patients who were candidates for perineal prostatectomy or external-beam radiation, a strong case was made for laparoscopic lymphadenectomy. After the introduction of laparoscopic pelvic node dissection for prostate carcinoma, studies comparing minilaparotomy with laparoscopic resection were done. The number of nodes excised in these studies and the limitations of the laparoscopic technique in the early days have somehow made a pelvic node dissection synonymous with clearing the obturator fossa only in many urologic practises [3,4]. More recently, publications of urologists who documented their practice of extended lymph node dissection have caused reasons for concern [5,6]. Dissection of only the obturator fossa misses, in some series, up to 75% of the clinically occult metastasis [7]. The sentinel node (SN) concept was first developed by Cabanas and applied to patients with penile carcinoma. With lymphangiography studies he assessed the location of the first lymph node from the lymphatics of the penis. Excision of only this node on both sides was believed to give sufficient proof of lymph node involvement [8]. The SN procedure is a diagnostic procedure. In case of penile carcinoma it was used as a tool to decide if a complete lymphadenectomy was indicated or not. Unfortunately, the method was not reliable enough. Morton described the dynamic SN procedure. By injecting a dye and a radioactive tracer in or near the tumour, the spread of the tracer could be followed on a g camera and the first landing zones could be visualised. With a handheld probe these nodes may then be identified during surgery [9]. The method proved to be of great use in patients with breast carcinoma and those with melanoma [10,11]. The benefit for the patients was great because many could be spared a regional lymphadenectomy and the disfiguring arm oedema that sometimes follows. In urology the dynamic SN procedure was pioneered by Horenblas on men with penile cancer, and it developed into a very reliable diagnostic method [12]. The success in penile carcinoma may be attributed to several factors. The tumour as injection site is easily accessible. The first landing zone, the groin, is a superficial area, so the SN procedure is a minor operation. But most of all, the squamous cell carcinoma of the penis never skips the lymph nodes of the groin. Metastases elsewhere without a positive lymph node in the groin are not seen, unless there is a sarcomatoid component in the tumour [13]. Unfortunately, these factors are not present in other urologic cancers. So a lymphadenectomy is still considered the standard diagnostic procedure for bladder and prostate carcinoma by many urologists. Wawroschek showed the feasibility of the SN procedure in patients with prostate carcinoma [14]. 1.2. Indications for assessment of the nodal status The risk assessment of the likelihood of nodal involvement and the practice to refrain from lymph node dissection in the lower risk groups is in doubt since the publication of incidence figures of node involvement in the low-risk groups with extended lymph node dissection [5,6]. The group of patients in whom a node dissection can be omitted safely is probably more limited than generally agreed in recent years. Prostatectomy patients may have a survival benefit from complete node dissection [7,15]. In patients with a low nodal metastatic load this may be simply due to the removal of all tumour. There is also the statistical effect on survival in the pN0 and in the pN+ groups by better allocation of patients with micrometastases. For patients with two or more nodes it might be mainly a prolongation of their progression-free survival. (For a detailed discussion, see Dhar et al [16].) According to other experts, adjuvant hormonal treatment is indicated in node-positive prostatectomy patients; N1 patients will then have almost the same 10-yr cancer-specific survival as N0 patients, but N2 and N3 patients will still do worse [17]. Another development that makes accurate staging important is the use of radiotherapy in appropriate candidates. Since the introduction of conformal radiotherapy, it is possible and profitable to give very high doses to the prostate. However, when the lymph node basins are to be radiated as well, the radiation dose safely given to the prostate is restricted. To make this type of treatment decision a reliable assessment of the nodal involvement is mandatory. eau-ebu update series 5 (2007) 223–231 A study on outcomes of radiotherapy suggests that patients will not benefit from adjuvant hormonal therapy in T1/T2, Gleason score < 7 if they have a proven pN0 [18]. Three years of hormonal treatment may be avoided in these patients by a reliable nodal status assessment. 