Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
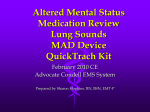
Altered Mental Status Medication Review Lung Sounds MAD Device ECRN Module I 2010 CE Condell EMS System Prepared by Sharon Hopkins, RN, BSN, EMT-P Objectives Upon successful completion of this module, the ECRN will be able to: Describe elements of normal mental status. Describe components of the neurological examination. List the three components of the Glasgow coma scale. Calculate the GCS. List common causes of an altered mental status. Objectives cont’d Review Cincinnati Stoke Scale Describe the FAST concept Review Region X SOP Altered Mental Status Explain the differences between the adult and the pediatric airway. Describe the assessment of the airway and respiratory system. Describe the various lung sounds auscultated during assessment. Objectives cont’d Discuss the methods for measuring oxygen and carbon dioxide in the blood in the prehospital setting. Identify pre-hospital indications, contraindications, dosing, side effects, and special considerations of Dextrose, Glucagon, Narcan, Albuterol, Epinephrine 1:1000, Benadryl, Lasix, and Morphine. Objectives cont’d Describe the indications, contraindications, dosing, side effects, and special considerations for administering Narcan via the MAD tool. Describe the MAD tool and the procedure for using the MAD tool. Describe the indications, contraindications, complications, and the process for performing a cricothyrotomy in the field. Normal Mental Status Consciousness Person is fully responsive to stimuli and demonstrates awareness of the environment Altered level of consciousness Some form of dysfunction or interruption in the central nervous system Normal Mental Status Patient is awake Patient is alert – aware of surroundings Patient is oriented to person, place, & time Patient is cooperative Patient carries on normal conversation Patient able to follow/obey commands Gait is even and steady Altered Level of Consciousness Hallmark sign of central nervous system injury or illness Did You Know? When perfusion is declining, the first indicator is a changing level of consciousness The last indicator is a falling blood pressure Assessing Mental Status - AVPU A– awake V – responds to verbal stimuli P – responds to painful stimuli U- unresponsive A – “Awake” Patient is awake, alert and aware of surroundings OR Patient may be awake but confused Report what the patient is oriented to • “Oriented to person but not place or time” Key is watching for a change in level of consciousness from the baseline taken V – Verbal Response This would need to be evaluated prior to touching the “unconscious” patient Problem: If trauma is involved, need to manually control the C-spine before causing the patient any movement of the c-spine If possible, call the patient’s name to check for response to verbal stimuli prior to making physical contact P – Painful Response Does not necessarily mean you have to perform a painful task to check for response Start with simple tactile contact – touch Add deeper stimulation if needed • Sternal rub • Pinch of thumb web space • Trapezius muscle squeeze (near neck) Do not cause so much trauma as to leave marks/bruises Observe for some kind of response with muscles Patient Response Patient response can include: Opening of eyelids even briefly Fluttering of eyelids Wrinkling of brows Most important is looking for changes in the patient’s response from one evaluation/assessment to the next U - Unresponsive The patient has NO response at all No moaning No muscle twitch at all • No eyelid flutter • No wrinkling of the eyebrow Muscles are flaccid with absolutely no response regardless of stimuli Neurological Exam In the Field AVPU – what is level of consciousness? Pupillary response Movement of distal extremities Sensation of distal extremities Wiggling fingers and toes Ability to feel contact with fingers and toes GCS <10 or deteriorating mental status patient is considered critical and categorized as Category I trauma Glasgow Coma Scale - GCS The best score possible is given More important is watching the trend than relying on any one score Objective tool All using the tool on the same patient should get the same score Evaluate Best eye opening