Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
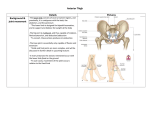
Anterior and Medial Thigh Muscles/Actions Anterior Compartment Muscles Iliopsoas (iliacus, psoas major/minor) Iliac crest, vertebrae (T12-L5) lesser trochanter Action Main: -Major flexor of the hip Other: -Flex trunk if hip fixed (sit up) -Eccentrically resists acceleration while walking down hill -Maintain lumbar lordosis -Balance trunk while sitting -Initial and mid-swing Sartorius Main: -Flex hip Other: -ABducts -ER thigh -Flex knee -IR leg Pectineus Main: -Flex hip Other: -ADduction -ER ASIS medial tibia Superior ramus pectineal line on post. Femur Quadriceps Distally all attach to quadriceps tendon patella patellar ligament tibial tuberosity Most important function: -Receive weight during loading response (flat foot) -Projection (jumping) Rectus Femoris Main: AIIS -Flex thigh -Extend knee Other: -Accelerate thigh during swing phase Vastus Lateralis Main: -Extend knee Vastus Intermedius Main: -Extend knee Vastus Medialis Main: -Extend knee Posterior femur Anterior femur Posterior femur OVERALL: Anterior compartment flexes the hip and extends the knee o If a muscle flexes hip then that means they cross the hip joint o If a muscle extends the knee then they cross the knee joint o If the muscle does both… then crosses both joints! Medial Compartment Muscle Obturator externus Obturator membrane greater trochanter Action -ER of femur -Only muscle in medial compartment that does not ADduct the thigh! Pectineus -See above Adductor Longus -Flex thigh (<70°) -Extend thigh (>70° until reaches 70° again) Adductor Brevis -Flex thigh (<70°) -Extend thigh (>70° until reaches 70° again) Adductor Magnus Adductor Part -Flexes thigh Hamstrings Part -Extends thigh Inferior ramus linea aspera Inferior ramus linea aspera Adductor Part: Inferior ramus linea aspera Hamstrings Part: Ischial tuberosity linea aspera Gracilis Pubic symphysis and inferior ramus medial tibia -IR of femur OVERALL: All of the muscles in the medial compartment do ADduction o Table above just includes the oddball movements Obturator externus and gracilis minimize vertical shifts during walking (keep the hip level) Innervation Motor: Lumbar Plexus - Anterior rami T12-L4 Anterior compartment of thigh Sacral Plexus - Anterior rami L4-S3 -Posterior compartment of thigh Anterior compartment of thigh innervated by femoral nerve (L2-L4) EXCEPT: Anterior rami of L1-L2 = psoas major and minor Pectineus can be innervated by femoral nerve but ALSO obturator nerve o This is b/c it is in both anterior and medial compartment Medial compartment of the thigh innervated by the obturator nerve (L2-L4) EXCEPT: Pectineus… see above Adductor magnus o Adductor part (flex thigh) = obturator n. o Hamstrings part (extend thigh) = tibial divison of sciatic n. Sensory: Vasculature Great and small saphenous v. femoral v. external iliac v. (becomes this at inguinal ligament) Clinical Relevance Fascial lines are important as guidelines for surgery. o Thigh region has two… lateral and medial intermuscular septum o Psoas Abscess o Abdominopelvic infections (Spinal TB/enteritis (Crohn’s)) o May be mistaken for femoral/inguinal hernia o Infection can pierce through fascia and spread causing severe referred hip/thigh/knee pain Rectus Femoris Strain o Rapid contraction following stretch (ex: soccer kick) = anterior hip pain o So basically, if you contract if too hard during swing phase. Femoral Triangle o Superior border = inguinal ligament o Lateral border = Sartorius m. o Medial border = adductor longus m. o Floor = iliopsoas/pectineus o Roof = fascia lata o Femoral Sheath (protects vessels from inguinal ligament during hip movements) o Femoral n. is in the femoral triangle but NOT in the femoral sheath!! Lateral compartment = femoral a. Intermediate compartment = femoral v. Medial compartment (femoral canal) = lymphatic Lymphatics don’t take up the whole space in the femoral canal… leads to potential femoral hernia Femoral Hernias o o Abdominal contents can herniate through the femoral ring into the femoral canal and come out through the saphenous v. opening. o More common in female’s b/c they have wider pelvis’s leading to a wider