1.3. Prognostic significance of the nodal status Prostate-specific antigen (PSA), clinical tumour stage, and Gleason sum score are already powerful prognosticators. Several nomograms are available to combine them and make reliable predictions of the possibility for definite cure [19,20]. However, accuracy is 70–80% [21]. This may not appeal to the patient as a tool to make major treatment decisions. Thus, in many patients with an apparently organconfined cancer additional diagnostics are still desirable. In a population-based study of men with prostate carcinoma with pN+, M0, the majority on conservative treatment, the cancer-specific survival rate was 72% at 5 yr and the median survival was 8 yr [22]. In this study, Gleason sum score tended to make a difference in survival, but T category, PSA level, or treatment did not affect the outcome. In a cohort of patients treated with external-beam radiation, the prognosis of N+ patients was much worse [23]. The risk of dying of prostate cancer at 10 yr was 17% for N0 patients and 57% for N+ patients. A significant difference in survival was not found between the N1, N2, and N3 patients, despite 225 extensive lymphadenectomy in the N1 and N2 patients. However, in this old series, the radiation dose would be considered low these days. Studer did find differences in tumour-specific survival between patients with one, two, and more than two affected nodes. After meticulous lymph node dissection and prostatectomy, but without adjuvant therapy, the median survival in patients with more than two positive nodes was reached at 6 yr, but patients with only micrometastasis had a 10-yr disease-specific survival of 80% [14]. 2. Methods Before surgery a radionuclide is injected in two to six portions into the peripheral zone of the prostate, guided by transrectal ultrasound. Injection in both lobes is important because each prostate lobe drains mainly into the ipsilateral group of pelvic lymph nodes [24]. The peripheral zone is the target; its drainage pattern is not different from the other zones [25]. Several carriers of the radionuclide (99mTc) are in use. Comparisons for prostate cancer have not been done as yet (for a discussion, see Beri and Janetschek [26]) After 15 min, scintigraphy is performed on the g camera and repeated after 2 and 4 h, to distinguish a ductectasy of a lymph vessel from a real node and to decide which lymph nodes are first echelon and which nodes are second echelon. After 4 h the pattern does not change significantly [27]. Single-photon emission computed tomography/computed tomography (SPECT/CT) is an asset, providing additional anatomic information and, according to some authors, increasing the yield of SNs [28] (Fig. 1). Surgery is performed 5–20 h after injection. A g probe Fig. 1 – Single-proton emission computed tomography/computed tomography shows anatomic details of the location of the sentinel node and so facilitates the intraoperative detection (picture by R.A. Valdés Olmos, Netherlands Cancer Institute). 226 eau-ebu update series 5 (2007) 223–231 is used in the radioguided surgery to locate the active nodes in vivo and after excision is used ex vivo to confirm the node’s activity and to separate it from adjacent fatty tissue or other nodes, and finally to check the operation field for residual activity. When the method is introduced in a practice, a confirmatory extended node dissection is highly recommended in the beginning, to get the logistics right and to make sure the method is properly performed [29]. This is necessary because several choices must be made in terms of equipment, materials, and methods. Communication between the nuclear medicine department and the performing urologist must meet high standards, because hygienic rules of radiography need to be applied and decisions on the location of first-echelon nodes must be discussed. 3. Results 3.1. Validation The pioneers of the SN dissection for prostate cancer have performed an additional extended lymph node dissection so they could show the reliability of this method [14]. The false-negative rate is very low when compared to the gold standard, the extended pelvic lymph node dissection; in the largest series only two negative SNs were found in 207 patients with positive nodes [30]. Additional evidence of the reliability of the laparoscopic SN method is found in the fact that the diagnostic yield is twice as high compared to old pelvic node dissection series and identical to modern series of open extended pelvic lymph node dissection [26]. 