Best verbal response Best motor response GCS – Eye Opening 4 – Spontaneous; patient’s eyes are open 3 – Eyes open or motion is made to verbal stimuli Start with soft voice, may have to yell at patient to open eyes 2 – Eyes open with tactile or painful stimuli Does not have to be focusing Start with gentle touch; may need to add more intense stimuli 1 – No eye opening; no muscle motion at all GCS – Verbal Response – Oriented to person, place, and time 4 – Pleasantly confused 3 – Inappropriate words 5 2 1 You can understand the word(s) spoken but they are not within context – Incomprehensible words – sounds No intelligible word understood; moans and groans; makes noises – Silent; no noise is made at all GCS – Motor Response – Obeys commands 5 – Localizes pain / purposeful movement 6 4 Can push you away or grab at the noxious stimuli (IV, collar, bandaging, your hands) – Withdrawal No longer localizing, just withdraws/pulls away to get away from annoying/painful stimuli (IV, collar, bandaging, your hands) Motor cont’d 3 2 1 – Flexion to pain Arms flex/bend slowly toward center of chest when any stimuli applied – Extension to pain Arms slowly extend and curl inward and legs straighten when any stimuli applied – No movement at all GCS Results range 3 – 15 Minor head injury – 13 – 15 Moderate head injury – 9 – 12 Severe head injury (coma) - <8 Score Significant mortality risk Consider intubation or other means to secure the airway GCS Practice Read the following case scenarios Determine the best eye opening, verbal response, motor response When the response is asymmetrical, award the highest points possible Don’t guess or assume what you think they really can do Award points for what is performed Be objective Note: Answers follow the practice slide GCS Case #1 Patient lying in the bed (no trauma), eyes are closed You need to yell the patient’s name and then the eyelids flicker They are mumbling They are grabbing at your hands and pushing you away. They have pulled out the IV. GCS Case #1 Score Eye opening – 3 Responded to loud voice Verbal Mumbling is incomprehensible words/sounds Motor response – 2 response – 5 Patient can recognize (localize) what feels obnoxious and what he wants to stop so they are grabbing at you and pulling at equipment Total GCS - 10 GCS Case #2 Patient is lying in the street watching you approach They mumble as you talk to them They are grabbing at your hands and pushing you away GCS Case #2 Score Eye opening – 4 Spontaneous; doesn’t necessarily indicate focusing Verbal Mumbling, moaning, groaning Motor response – 2 response – 5 Purposeful movement by grabbing at what the patient perceives as noxious stimuli Total GCS - 11 GCS Case #3 Patient watches your approach and acknowledges your presence Patient answers most questions and thinks you are their relative come to visit Patient able to move left arm to command but not able to move right arm (new onset – possible stroke) GCS Case #3 Score Eye opening – 4 Spontaneous Verbal Pleasantly confused Motor response – 4 response – 6 Highest possible score based on the arm that can and does move Total GCS - 14 GCS Case #4 Child’s eyelids flicker when deformed extremity is manipulated Child moans out when painful areas are manipulated Child pulls away when touched and tries to turn away from EMS GCS Case #4 Score Eye opening – 2 Response to painful stimuli Verbal response – 2 Moans and groans are incomprehensible words / sounds Motor response – 4 Withdrawing from what is sensed as painful stimuli Flexion would be slow flexing of arms toward center of chest – this patient’s response is not flexion Total GCS – 8 (Protect airway; consider intubation) GCS Case #5 Patient’s eyes remain closed; no eyelid movement at all There are no sounds heard from the patient The patient straightens their arms, twists their wrists, arches their back, and straightens their legs when stimulated GCS Case #5 Score opening – 1 (no response) Verbal response – 1 (no response) Motor response – 2 Eye Abnormal extension The worse level of response prior to no response at all Total GCS – 4 Patient is critical; Category I Patient usually needs some airway intervention Common Causes of Altered Mental Status A – acidosis, alcohol E – Epilepsy I – Infection (brain, sepsis) O – Overdose U – Uremia (kidney failure) T – Trauma, tumor, toxins I – Insulin – hypo or hyperglycemia P – Psychosis, poison S – Stroke, seizure Initial Patient Assessment Airway Open or obstructed Maneuvers needed to open • Head tilt / chin lift • With trauma, modified jaw thrust Breathing Quality Quantity (eyeball assessment at this time) Initial Assessment cont’d Circulation Quality Quantity (don’t count; get estimate of range) Disability AVPU GCS Expose – need to obtain baselines to examine Can’t evaluate or fix what you can’t see Assessment Tools AVPU Alert (interpreted as an awake patient) Responds to verbal stimuli Responds to painful stimuli Unresponsive Assessment Tools GCS Best eye opening response Best verbal response Best motor response Scores range from the lowest of 3 to highest of 15 Obtain and document GCS on all patient calls Cincinnati Stroke Scale Obtain for suspicion of TIA or stroke Evaluate for facial droop Check the patient’s symmetry during a broad, big smile (teeth showing) Evaluate for arm drift Check for weakness in holding arms outstretched, palms up, for 10 seconds Evaluate for clear speech Have patient repeat words listening for clear speech patterns Airway Protection and the Stroke Patient Crucial - high mortality rate for aspiration Is airway patent and can patient protect their own airway? Check if patient is able to handle & swallow own saliva • Detailed/involved swallow study done in-hospital Patient speaks in clear unobstructed voice Interventions to consider Have suction on and ready Ability to quickly turn patient onto their side FAST - Public Educational Tool Tool developed by organizations for public recognition of stroke and to encourage FAST action Region X SOP – Altered Mental Status Consider etiology If cause of problem can be identified, then interventions can be focused • Diabetes – check blood sugar • Drug overdose – what are the environmental clues • Poisoning – environmental evidence around • Alcohol related – environmental evidence; use your nose SOP – Altered Mental Status Maintain airway Patency extremely important Evaluate rate and quality If respirations inadequate, ventilate • 1 breath every 5-6 seconds all patients – infancy to elderly Intubate as necessary Use C-spine precautions as indicated If any doubt, err on side of extra precautions Provide Routine Medical Care IV – O2 - monitor SOP – Altered Mental Status Obtain blood glucose level If <60 – treat • Adult - Dextrose 50% 50 ml IVP • Child 1 – 15 – Dextrose 25% 2 ml/kg • Infant <1 – Dextrose 12.5% 4 ml/kg Dilute 1:1 ratio D 25% with normal saline Equal amounts of product make 1:1 dilution (Dextrose and normal saline) Treating Altered Mental Status In absence of IV access • Adult – Glucagon 1 unit (1 ml) IM • Pediatrics < 15 – Glucagon 0.1 mg/kg IM Max dose of 1 mg Practice math: 44 pound child with no IV access • How many kg? 44# 2.2 = 20 kg • 20 kg x 0.1mg/kg = 2 mg • How much Glucagon do you give? Max of 1 mg (max drugs at adult dose) Altered Mental Status cont’d If patient not alert, respirations decreased, or narcotic overdose suspected: Narcan 2mg IN/IVP/IO • Repeat every 5 minutes as needed until desired effect Quality of respirations have improved Don’t need patient to be 15 on GCS Don’t need patient awake necessarily • Maximum total dose 10 mg Transport Altered Mental Status cont’d Note: Attempt to identify substances involved If not a safety hazard, obtain and transport substance container with the patient Consider use of restraints prior to administration of Narcan • Patient may become violent when level of consciousness improves Adult Airway Note Pediatric airway funnel shaping of pediatric airway Notice Difference in Tongue Size Adult airway tongue Pediatric airway Pediatric airway Differences Jaw smaller Teeth softer and more fragile Tongue relatively larger Potential to produce more obstruction Epilgottis floppier and rounder Recommend straight Miller blade over curved Macintosh for intubation Larynx more superior & anterior Higher and more forward Funnel shaped due to underdeveloped cricoid cartilage • Under age 10 cricoid cartilage narrowest part of airway Ribs and cartilage softer and more pliable Children rely on diaphragm muscle for breathing Airway Assessment