femoral ring. Femoral Artery o Can take pulse… if pulse is weak then could signify an occluded artery. o Catheters can also be inserted here and run all the way up to the heart. Gluteal Region Muscles/Actions Superficial Layer Muscles Actions Tensor Fascia Latae -AB -IR Gluteus Maximus -Extend thigh -ER Gluteus Medius -AB -IR Gluteus Minimus -AB -IR ASIS IT band lat. Tibia Ilium, sacrum, coccyx IT band, gluteal tuberosity Ilium lateral greater trochanter Ilium anterior greater trochanter Deep layer Muscles Piriformis Anterior sacrum greater trochanter Superior gemellus Ischial spine greater trochanter Obturator internus Obturator membrane greater trochanter Inferior gemellus Ischial tuberosity greater trochanter Quadratus femoris Ischial tuberosity greater trochanter Actions All do ER and AB! QF is the strongest lateral rotator of the thigh Triceps Coxae made up of superior gemellus, obturator internus, and inferior gemellus OVERALL Mainly muscles of the superficial gluteal region AB and IR EXCEPT: o Gluteus maximus ER and extends ALL muscles of the deep gluteal region AB and ER and distally attach to the greater trochanter. Innervation Alternative routes of the sciatic n. Motor Superificial layer is mainly innervated by the superior gluteal n. EXCEPT: Gluteus maximus is innervated by the inferior gluteal n. Deep layer: Ventral rami of S1, S2 = piriformis m. N. to obturator internus = superior gemelli and obteratur internus mm. N. to quadratus femoris = inferior gemelli and quadratus femoris mm. Sensory Clunial nerves Superior = top half from sacrum over to tubercle of iliac crest Middle = skin over sacrum Inferior = bottom half down to greater trochanter Ligaments Greater Foramen -Greater sciatic notch made up of sacrospinous ligament Muscles -Piriformis m. Nerves -Superior and inferior gluteal nn. -Pudendal n. Arteries -Superior and inferior gluteal aa. -Pudendal a. Lesser Foramen -Lesser sciatic notch made up of sacrospinous and sacrotuberous ligament Muscles -Obterator internus m. Nerves -Pudendal n. Arteries -Pudendal a. Note that pudendal n. and a. go through both of the foramen! Joint Capsule of the Hip Iliofemoral ligament o Anterior and superior o Prevents hyperextension of thigh Pubofemoral ligament o Anterior and inferior o Prevents over ABduction Ischiofemoral ligament o Posterior o Prevents hyperextension… but is the weakest ligament of the joint capsule o If torn then can get a posterior dislocation of the hip Ligament to head of femur o Carries artery to head of femur Obturator a. acetabular branch a. to head of femur Bursa Trochanteric -Largest -B/w gluteus maximus and greater trochanter Ischial - B/w gluteus maximus and ischial tuberosity Gluteofemoral -B/w IT band and vastus lateralis Clinical Relevance Damage to the ligament of the head of the femur o Can cause avascular necrosis of the femoral head b/c carries artery to head of femur. Piriformis Syndrome o “Fat Wallet Syndrome” o Peripheral neuritis of sciatic nerve due to impingement by piriformis m. o Associated w/ low back pain and pain that radiates down the posterior leg. Trendelenburg Test o o Positive if hip on leg in swing phase drops b/c gluteus medius and minimus are weak and not able to AB the hip up. o Can be from an injury to the superior gluteal n., fracture of greater trochanter (where gluteus medius/minimus attach), or dislocation of the hip joint. Posterior Thigh Muscles/Actions Posterior Compartment (Hamstrings) Muscles Biceps Femoris Long Head Ischial tuberosity head of fibula Short Head Linea aspera head of fibula Semitendinosus Ischial tuberosity superior medial tibia Semimembranosus Ischial tuberosity posterior medial epicondyle tibia Part of the distal attachment forms the oblique popliteal ligament!! Actions All of the extend the hip EXCEPT: -Short head of bicep femoris ALL of them flex the knee! If lower limb fixed: -Extend the trunk (prevent forward falling) When Knee is 90°: -Semitendinosus and semimembranosus: IR knee -Biceps femoris: ER knee (can rotate laterally more than medially) Gait: -Eccentrically contract during terminal swing to decelerate quadriceps (hip flex/knee extension) OVERALL: The hamstrings extend the thigh and flex then knee but