3.2. Anatomic considerations SN research will answer the question which nodes are affected first of all. Careful documentation of extensive lymph node resection series will answer the question in which tumour stages excision of all tumour-bearing nodes is necessary to cure the patient and which areas must be covered. To describe the location of SNs and to communicate the extent of an extended resection, agreement must be reached on the nomenclature. Unfortunately, the literature seems to lack generally agreed-on definitions of the boundaries of the lymph node-bearing areas in the pelvic region. Surgical atlases give a rather vague description and leave room for interpretation. An example is shown in Fig. 2, where two acknowledged authorities seem to place the obturator lymph node area in different places [6,31]. As the anatomic regions are defined currently, it does not necessarily mean that the whole of that Fig. 2 – Two acknowledged authorities seem to place the obturator lymph node area in different places. This illustrates the need for unequivocal definitions of the involved anatomic sites [6,30]. (a) Extend of lymph node dissection performed; (1) external iliac, (2) obturator fossa (3) internal iliac (hypogastric). (b) The field of dissection: Region 1, paracaval; Region 2, interaortocaval; Region 3, paraaortic; Regions 4 & 5, common iliac; Regions 6 & 7, external iliac; Region 8, intercommon iliac (presacral); Regions 9 & 10, obturator; Regions 11 & 12, internal iliac. particular area is relevant for the specific aim to find affected lymph nodes. Indeed, the SNs were found to cluster around the bifurcation of the internal and external iliac artery, thus involving parts of the obturator fossa, the external iliac, the internal iliac, and communal iliac regions [27] (Fig. 3). This notion that not the whole of these regions may be relevant has been expressed before: ‘‘in a high proportion of patients a SN was located along the initial centimetres of the hypogastric artery’’ [32]. The distribution of positive lymph nodes as reported in various SN series are shown in 227 eau-ebu update series 5 (2007) 223–231 Fig. 3 – Positive sentinel nodes (SNs) cluster around the iliac bifurcation and are not scattered throughout the several anatomic sites [27]. The right side is the location of the SNs that contained prostate cancer; on the left side are the negative SNs. Table 1. Often more than one region is involved, so this is a calculation from the original publications [33–35]. The obturator fossa, together with the internal and external iliac regions, accounts for 91% of the tumour-positive sentinel lymph nodes. This agrees nicely with the definition of an extended lymph node dissection as proposed by Burkhard and Studer [36]. So the obturator fossa, the external iliac, the internal iliac, common iliac, the presciatic, and the presacral areas are all known to harbour nodes that might be the first landing zones of prostate carcinoma. The clearance of all these regions is a major undertaking (Fig. 4). For most urologists this is only justified when this manoeuvre makes the difference for definite cure. Until new imaging techniques can guide us, the borders of the extended node dissection will necessarily be arbitrary. 3.3. Complications In a previous issue of the European Association of Urology update series it was argued from the Fig. 4 – An extensive node dissection, involving the presacral area and the para-aortic nodes up to the inferior mesenteric artery is a rather large operation. Most authors define their extended lymphadenectomy template smaller (picture by the audiovisual department, Netherlands Cancer Institute). literature that an extended pelvic node dissection has a complication rate not different from the limited dissection [37]. However, since then several papers have documented a higher complication rate. Briganti et al in their paper on 963 patients report a complication rate of 19.8% for an extended open lymph node dissection, more than twice what they report for dissection of fewer than 10 nodes [38]. Clark and coworkers did a limited dissection on one side and an extended dissection on the other side on the same patients and found three times as many complications on the extended side [39]. The majority of complications were related to the development of lymphoceles. In our own experience we did not see an increase in complications when we performed extended pelvic lymphadenectomy in (open) cystectomies, but in our laparoscopic diagnostic extended dissections we experienced an unacceptable complication rate of 23% [27]. Table 1 – Distribution of positive lymph nodes as reported in various sentinel node series Weckermann et al [33] Obturator fossa Internal iliac External iliac Common iliac Presacral Other Presacral or other 24% 38% 27% — — — 10% Jeschke et al [34] 32% 29% 40% 0% 0% — — Often more than one region is involved, so calculations are from the original publications [33–35]. Corvin et al [35] 43% 20% 12% 13% 12% — — Mean 32% 29% 30 — — — — 228 eau-ebu update series 5 (2007) 223–231 Beri and Janetschek reported a 35.3% rate of procedure-related complications from the laparoscopic extended lymph node dissections, whereas for the laparoscopic SN procedure they found only an 0.8% rate of complications [26]. 