Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
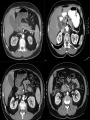
Pancreatic Cancer Review Gina Vaccaro, MD May 20, 2009 Outline Anatomy Histologic types Epidemiology Precursor lesions Presentation Treatment Anatomy of the pancreas DePinho, Nature Reviews, 2002 Anatomy of the pancreas DePinho, Nature Reviews, 2002 Histology Ductal adenocarcinoma, PDAC (>85%) Acinar cell carcinoma Pancreatic Neuroendocrine Tumor Cystic neoplasms Other- Lymphoma (NHL) DePinho, Nature Reviews, 2002 DePinho, Nature Reviews, 2002 Ductal Adenocarcinoma by the Numbers 33,730 cases/yr in US 30,000 deaths/yr 7th- 8th decade of life- peak incidence 72 years- median age at diagnosis 4th- most common cause of Ca-related death in US 15-20%- 5 yr survival if resectable 3%- 5 yr survival, all stages 2007 Estimated US Cancer Cases* Men 766,860 Women 678,060 Prostate 29% 26% Breast Lung & bronchus 15% 15% Lung & bronchus Colon & rectum 10% 11%Colon & rectum Urinary bladder 7% 6% Uterine corpus Non-Hodgkin lymphoma 4% 4% Non-Hodgkin lymphoma Melanoma of skin 4% 4% Melanoma of skin Kidney 4% 4% Thyroid Leukemia 3% 3% Ovary Oral cavity 3% 3% Kidney Pancreas 2% 3% Leukemia 19% 21% All Other Sites All Other Sites *Excludes basal and squamous cell skin cancers and in situ carcinomas except urinary bladder. Source: American Cancer Society, 2007. 2007 Estimated US Cancer Deaths* Lung & bronchus 31% Men 289,550 Women 270,100 26% Lung & bronchus 15% Breast Colon & rectum Prostate 9% Colon & rectum 9% 10% Pancreas 6% 6% Pancreas Leukemia 4% 6% Ovary Liver & intrahepatic bile duct 4% 4% Leukemia 3% Esophagus 4% Non-Hodgkin lymphoma Urinary bladder 3% 3% Uterine corpus Non-Hodgkin lymphoma 3% 2% Brain/ONS 2% Kidney 3% Liver & intrahepatic bile duct All other sites 24% ONS=Other nervous system. Source: American Cancer Society, 2007. 23% All other sites Predisposing Factors Age Smoking Chronic pancreatitis Obesity Diabetes mellitus None? Familial Syndromes Hereditary Breast and Ovarian cancer (BRCA2) Peutz-Jeghers (LKB1) Familial atypical multiple mole melanoma (p16INK4a) Lynch syndrome (MSH2, MLH1, etc.) Hereditary pancreatitis (PRSSI) Familial Syndromes Account for < 20% of the familial aggregation of PC National Familial Pancreas Tumor Registry (Hopkins)- 1200 families Familial PC- at least two 1st degree relatives Risk is 18X baseline Second degree relatives in familial PC kindreds have increased risk (3.7% vs. 0.6%) Precursor Lesions PanIN (Pancreatic intraepithelial neoplasia) MCN (Mucinous cystic neoplasm) IPMN (Intraductal papillary mucinous neoplasm) Genetic Progression Model DePinho, Nature Reviews, 2002 Regeneration Tumorigenesis DePinho, Nature Reviews, 2002 KRAS mutation is necessary, but not sufficient Activating mutations are the 1st known genetic alterations Occur sporadically in normal pancreatic tissue Detected in ~30% of early neoplasms Nearly 100% of advanced PDAC Mice with pancreas-specific KRASG12Ddevelop PanIN, can progress to PDAC in the appropriate tumor suppressor background. A Target Rich Environment DePinho, Gen Dev, 2006 Presentation Abdominal pain (Bad sign) Jaundice (Head lesions) Weight loss New onset diabetes mellitus Pancreatic enzyme insufficiency (diarrhea, floating/fatty stools) Diagnosis FNA of the primary mass or distant metastases FNA of the primary is obtainable with EUS (endoscopic ultrasound) EUS is also useful for staging, invasion into surrounding vessels (SMA, SMV) Determination of resectability Case 1 66 yo female presented with upper abdominal pain Non-smoker, father has pancreatic cancer Started on PPI by PCP Pain continued, developed anorexia, 8 lb weight loss U/S- intra