cannot do both motions to maximum contraction simultaneously! o If in full thigh extension then cannot fully flex the knee o If in full knee flexion then cannot full extend the thigh Innervation OVERALL: o Hamstrings are innervated by the tibial division of the sciatic EXCEPT: o Short head of biceps femoris is innervated by the fibular division of the sciatic nerve Clinical Relevance Pes Anserinus o “S sandwich” o Sartorius, Gracilis, Semitendinosus o Hamstring Strain o Usually happens in sprinting when there is rapid lengthening of hamstring during terminal swing Basically, violently slowing down the hamstrings during a sprint vs. the quads are forcefully springing you forward Avulsion Fracture of Ischial Tuberosity o o Hamstrings fully lengthened (thigh flexed and leg extended) o Still an eccentric motion here… same basic mechanics leading to injury as hamstring strain Cruciate Anastomosis o o Composed of lateral and medial circumflex femoral aa., inferior gluteal a., and the first perforating a. of profunda femoris. o If there is a blockage in the external iliac a. and proximal part of the femoral a. then blood can reach the popliteal a. through the Cruciate anastomosis. o Bypass route is: o Internal iliac a. inferior gluteal a. 1st perforating branch descending branch of lateral circumflex femoral a. superior lateral genicular a. popliteal a. Popliteal Fossa Borders: o Lateral border = Biceps Femoris o Medial Border = Semitendinosus/Semimembranosus o Inferior border = Gastrocnemius o Roof = skin and popliteal deep fascia (continuous w/ fascia lata and crural fascia) o Floor = femur, knee joint capsule, popliteus muscle Contents: o Popliteal a. and v. o Sciatic n. bifurcates into common fibular n. and tibial n. o Tibial n. goes straight through the middle of the popliteal fossa o Common fibular n. follows the tendon of biceps femoris m. and curls around the fibular head. Can easily get injured if fracture fibula o Small/short saphenous vein popliteal vein femoral vein Neurovasculature Saphenous n., femoral a. and v. adductor canal (saphenous n. pierces through and leaves) adductor hiatus popliteal a. and v. dive through adductor hiatus to posterior side now in popliteal fossa popliteal a. bifurcates to anterior and posterior Genicular branches arise off of the popliteal a. and form anastomoses around the knee. Clinical Relevance o Hot spot for injury and lots of problems as a result o Acts as a passage for surgeons to get to the knee o Small/short saphenous v. serves as a landmark that makes it easier to find the tibial n. o You follow this vein and the sural n. to find key structures during surgeries o You can take the popliteal a. pulse in the popliteal fossa o Popliteal fascia is extremely tough and does not expand to pressure easily = severe pain if abscess/tumor present o Baker’s (popliteal) cyst o Protrusion of the bursa b/w semimembranosus tendon and medial head of grastrocnemius o Arteriovenous Fistula (AVF) o Abnormal connection b/w artery and vein o Can happen from injuries involving the knee joint or during surgery o Shunts blood from artery to vein blood is not getting to leg can cause necrosis of the leg and foot o AVF also results in a venous aneurysm (bulging) of the popliteal v. Knee and Leg Muscles/actions Anterior Compartment Muscles Actions Tibialis anterior -Dorsiflexion Extensor hallucis longus Tibialis anterior and extensor hallucis longus also do inversion. Lateral tibia medial cuneiform/1st metatarsal Fibula 1st phalange Gait: -Smooth lowering of foot while pulling body over the foot (heel strike) -Toe ground clearance (terminal swing) Extensor digitorum longus Fibula 2nd-5th phalanges Fibularis tertius EDL 5th metatarsal Lateral Compartment Fibularis longus -Eversion -Weak plantar flexion Fibularis brevis Gait: -Prevents excessive inversion (ankle sprain) during swing phase -This holds the medial aspect down during swing phase Fibula 1st metatarsal Fibula 5th metatarsal Posterior Compartment Superficial All muscles distally attach to the Achilles tendon calcaneal tuberosity Gastrocnemius Femoral epicondyles Main: -Plantarflexion Other: -Weak knee flexion Soleus Soleal line of tibia and fibula Plantaris Femur Can’t maximally