Inspection Begin as you are approaching the patient Auscultation Listen for audible sounds, then use stethoscope Palpation Can gather a lot of information through the art of touch Assessment of Airway Initial assessment ABC’s • Airway open? Fully open with adequate air exchange? Partially or fully obstructed with poor air exchange? • Are they breathing? Look for chest rise and fall Listen for air movement Feel for air movement • Do they have a pulse? Airway Assessment cont’d Inspection Evaluate adequacy of breathing Note any signs of trauma Assess skin color • Paleness and diaphoresis due to sympathetic stimulation in early respiratory compromise • Cyanosis if deoxygenated (LATE SIGN!!!) Patient positioning • Tripod – leaning forward (CHF? Asthma?) • Orthopnea – can’t lay down (CHF? Asthma?) Inspection cont’d Observe for dyspnea • May cause or be caused by hypoxia • Prolonged dyspnea can lead to anoxia (absence of oxygen) • Is dyspnea a new onset or perhaps chronic in the patient with long standing COPD Abnormal Respiratory Patterns Kussmaul’s Deep, slow or rapid, gasping breathing Commonly found in diabetic ketoacidosis in attempt to blow off excess CO2 (acid) Cheyne –Stokes Progressively deeper, faster breathing alternating with gradually shallow and slower breathing Indicates brainstem injury Respiratory Patterns cont’d Biot’s Central neurogenic hyperventilation Irregular pattern of rate and depth with sudden, periodic episodes of apnea Indicates increased intracranial pressure Deep, rapid respirations Indicates increased intracranial pressure Agonal Shallow, slow, or infrequent breathing Indicates brain anoxia, impending death Respiratory Assessment cont’d Auscultation Listen 1st audibly for any abnormal sounds Have patient cough to clear loose secretions Then listen with stethoscope • Right and left apex (under clavicles) • Right and left bases (8th – 9th intercostal space, midclavicular) • Right and left lower thoracic back or right and left midaxillary line (lateral chest wall) Auscultation cont’d Posterior aspect preferable to anterior surface Less tissue mass Lungs closer to the surface Less interference with heart sounds Anterior and lateral sections of the chest are more accessible especially in supine patients Evaluate for symmetrical equality Keep stethoscope in place long enough to hear end of exhalation Many abnormal sounds heard first at end of exhalation Abnormal Lung Sounds Snoring Partial obstruction of upper airway, usually from tongue Patient needs airway repositioned Gurgling Accumulation of fluids (blood, vomitus, other secretions) in upper airway Stridor Harsh, high-pitched sound heard on inhalation; usually indicates laryngeal edema or constriction Lung Sounds cont’d Wheezing Musical, squeaking, or whistling sound heard in inspiration and/or exhalation Indicates bronchiolar constriction • Asthma, COPD Quiet Diminished or absent breath sounds ominous Indicates serious problem with airway, breathing, or both Lung Sounds cont’d Crackles (rales) Fine, bubbling sound heard on inspiration, sounds like velcro ripping Indicates fluid in smaller airways • CHF • Pneumonia Gas exchange may be compromised Rhonchi Course, rattling noise heard on inspiration Associated with inflammation, mucus, or fluid in bronchioles Gas exchange may be compromised • Chronic bronchitis Airway Assessment Palpation Often forgotten assessment tool Palpate chest wall for • Tenderness • Symmetry • Abnormal motion • Crepitus (bone crunching) • Subcutaneous emphysema Air leakage into tissue Pulse Oximetry Measures hemoglobin oxygen saturation in peripheral tissue Non-invasive means to measure effectiveness of oxygenation and ventilation Continually reflects changes May detect changes faster than assessment of vital signs Pulse Oximetry Place probe over a peripheral capillary bed Fingertip, toe, earlobe 2 sensors take measurements of light reaching them from 2 light emitting diodes Oximeter calculates ratio of light received • Influenced by amount of oxygenated versus deoxygenated hemoglobin SpO2 determined Suggested SpO2 Results – 99% - normal 91 -94% - mild hypoxia 95 Perform additional evaluation Administer supplemental oxygen 86 – 91% - moderate hypoxia Perform additional evaluation Administer 