3.4. Contraindications Patients with a history of transurethral resection of the prostate (TURP) had a 20% chance of an undetectable SN in one series [33]. Recent acute prostatitis (eg, after prostate biopsies) is a contraindication for the intraprostatic application of the SN tracer [34]. 4. Discussion Especially authors from the United States and Australia challenge the need for anything more than a limited lymph node dissection in combination with a retropubic prostatectomy. Their main arguments are the additional costs, the complications involved, and the low yield in their experience (3.2% for Clark et al [39] and 2.4% for Garret et al [40]). The great difference with the European findings of much higher incidence figures of nodal involvement is not yet fully explained. 4.1. Advantages of the SN procedure compared to an extended node dissection prostatectomy, the extended lymphadenectomy does not increase the number of complications in high-volume series [5,36]. When the SN procedure reveals a minor lymph node involvement and cure is still the aim, an additional extended lymphadenectomy is needed [30]. 4.3. If a laparoscopic prostatectomy is performed, the combination with a laparoscopic SN procedure is the logical combination. The open and the laparoscopic SN procedures have the same diagnostic yield, but comparisons are not made [26]. The advantages and disadvantages of a laparoscopic procedure compared to an open procedure are the same as in any procedure. Especially patients opting for an external-beam radiation treatment have much to gain by a laparoscopic procedure [35]. 4.4. Future developments 4.4.1. Treatment strategies As in other cancers, treatment strategies will be developed with (neo) adjuvant drugs other than hormones. The evaluation of the necessary studies will be more effective with stratification for the nodal status. 4.4.2. An SN dissection involves less dissection and may have a lower complication rate [26]. In 5–10% positive lymph nodes may be found outside of the extended lymphadenectomy area (Table 1). In SN techniques the nodes are presented one by one and often will be scrutinised with immunohistochemistry techniques in addition to routine microscopy [41]. This will improve the diagnostic accuracy. Especially when the patient is to undergo externalbeam radiation treatment or a perineal prostatectomy, this less invasive procedure has its merits. When the laparoscopic SN techniques develop into a widely available technique with a low complication rate, the discussion on the sense or not of assessment of the nodal status in low-risk groups may be settled in the future. Open or laparoscopic? Imaging techniques Recent developments in imaging techniques will enable us to identify lymph nodes that are very suspicious of harbouring micrometastases. (This is a node with a tumour of <2 mm diameter [42].) Aspiration biopsy is rather likely to be false negative in such a case. This will make a confirmatory excision of such a lymph node mandatory (and preferably in the least invasive way). Positron emission tomography/CT (PET/CT) will not reveal micrometastases with the present technique [43]. 4.4.3. Innovations Innovations, such as the handheld g camera, to be used during the SN operation, will make the (laparoscopic) excision of a SN easier and even more reliable. 4.2. Disadvantages of the SN procedure compared to an extended node dissection 4.4.4. It is a technically demanding procedure, especially the laparoscopic SN procedure. It involves high-tech equipment and skills. Combined with a retropubic Innovative imaging techniques will point to lymph nodes suspicious of harbouring micrometastases. When aspiration biopsy is negative, a minimal invasive excision technique, preferably image- Future perspectives eau-ebu update series 5 (2007) 223–231 guided, will be sensitive enough to confirm this suspicion or will prove that the patient is node negative. The necessary extent of the node dissection with curative intent will be based on imaging techniques. When the situation is judged to be beyond definite cure, adjuvant treatment decisions will be based, among other relevant information such as molecular tumour characteristics, on the nodal status and not on a best guess according to nomograms. [13] [14] [15] Conflicts of interest [16] The authors have nothing to disclose. [17] References [1] Golimbu M, Moralis P, Al-Askari S, Brown J. Extended pelvic lymphadenectomy for prostatic cancer. J Urol 1979;121:617–9. [2] Partin AW, Kattan MW, Subong EN, et al. Combination of prostate-specific antigen, clinical