Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
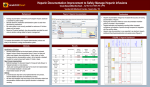
1588 either Cat: Mechanical support, left ventricular assist devices MANAGEMENT OF HEPARIN INDUCED THROMBOCYTOPENIA AND LEFT VENTRICULAR THROMBUS IN A PATIENT WITH CARDIOGENIC SHOCK H. Keshmiri1, B. Mohamedali2, G. Bhat2, A. Tatooles3, G. Sayer2 1. University of Illinois at Chicago/ Advocate Christ Medical Center Department of Internal Medicine, Chicago, IL, USA 2. University of Illinois at Chicago/ Advocate Christ Medical Center Department of Cardiology, Chicago, IL, USA 3. Advocate Christ Medical Center, Department of Cardiothoracic Surgery, Oak Lawn, IL, USA Background: Anticoagulation with heparin is the standard of care during cardiopulmonary bypass (CPB) for mechanical circulatory support (MCS) surgery. However, patients with active Left Ventricular (LV) apical thrombus and heparininduced thrombocytopenia (HIT) pose a special challenge. We report a case of a patient with LV thrombus and HIT who required MCS. Case: Forty-year-old female presented with cardiogenic shock secondary to ST-elevation myocardial infarction. She was treated with thrombectomy and drug eluting stent (DES) of the left main coronary artery. She was anticoagulated with intravenous heparin, as well as aspirin and clopidogrel for her DES. Initial transthoracic echocardiogram (TTE) indicated an ejection fraction of 10% and no evidence of LV apical thrombus. Her clinical condition continued to deteriorate requiring inotropes and an intraaortic balloon pump (IABP). Repeat TTE demonstrated a large LV apical thrombus. Decision was made to place a left-sided centrifugal pump. Postoperatively, however, patient was found to be HIT positive with an optical density of 2.6. Heparin was discontinued and patient was started on argatroban. A month later, after her optical density came down to 0.6, she was implanted with a HeartMate II left ventricular assist device (LVAD). Intraoperative heparin was utilized again and patient was immediately started on postoperative argatroban bridging with coumadin. She made progressive recovery and underwent heart transplantation. Conclusion: To the best of our knowledge, this is the first reported case of a patient with HIT and LV thrombus, who underwent sequential temporary and durable LVAD placement while receiving intraoperative heparin. We demonstrate that patients who are HIT positive with an LV apical thormbi requiring an LVAD may still undergo CPB on heparin anticoagulation.