100% supplemental oxygen <85% - severe hypoxia Immediate intervention required SpO2 Error Results Current equipment more accurate; less error readings False readings possible Carbon monoxide exposure – false high High-intensity lighting near sensors Hemoglobin abnormalities Absent peripheral pulses Hypovolemia; severe anemia • SpO2 may be normal but the amount of hemoglobin available is low Coordinate readings with patient assessment Capnography Graphic recording or display of measurement of expired CO2 over time End-tidal CO2 (ETCO2) – measurement of CO2 concentration at end of expiration Provides information Systemic metabolism (production of CO2) Circulation Ventilation How Does CO2 Circulate? CO2 is normal end product of metabolism Transported by venous system to right side of heart Pumped from right ventricle pulmonary artery lungs and pulmonary capillaries Diffuses into alveoli Removed from body via exhalation Poor Perfusion States Shock, cardiac arrest, pulmonary embolism, bronchospasm, incomplete airway obstruction (ie: mucous plugging) Perfusion decreased ETCO2 will reflect pulmonary blood flow and cardiac output Will not reflect ventilation in poor perfusion states End Tidal CO2 Detector Contains pH sensitive chemically impregnated paper to estimate ETCO2 level Color change is reversible Will reflect changes breath to breath Paper will be unreliable if contaminated with acidic drugs or gastric contents Tool placed near elbow on BVM Interpreting the ETCO2 – indicates measured CO2 being exhaled Yellow Evaluate after 6 breaths Tan – low levels of CO2 measured Misplaced tube or poor carbon dioxide production • Evaluate tube positioning • Evaluate patient perfusion Blue or purple – no CO2 being measured Suspect unsuccessful intubation ETCO2 Applications Verify placement of endotracheal tube Assess effectiveness of CPR • CO2 levels fall abruptly at onset of cardiac arrest • CO2 levels begin to rise with effective CPR Medication Review (Information based on Region X EMS usage) Indication Contraindication Dosing Side effects Special considerations Dextrose Carbohydrate used to raise the sugar level No contraindication in suspected hypoglycemia Administered when the blood sugar level is less than 60 Dose based on age Adult 16 and over – 50% 50 ml slow IVP 1 – 15 – D 25% - 2 ml / kg slow IVP <1 – D 12.5% - 4 ml / kg slow IVP • Mix 1:1 dilution with D25% and normal saline Dextrose cont’d Local vein irritation may occur especially when small veins are used If glucagon was administered and then an IV site is secured, retest the blood sugar level If blood glucose remains <60 and patient condition not improved, administer Dextrose Glucagon Hormone to stimulate breakdown of glycogen (stored form of glucose) Patient may have an allergic reaction if they have allergies to proteins Adult dosing – 1 mg (1 unit) IM Pediatric dosing up to 15 years old – 0.1 mg/kg (max dose 1 mg – 1 unit) Glucagon cont’d Observe for nausea and vomiting May take up to 20 minutes for Glucagon to be effective Will not have any effect if there are no stores of glycogen in the liver Patient requires rapid transport and continued efforts at IV access Drug must be reconstituted prior to administration Albuterol Ventolin, Proventil Bronchodilator with onset 5 – 15 minutes after inhalation Used in asthma, to reverse bronchospasm in COPD, and bronchospasm & laryngeal edema of an allergic reaction All patients inhale 2.5 mg via nebulizer Albuterol cont’d May cause tachycardia & restlessness Has greater influence in the lungs than on the heart Less effective if patient taking beta blockers at home (usually for hypertension; meds end in “alol”) Beta blockers block bronchodilation response Offer aerosol mask if patient unable to keep mouthpiece sealed between lips Albuterol Kit and Masks 2.5 mg / 3 ml Connected to O2 source Watch Available in adult and pediatric sizes for signs of exhaustion May need to be bagged Epinephrine via Nebulizer In presence of croup/epiglottits If patient not responding to 2 doses of Albuterol, provide alternate treatment • Epinephrine 1:1000 1 ml mixed with 2 ml normal saline • Mix in nebulizer • Connect to oxygen to create a mist • Assist patient while inhaling the mist Nebulized Epinephrine for moderate to severe