and extra hepatic biliary ductal dilitation CT- 1.4cm pancreatic head mass, 18mm CBD, dilated pancreatic duct Case 1 EUS- 2 x 1.8cm pancreatic head mass, 18 mm CBD, no nodes FNA- adenocarcinoma Staged T3N0 No involvement of critical vascular structures. Underwent “Whipple” resection Case 1 Pathology: 2.5 cm ductal adenocarcinoma T4N1 (1/19 nodes) Positive SMA and radial margin Angiolymphatic and perineural invasion Poor prognosis- 5 yr survival 10-20% Recommendation- Adjuvant chemotherapy, chemoradiation (6 months) Case 2 62 yo male presented with L flank Presented to urgent care, MD palpated an abdominal mass CT done- 11 x 8 cm mass in the body of the pancreas, no mets, obliteraion of portal, splenic, SMV Also noted to have L renal stone Patient has no symptoms, no weight loss, no pain Case 2 Case 2 EUS/FNA- low grade neuroendocrine neoplasm Disease is not resectable Prognosis is good, median survival >5yrs Options: Observation Somatostin analog Chemotherapy Biologic therapy Extent of disease at presentation Localized/Resectable (15-20 %) Locally Advanced/Unresectable (40 %) Metastatic (40 %) MS 15-19 mo MS 8-12 mo MS 3-6 mo Staging (AJCC 2002) Primary TX T0 Tis T1 T2 T3 Tumor (T) Primary tumor cannot be assessed No evidence of primary tumor Carcinoma in situ (also PanIN 3) Tumor limited to pancreas, <=2cm Tumor limited to pancreas, >2cm Tumor extends beyond pancreas w/o involvement of celiac axis or SMA T4 Tumor invades celiac axis or SMA (unresectable) Regional Lymph Nodes (N) NX Regional lymph nodes cannot be assessed N0 No regional lymph node metastases N1 Regional lymph node metastases Distant Metastasis (M) MX Distant metastasis cannot be assessed M0 No distant metastasis M1 Distant metastasis Stage Grouping Stage 0 Tis N0 M0 Stage IA T1 N0 M0 Stage IB T2 N0 M0 Stage IIA T3 Stage IIB T1 T2 T3 N0 N1 N1 N1 M0 M0 M0 M0 Stage III T4 Any N M0 Stage IV Any T Any N M1 Five-year Relative Survival (%)* during Three Time Periods By Cancer Site 1975-1977 50 1984-1986 53 Breast (female) 75 79 89 Colon 51 59 65 Leukemia 35 42 49 Lung and bronchus 13 13 16 Melanoma 82 86 92 Non-Hodgkin lymphoma 48 53 63 Ovary 37 40 45 † Pancreas 2 3 5 Prostate 69 76 100 Rectum 49 57 66 Urinary bladder 73 78 82 Site All sites 1996-2002 66 *5-year relative survival rates based on follow up of patients through 2003. †Recent changes in classification of ovarian cancer have affected 1996-2002 survival rates. Source: Surveillance, Epidemiology, and End Results Program, 1975-2003, Division of Cancer Control and Population Sciences, National Cancer Institute, 2006. Why is pancreatic cancer so hard to treat? Factors to Overcome No adequate screening test High incidence of metastatic disease at presentation Fulminant clinical course Lack of adequate systemic therapies Chemotherapy resistant Radiation resistant Lack of understanding of the biology Resectable Disease Criteria for Unresectability Determined by multi-disciplinary evaluation Extrapancreatic involvement – (extensive peripancreatic nodal involvement and/or distant mets) Encasement or occlusion of the SMV or SMV-portal vein confluence – (SMV reconstruction may be feasible) Direct involvement of SMA, IVC, aorta, celiac axis Surgery (tumors of head, neck or uncinate process) Pancreaticoduodenectomy (Whipple) Operative mortality <2-3% in major surgical centers Surgery (tumors of body or tail) Often present late with larger tumors and frequent metastases Distal pancreatectomy +/- splenectomy Chemotherapy 5-fluorouracil Pyrimidine analog In use for over 40 yrs Thymidylate synthase inhibitor Pancreatic, colon, breast, esophageal, gastic cancer, etc. Gemcitabine Nucleoside analog