stage, and Gleason score to predict pathological stage of localized prostate cancer. A multi-institutional update. JAMA 1997;277:1445–51. [3] Shackley DC, Irving SO, Brough WA, O’Reilly PH. Staging laparoscopic pelvic lymphadenectomy in prostate cancer. BJU Int 1999;83:260–4. [4] Perrotti M, Gentle DL, Barada JH, Wilbur HJ, Kaufman Jr RP. Mini-laparotomy pelvic lymphnode dissection minimises morbidity, hospitalisation and cost of pelvic lymphnode dissection. J Urol 1996;155:986–8. [5] Heidenreich A, Zoltan V, von Knobloch R. Extended pelvic lymphadenectomy in patients undergoing radical prostatectomy: high incidence of lymph node metastasis. J Urol 2002;167:1681–6. [6] Burkhard FC, Bader P, Schneider E, Markwalder R, Studer UE. Reliability of preoperative values to determine the need for lymphadenectomy in patients with prostate cancer and meticulous lymph node dissection. Eur Urol 2002;42:84–92. [7] Allaf ME, et al. Anatomical extent of lymph node dissection: impact on men with clinically localized prostate cancer. J Urol 2004;3:849–54. [8] Cabanas RM. An approach for the treatment of penile carcinoma. Cancer 1977;39:456–66. [9] Morton DL, Wen DR, Wong JH, et al. Technical details of intraoperative lymphatic mapping for early stage melanoma. Arch Surg 1992;4:392–9. [10] Morton DL, Thompson JF, Essner R, et al. Immediate versus delayed lymphadenectomy in the management of primary melanoma. N Engl J Med 2006;355:1307–17. [11] Nieweg OE, Van Rijk MC, Valdés Olmos RA, Hoefnagel CA. Sentinel node biopsy and selective lymph node clearance—impact on regional control and survival in breast cancer and melanoma. Eur J Nucl Med Mol Imaging 2005;32:631–4. [12] Tanis PJ, Lont AP, Meinhardt W, Valdés Olmos RA, Nieweg OE, Horenblas S. Dynamic sentinel node biopsy for penile [18] [19] [20] [21] [22] [23] [24] [25] [26] [27] [28] 229 cancer: reliability of a staging technique. J Urol 2002;168: 76–80. Lont AP, Gallee MP, Snijders P, Horenblas S. Sarcomatoid squamous cell carcinoma of the penis: a clinical and pathological study of 5 cases. J Urol 2004;172:932–5. Wawroschek F, Vogt H, Weckermann D, Wagner T, Harzman R. The sentinel lymphnode concept in prostate cancer—first results of gamma probe-guided sentinel lymph node identification. Eur Urol 1999;36:595–600. Bader P, Burkhard FC, Markwalder R, Studer UE. Disease progression and survival of patients with positive lymph nodes after radical prostatectomy. Is there a chance of cure? J Urol 2003;169:849–54. Dhar NB, Burkhard FC, Studer UE. Role of lymphadenectomy in clinically organ-confined prostate cancer. World J Urol 2007;25:39–44. Cheng L, Zincke H, Blute ML, et al. Risk of prostate carcinoma death in patients with lymph node metastasis. Cancer 2001;91:66–73. Fossa SD, Lilleby W, Waehre H, et al. Definite radiotherapy of prostate cancer: the possible role of staging lymphadenectomy. Int J Radiat Oncol Biol Phys 2003;57:33–41. D’Amico AV, Whittington R, Malkowicz SB, et al. Predicting prostate specific antigen outcome preoperatively in the prostate specific antigen era. J Urol 2001;166: 2185–8. Kattan MW, Eastham JA, Stapleton AM, Wheeler TM, Scardino PT. A preoperative nomogram for disease recurrence following radical prostatectomy for prostate cancer. J Natl Cancer Inst 1998;90:766–71. Chun FK-H, Karakiewicz PI, Briganti A, et al. A critical appraisal of logistic regression-based nomograms, artificial neural networks, classification and regression-tree models, look-up tables and risk-group stratification models for prostate cancer. BJU Int 2007;99:794–800. Aus G, Nordenskjöld K, Robinson D, Rosell J, Varenhorst E. Prognostic factors and survival in node-positive (N1) prostate cancer—a prospective study based on data from a Swedish population-based cohort. Eur Urol 2003;43:627–31. Gervasi LA, Mata J, Easley JD, et al. Prognostic significance of lymph nodal metastases in prostate cancer. J Urol 1989;142:332–6. Raghavaiah NV, Jordan WR. Prostatic lymphography. J Urol 1979;121:178–81. Brossner C, Ringhofer H, Hernady T, Kuber W, Madersbacher S, Pycha A. Lymphatic drainage of prostatic transition and peripheral zones visualised on a threedimensional workstation. Urology 2001;57:389–93. Beri A, Janetschek G. Technology insight: radioguided sentinel node lymph node dissection in staging of prostate cancer. Nat Clin Pract Urol 2006;3:602–10. Meinhardt W, Valdés Olmos RA, van der Poel H, Bex A, Horenblas S. Laparoscopic sentinel node dissection for prostate carcinoma, technical and anatomical aspects. In preparation. Sherif A, Garske U, de la Torre M, Thörn M. Hybrid SPECTCT: an additional technique for sentinel node detection of patients with invasive bladder cancer. Eur Urol 2006;50: 83–91. 