cases Epinephrine 1:1000 A drug that mimics the sympathetic nervous system Stimulation on the vessels trigger vasoconstriction • Will raise the blood pressure Stimulation in the lungs triggers bronchodilation • Will improve air exchange Useful in asthma, COPD, allergic reactions with airway involvement, and anaphylaxis Epinephrine 1:1000 cont’d Use with caution in the elderly and those with heart disease Can strain the heart by increasing the workload of the heart (rate and force of contractions) Adult dosing allergic reaction with airway involvement – 0.3 mg SQ Adult dosing anaphylaxis – 0.5 mg IM Faster absorption in poor perfusion Epinephrine 1:1000 cont’d Pediatric dosing up to 15 years of age Allergic reaction with airway involvement • Epi 1:1000 - 0.01 mg/kg SQ • Max single dose 0.3 ml (0.3 mg) • May repeat every 15 minutes Anaphylaxis • • • • Epi 1:1000 – 0.01 mg/kg IM Max single dose 0.3 ml (0.3 mg) IM faster absorption in poor perfusion state May repeat every 15 minutes Epinephrine 1:1000 cont’d May Tachyarrhythmias Palpitations Restlessness Anxiety Headache May cause: increase oxygen demand in the heart Use cautiously in elderly and those with heart disease Benadryl - Diphenhydramine Antihistamine to block the release of histamine in allergic reactions Max effect in 1 – 3 hours Duration of effect 6 -12 hours Medication must be continued over several days or symptoms will rebound Useful in allergic reactions including anaphylaxis Benadryl cont’d Avoid use in severe, uncontrolled asthma and COPD Adult dosing Stable allergic reaction – 25 mg slow IVP or IM Allergic reaction with airway involvement & anaphylaxis – 50 mg slow IVP or IM Pediatric dosing – 1 mg/kg IVP Stable allergic reaction – max dose 25 mg Allergic reaction with airway involvement or anaphylaxis – max dose 50 mg Benadryl cont’d May cause drowsiness, headache, confusion, wheezing, palpitations, hypotension, nausea, vomiting, drying of secretions Elderly particularly sensitive to effects of Benadryl Watch for hypotension and drowsiness Lasix (furosemide) Diuretic that stops reabsorption of sodium and chloride in the kidneys Triggers dilation of the venous system Could drop blood pressure Decreases pre-load Amount of blood returning to the heart Onset of venodilation immediate Onset of diuretic effect within 15 – 20 minutes Lasix (furosemide) cont’d Useful in CHF and pulmonary edema Venodilation useful in hypertensive crisis Slight risk in persons allergic to sulfa drugs (typically antibiotics) Dosing is 40 mg IVP/IO If patient is on Lasix, they are sensitized to it Use the larger dose of 80 mg IVP/IO Lasix (furosemide) cont’d May cause headache, dizziness, hypovolemia, nausea Patient may experience temporary hearing loss and ringing in the ears with repeated doses given rapid IVP/IO over a period of time Morphine Narcotic analgesic (opioid) Reduces anxiety Creates a euphoric feeling Depresses the central nervous system (CNS) • Reduces pain sensation Dilates venous blood vessels • Decreases blood return to the heart (pre-load) Useful in ACS, pulmonary edema, pain Potentiates versed during conscious sedation Helps versed to be more effective Morphine cont’d Dosing 2 mg given slow IVP (over 2 minutes) May repeat every 2-3 minutes Maximum total dose is 10 mg Side effects Hypotension Respiratory depression Bradycardia Altered level of consciousness Morphine cont’d Opioids cause pupils to constrict Use cautiously when other depressant drugs have been taken Includes alcohol Reversal agent is Narcan Adult dosing 2 mg IVP • May repeat every 5 minutes; max total 10 mg Pediatric dosing < 20kg – 0.1 mg/kg IVP/IO/IM • Max total dose is 2mg • > 20kg – 2 mg IVP/IO/IM Narcan Narcotic antagonist with an onset within 2 minutes May cause withdrawal symptoms including seizures Adult dose – 2 mg IN/IVP/IO Repeated every 5 minutes as needed up to 10 mg Pediatric dose up to 15 years weight based <20 kg (44#) – 0.1 mg/kg IVP/IO/IM >20 kg (44# - typically a 4-6 year old) – 2 mg IVP/IO/IM Narcan cont’d Side effects are rare. Watch for hypotension, nausea, vomiting, blurred vision, opiate withdrawal (including seizures) Goal is to reverse severe respiratory depression; NOT to have an awake & talking patient Duration of Narcan may be shorter than drug