Difluorinated analog of deoxycytidine Pancreas, breast, lung and ovarian Adjuvant Therapy Adjuvant therapy Rationale: High risk of local and systemic recurrence Overall poor prognosis 5-yr survival after resection: 25-30% node-neg vs. 10% node-pos Current standard: No universally accepted standard approach Adjuvant therapy 5 major randomized trials GITSG, EORTC, ESPAC-1, RTOG 9704, CONKO-1 Over 1200 patients studied Significant methodological differences Chemoradiotherapy in N. America (GITSG, RTOG) Chemotherapy alone in Europe (EORTC,ESPAC-1, CONKO) 5-fu based chemoradiation Trial GITSG EORTC ESPAC-1 RT dose Chemo 40 Gy(split) Bolus 5fu None None 1 yr % 2 yr % 20 (p=.01) 63 42 11 49 15 40 GY(split) CI 5-fu 17.1 (p=.099) 65 37 None 12.6 40 23 None 2x2 factorial design MS (Mo) ESPAC-1 (5-fu) Chemoradiotherapy vs. none MS 15.9 vs. 17.9 mos 2-yr survival 29 vs. 41 % 5-yr survival 10 vs. 20 % Chemotherapy vs. none Neoptolemos, NEJM 2004 MS 20.1 vs. 15.5 mos 2-yr survival 40 vs. 30 % 5-yr survival 21 vs. 8 % Kaplan-Meier estimates of survival according to whether or not patients Received chemoradiotherapy (Panel A) or chemotherapy (Panel B) Neoptolemos, NEJM 2004 ESPAC-1 Limitations Trial design (2 x 2 factorial) Possible selection bias Suboptimal radiation dose Only 70% received 40 Gy Uses 5-fu based chemotherapy Design delays initiation of adjuvant chemotherapy in the combination arm Gemcitabine-based adjuvant therapy RTOG 9704 (ASCO 2006) 442 subjects All received chemoradiation (50.4 Gy) + CI 5-fu 2 Arms: Additional 5-fu Additional Gemcitabine No overall difference in aggregate survival Head lesions only Gemcitabine arm superior MS 20 vs. 17 mos 3-yr OS 32 vs. 21 % (p=0.047) Gemcitabine-based adjuvant therapy CONKO-001 368 subjects Randomized to Obs vs. Gemcitabine x 6 cycles 10 % never received chemotherapy 62 % received all 6 cycles Gr 3/4 toxicity 7.7 % in Gem arm vs. 2.5 % in Obs Median DFS 13.4 vs. 6.9 mos (p<0.001) No difference in overall survival (22 vs. 20 mos) QOL similar in both groups Disease-free and Overall Survival (Intent-to-Treat Analysis) Oettle, JAMA 2007 Adjuvant therapy (Conclusions) Benefit of adjuvant chemotherapy is clear Gemcitabine is better than 5-fu as adjuvant chemotherapy Role of chemoradiation therapy is uncertain Clinical trial participation should be encouraged Molecularly-targeted therapies, vaccines are under investigation Future Directions Phase III: ESPAC-3 5-fu/LV vs. Gem vs. Obs Phase II: Addition of targeted agents to Gemcitabine – – – – – Bevacizumab Erlotinib Erbitux Capecitabine Oxaliplatin Neoadjuvant Therapy Rationale for Neoadjuvant therapy Intact vasculature permits maintenance of oxygenation in tissue necessary for radiation-induced necrosis Improved delivery of chemotherapy to tumor May downstage tumor 20-30% of resected patients are unable to receive adjuvant therapy Saves patients with occult metastases from morbidity of unnecessary surgery Neoadjuvant therapy No randomized studies comparing to adjuvant Small, Phase II, mostly single instituiton 5-fu and Gemcitabine chemoradiation have been studied Neoadjuvant chemoradiation can be given safely without excess surgical morbidity ACOSOG Z5041 Gemcitabine-Erlotinib Surgery Gemcitabine-Erlotinib Locally Advanced, Unresectable Disease Locally advanced, unresectable 40% of newly diagnosed patients Most with adherence to adjacent structures (celiac or SM vessels) Median survival 8-12 mos Optimal treatment is controversial Treatment options: RT alone Chemotherapy alone Concurrent chemoradiation (+/- surgery) Chemoradiation > RT alone GITSG (Morertel, Cancer 1981) 194 patients Randomized to: High dose RT Moderate