230 eau-ebu update series 5 (2007) 223–231 [29] Guiliano AE, Kirgan DM, Guenter JM, Morton DL. Lymphatic mapping and sentinel lymphadenectomy for breast cancer. Ann Surg 1994;220:391–401. [30] Weckermann D, Dorn R, Holl G, Wagner T, Harzmann R. Limitations of radioguided surgery in high-risk prostate cancer. Eur Urol 2007;51:1549–58. [31] Ghoneim MA, Abol-Eneim H. Lymphadenectomy with cystectomy: is it necessary and what is its extent? Eur Urol 2004;46:457–61. [32] Brenot-Rossi I, Bastide C, Garcia S, et al. Limited pelvic lymphadenectomy using the sentinel lymph node procedure in patients with localised prostate carcinoma: a pilot study. Eur J Nucl Med Mol Imaging 2005;32:635–40. [33] Weckermann D, Dorn R, Trefz M, et al. Sentinel lymph node dissection for prostate cancer: experience with more than 1,000 patients. J Urol 2007;177:916–20. [34] Jeschke S, Beri A, Grüll M, et al. Laparoscopic radioisotopeguided sentinel lymph node dissection in staging of prostate cancer. Eur Urol. In press. doi:10.1016/j.eururo. 2007.03.064. [35] Corvin S, Schilling D, Eichhorn K, et al. Laparoscopic sentinel lymph node dissection – a novel technique for the staging of prostate cancer. Eur Urol 2006;49:280–5. [36] Burkhard FC, Studer UE. The role of lymphadenectomy in prostate cancer. Urol Oncol 2004;22:198–204. [37] Heidenreich A, Ohlman CH. The role of anatomic extended pelvic lymphadenectomy in men undergoing CME questions Please visit www.eu-acme.org/europeanurology to answer these CME questions on-line. The CME credits will then be attributed automatically. 1. In prostate carcinoma, lymph nodes outside of the obturator fossa A. Are as often involved as the nodes inside of the fossa. B. Are second-echelon nodes. C. If positive, indicate an urgent need for hormonal treatment. D. Are recognised as relevant only since the last decade. 2. The presence of prostate cancer in multiple lymph nodes in cM0 patients, A. Indicates death within 5 yr. B. Makes immediate hormonal treatment mandatory. C. Makes an extended lymph node dissection mandatory. D. Is of more prognostic significance than initial serum prostate-specific antigen value. 3. The presence or absence of microscopic lymph node metastases in prostate carcinoma [38] [39] [40] [41] [42] [43] radical prostatectomy for prostate cancer. EAU Update Series 2005;3:98–106. Briganti A, Chun FK, Salonia A, et al. Complications and other surgical outcomes associated with extended pelvic lymphadenectomy in men with localized prostate cancer. Eur Urol 2006;50:1006–13. Clark T, Parekh DJ, Cookson MS, et al. Randomised prospective evaluation of extended versus limited node dissection in patients with clinically localized prostate cancer. J Urol 2003;169:145–8. Garret KL, McNeal JE, Cohen RJ. Intraoperative lymph node staging of prostate cancer: the case against. ANZ J Surg 2003;73:263–6. Wawroschek F, Wagner T, Hamm M, et al. The influence of serial sections, immunohistochemistry, and extension of pelvic lymph node dissection on the lymph node status in clinically localized prostate cancer. Eur Urol 2003;43: 132–7. Harisinghani MG, Barentsz J, Hahn PF, et al. Noninvasive detection of clinically occult lymph-node metastases in prostate cancer. N Engl J Med 2003;348:2491–9. Hacker A, Jeschke S, Leeb K, et al. Detection of pelvic lymph node metastases in patients with clinically localized prostate cancer: comparison of [18F]fluorocholine positron emission tomography-computerized tomography and laparoscopic radioisotope guided sentinel lymph node dissection. J Urol 2006;176:2014–8. A. Can be detected with the sentinel node procedure. B. Can be detected with the sentinel node procedure and with a computed tomography scan. C. Can only be detected with a 3-Tesla magnetic resonance imaging scan. D. Can be detected with the sentinel node procedure, as well as with magnetic resonance imaging, as well as with a positron emission tomography scan. 4. The dynamic sentinel lymph node dissection is preferable to an extended lymph node dissection because A. It is easier to perform. B. It is more accurate. C. There is level A evidence it causes fewer complications. D. Not true, it depends on the clinical context. 5. The dynamic sentinel node technique A. Is scientifically speaking interesting, but of little practical use. B. Always needs to be followed by an extended lymphadenectomy. C. Makes an extended lymphadenectomy unnecessary in the majority of patients. D. Was invented by Cabanas. eau-ebu update series 5 (2007) 223–231 6. The extended lymph node dissection, according to most authors, involves: A. Obturator fossa, external iliac nodes, internal iliac nodes, presciatic nodes, presacral nodes, and the common iliac nodes. 231 B. Obturator fossa, external iliac nodes, internal iliac nodes. C. Obturator fossa, external iliac nodes, internal iliac nodes, presciatic nodes. D. Obturator fossa, external iliac nodes.