it is trying to counteract Watch for return of symptoms Alternate Medication Delivery MAD Mucosal atomization device Tool to deliver medications via nasal route Medication atomized into tiny particles Nasal mucosa highly vascular • Immediate absorption into bloodstream • Onset of action within 3-5 minutes • Peak onset 15-20 minutes Using Nasal Route - MAD Unable to establish IV access Medication administration indicated Nasal mucosa intact and clear of blood and mucus MAD Luer tip can be connected to variety of sizes of syringe White wedge fits firmly into nostril Fine mist spray covers a large surface area Medication adheres to nasal mucosa versus running down the throat Each nostril can tolerate up to 1 ml volume Narcan packaged 2mg/2ml – will need to deliver 1 ml in each nostril Attaching MAD Tip to Syringe Nasal cavity suctioned as needed to clear blood or secretions • Clear nasal passages enhance absorption of medication Medication delivered in divided doses • Maximum of 1 ml per nares Inserting MAD Nasal Patient’s head controlled with one hand Need to prevent movement • MAD gently but firmly placed into one nostril • Aimed upward and toward ear on same side Syringe briskly compressed to deliver the drug as an atomized mist into nares Dispensing Mist Must briskly compress syringe to convert liquid drug to a fine atomized mist Mist results in broader mucosal coverage; better chance of absorption into the blood stream than drops that can run straight back into the throat. MAD Region X have implemented the MAD beginning with Narcan “IN” documented for route of administration Will have the potential in the future to add further medication using the MAD Cricothyrotomy, QuickTrach Indications Assisted ventilations required and all other means have failed to secure an airway Contraindications Transected trachea Less invasive maneuver will be effective Note: In ED, staff will need to assist the MD with this device – do you know how? Equipment BVM QuickTrach kit >77 pounds use 4 mm kit 22 – 77 pounds use 2 mm kit < 22 pounds use needle cricothyrotomy Skin prep material Where is your airway kit kept in the ED? QuickTrach Kit Contents Needle with syringe Cannula with wings for strap attachment Extension tubing Velcro strap QuickTrach cont’d Procedure (RN to assist MD) Assemble equipment Patient supine, neck hyperextended if no trauma Locate cricothyroid membrane and cleanse site • Soft spot palpated just below Adam’s apple • Or, start at notch, run fingers up toward head First ridge of bone palpated is cricoid cartilage Membrane is just above this bony cartilage Procedure cont’d Anchor and stretch skin slightly Puncture cricothyroid membrane at 900 angle Aspirate syringe as needle enters trachea to confirm placement • Ability to freely aspirate air Change angle of needle to 600 towards feet Advance device until stopper is flush with skin Remove stopper • Stopper will be snug; avoid motion of needle Slide plastic cannula forward until snug against skin as you remove needle and syringe • Advance cannula as you remove needle like starting an IV Procedure cont’d Hold cannula snuggly • Patient may reflexively cough and could dislodge cannula Attach flexible connecting tube to cannula proximal end Begin to bag/ventilate the patient immediately • Once every 6-8 seconds for all patients Confirm placement • Auscultation lung sounds • Adequate chest rise Finish securing cannula with neck strap Case Study #1 Your patient called 911 after dropping her tea cup and being unable to move her right side Conscious, cooperative, speech slurred VS: 175/110; P – 98; R – 18; pupils cataract Initial care started (IV – O2 – monitor) What is your impression? What specific assessment should be done? Case Study #1 cont’d Impression Acute stroke Additional assessment Cincinnati Stroke Scale • Facial droop • Arm drift • Speech Transport decision Is CT scan available at receiving hospital? Case Study #2 EMS is at a local school for a patient with asthma Assessment taken walking towards child Sitting upright In obvious distress • Use of accessory muscles – neck, intercostal • Increased respiratory rate • Panic on their face Impression • Severe acute asthma attack Is assessment done after vital signs? Case Study #2 cont’d Assessment