dose RT + 5-fu High dose RT + 5-fu 1-yr survival: 11 % (60 Gy) 38 % (40 Gy + 5-fu) 36 % (60 Gy + 5-fu) Chemoradiation > RT alone Medicare/SEER (Krzyzanowska, JCO 2003) Large, retrospective cohort 1696 patients treated between 1991-96 Adjusted mean survival duration (weeks): Chemoradiation 47 RT alone 29 Chemo alone 27 No therapy 15 Supports the use of chemoradiation over either modality alone RT + Gemcitabine NCCN states “Radiation is usually given in combination with 5-fu chemotherapy. Recent evidence suggests that concurrent gemcitabine and radiation can yield similar outcomes.” Treatment of Metastatic Disease Efficacy endpoints Traditional tumor measurements to assess RR are often inadequate in the primary tumor site. Characteristic desmoplastic reaction and inflammatory response Recent trials have included QOL endpoints “Clinical benefit” and survival may be more accurate determinants of efficacy. Fluorouracil Extensively studied since 1950’s LV-modulated 5-fu (infusional and bolus) RR 0- 9% MS 10-24 wks Capecitabine (Cartwright, JCO 2002) Phase II study, 42 patients Chemotherapy-naive 24% achieved clinical benefit (pain intensity, analgesic use, KPS) 7% PR Well tolerated, 17% Gr 3 HFS Gemcitabine Nucleoside analog structurally similar to cytarabine Pivotal Trial (Burris, JCO 1997) 126 patients randomized: Gem 1000mg/m2 IV qwk 7/8, then 3/4 5-fu 600mg/m2 IV qwk Treatment was blinded to patients, not to investigators Primary efficacy measure= Clinical benefit response Composite of pain, KPS and weight Clinical benefit required improvement >= 4 weeks RR, TTP, OS Gemcitabine No confirmed objective responses Clinical benefit response 23.8% in Gem arm, 4.8% in 5-fu arm (P= .0022) Median survival 5.65 vs. 4.41 mos (P= .0025) Gemcitabine Combinations Gemcitabine has been combined with many other active cytotoxic agents: 5-fu Cisplatin Docetaxel Oxaliplatin Irinotecan Etc… No survival benefit has been seen over Gem alone Nieto, The Oncologist, 2008 Molecularly targeted therapy (Hochster, Cancer 2006) Nieto, The Oncologist, 2008 Targeting EGFR Gemcitabine + Cetuximab SWOG S0205 (Philip, ASCO 2007) Phase III study, 735 patients Targeting VEGF Gemcitabine + Bevacizumab Overexpression of VEGF/VEGFR are common Phase II data promising for Gem/Bev combo Phase III trial from CALGB 80303 (Kindler, ASCO 2007) Gemcitabine + Erlotinib Expression of EGFR is common, poor prognosis Phase III study from NCIC (Moore, JCO 2007) 569 patients randomized to: Gemcitabine 1000mg/m2 weekly +/Erlotinib 100mg po daily Few objective responses (8.6 vs. 7.9%) Overall survival 6.2 vs. 5.9 mos favoring combination 1-yr survival 23 vs. 17% (p=.023) Adjusted HR for death in erlotinib 0.82 (p=.038) FDA approved in 2005 in combination with gemcitabine (Moore, JCO 2007) Gemcitabine + Erlotinib 1st evidence of a survival benefit of EGFRTKI plus chemotherapy in any form of cancer 1st Phase III trial to demonstrate significant improvement in survival beyond that seen with Gemcitabine alone in pancreatic cancer Ongoing Trials Orathecin (rubitecan)- Oral Topo I inhibitor GV1001- Telomerase peptide vaccine AG-013736- Oral VEGFR/PDGFR-B inhibitor Sorafenib- Oral Raf/VEGFR/PDGFR-B/CKIT Aflibercept- VEGF Trap AZD0530- Oral Abl/Src kinase inhibitor PTK787/ZK 222584- VEGFR-TKI Romidepsin (Depsipeptide)- HDAC inhibitor MGCD0103 (MG-0103)- HDAC inhibitor Conclusions Pancreatic cancer remains a clinical challenge Current therapies offer only modest benefits Numerous studies incorporating new, targeted agents have offered little/no benefit over Gemcitabine alone. Rationally-designed combinations based on tumor biology may be more effective. Clinical trials