performed Observation / visual inspection Initial ABC’s • To determine presence of life threats Breath sounds auscultated • Bilateral wheezing heard predominately on exhalation Obtain vital signs • 98/62; P – 110; R – 28 and labored; SpO2 94% Case Study #2 cont’d Interventions required IV – O2 – monitor - medication Question Do you need an IV established prior to administration of medication? • No, albuterol nebulizer should be started as soon as possible • Give verbal prompts to slow breathing down, to take deeper breaths, and to eventually take and hold a deep breath Case Study #3 You are caring for a traumatically injured patient When asking them to open their eyes, you yelled their name and their eye opened briefly and then closed again They are using swear words during care provided They are pulling off equipment and grabbing at your hands while you provide care What is their GCS? Case Study #3 cont’d Eye opening To verbal – 3 points Verbal Inappropriate words – 3 points Motor response Purposeful movement – 5 points Total response GCS – 11 points Indicates moderate head injury Case Study #4 You are caring for a patient complaining of dyspnea Your patient is 62 years-old They are sitting in the tripod position They are using accessory muscles and have an increased respiratory rate With your stethoscope, you auscultate crackling sounds heard in the bases during exhalation Case Study #4 cont’d What are these breath sounds? What do these breath sounds indicate? Fluid in the smaller airways • CHF, pulmonary edema, pneumonia What medications may be indicated in the field (per SOP) for CHF? Crackles Nitroglycerin – venodilator Lasix – venodilator and diuretic Morphine – venodilator, reduce anxiety And of course, oxygen Intervention to add is CPAP Case Study #5 You received a 7 year-old patient from a local school with an asthma attack Your impression is an acute asthma attack You begin supplemental oxygen and begin to prepare to provide interventions Case Study #5 cont’d If this is an asthma attack, what signs and symptoms do you expect? Sitting up leaning forward Dyspnea with shortness of breath Increased respiratory rate Use of accessory muscles Dry mucous membranes Possibly audible wheezing Bilateral wheezing heard first on exhalation Dry, nonproductive cough Case Study #5 cont’d If you cannot hear any breath sounds, what does this mean? The airway is so constricted that no air is moving in or out – ominous What does wheezing sound like? Whistling, musical sound that can be heard on inhalation and exhalation • The louder the breath sounds the more air that is exchanging Case Study #5 cont’d What medication is indicated? Albuterol 2.5 mg (in 3 ml) nebulizer How can you help maximize the effects of the treatment? Calmly, quietly talk the patient through breathing Get the patient to slow down the breathing Get the patient to take some deeper breaths Get the patient to inhale and hold their breath periodically to get the drug into the lungs Case Study #6 You have an unresponsive male in his twenties The patient responds to painful stimuli The respirations are 6 per minute and shallow Pupils are constricted What is your impression? What interventions were necessary in the field? Case Study #6 Impression Narcotic overdose Interventions Immediately support ventilations • Bag at a rate of once every 5-6 seconds Protect the airway from aspiration Administer Narcan 2 mg (via MAD if no IV) • Administer a maximum of 1 ml per nares if using MAD Case Study #7 A patient is unable to be ventilated via BVM What options are available? Reposition the airway • Consider c-spine precautions if indicated Attempt intubation QuickTrach if unable to intubate Needle cricothyrotomy if unable to identify landmarks Case Study #7 Landmarks for Quicktrach Soft space just inferior/below thyroid cartilage (Adam’s apple) Or Start in notch and move finger upward • Feel first bony prominence – cricoid cartilage • Palpate for soft space above the cricoid cartilage Bibliography Bledsoe, B., Porter, R., Cherry, R. Paramedic Care Principles and Practices. Prentice Hall. 2009. Campbell, J. BTLS 5th Edition. Brady. 2004. Region X SOP, March 2007; amended January 1, 2008. videolaryngoscopy.com/…/AdultCobaltAirway.jpg www.wolfetory.com