do both of these actions at once (like hamstrings) Strongest plantarflexor Main: -Plantarflexion Other: -Weak knee flexion Deep Popliteus Lateral femoral condyle soleal line of tibia Flexor digitorum longus Tibia 2nd-5th phalanges IR tibia to unlock the knee from fully extended position Gait: -Crucial for toe off Flexor hallucis longus Fibula 1st phalange Tibialis posterior Tibia/fibula midfoot bones -Main inverter of leg -Support medial longitudinal arch Triceps surae = gastrocnemius and soleus OVERALL: o Posterior compartment are the main inverters of the foot o TA and EHL from the anterior compartment can also invert o All the posterior compartment muscles plantar flex o Actions in the table are the oddball movements o The retinaculum act as a fulcrum for the anterior compartment mm. Innervation Anterior compartment is innervated by the deep fibular n. o Found in b/w tibialis anterior and EDL/EHL Lateral compartment is innervated by the superficial fibular n. Posterior compartment is innervated by the tibial n. Clinical Relevance o The fascia in your leg is so tight to aid your veins in pumping blood back up to the heart o o Fibularis tertius m. may serve to support ATF ligament, which is commonly sprained. o Foot Drop o Severing the common fibular n. = can’t dorsiflex (deep fibular n.) or evert the foot (superifical fibular n.) o Can’t clear toes during swing phase o Compartment Syndrome o Deep compartment of the posterior leg happens more often than in the superficial compartment of the posterior leg. Split by the transverse intermuscular septum o Shin Splints (Medial tibial stress syndrome) o Microtrauma to periosteum of tibia as soleus m. suddenly used/overused o Can also arise from exterional compartment syndrome (muscular hypertrophy… usually ant. Compartment) and stress fractures Ankle and Foot Muscles/Actions Dorsal Compartment Muscles Extensor digitorum brevis Actions -Extend the digits Extensor hallucis brevis Plantar Compartment Layer 1 ABductor digiti minimi -AB 5th digit Flexor digitorum brevis -Flex digits 2-5 ABductor hallucis -AB 1st digit Layer 2 Quadratus plantae -Inserts on FDL tendon to help align pull of FDL Lumbricals -Flex PIP and extended DIP Layer 3 Flexor hallucis brevis -Flex 1st digit Adductor hallucis -AD 1st digit Flexor digiti minimi brevis - Flex 5th digit Two distal heads acts as a channel for FHL Tranverse and oblique head Interosseous Compartment/Layer 4 Plantar interossei -AD (PAD) digits 3-5 Dorsal Interossei -AB (DAB) digits 2-4 3 of them – arise from single metatarsal 4 of them – arise from two metatarsals Innervation Motor Dorsal compartment is innervated by the deep fibular n. Plantar compartment is innervated by the medial and lateral plantar nerves from the tibial n. Medial Plantar n. (purple) Layer 1: -Flexor digitorum brevis -ABductor hallucis Layer 2: -1st lumbrical Layer 3: -Flexor hallucis brevis Lateral Plantar n. (pink) Layer 1: -ABductor digiti minimi Layer 2: -Quadratus plantae -Lumbricals 2-4 Layer 3: -ADductor hallucis -Flexor digiti minimi brevis Layer 4: -All the interossei Sensory Deep and superficial fibular n. both give rise to dorsal digital nerves. Medial and plantar nerves both give rise to plantar digital nerves. Vasculature Dorsal Compartment Anterior tibial a. dorsalis pedis arcuate and lateral tarsal aa. Plantar Compartment Posterior tibial a. ABductor hallucis m. medial and lateral plantar aa. Lateral plantar a. plantar arch All of the neurovasculature to the plantar foot arises under ABductor hallucis m. Ligaments/Joints/Misc Hindfoot = talus and calcaneus Midfoot = cuboid, navicular, and cuneiforms Forefoot = metatarsals and phalanges 1st metatarsal has 2 sesamoid bones under it to protect the FHL tendon Plantar fascia/plantar aponeurosis Protects the sole of the foot, serves as muscular attachment and maintains integrity of the arches Arises from calcaneal tuberosity The foot has many segmented bones to adapt to unleveled ground and to absorb shock so that the rest of the skeleton doesn’t absorb it. The foot also acts as a segmented lever to adapt to unleveled ground. Toe off involves the deep muscles of the posterior compartment of the leg and the segmented lever of the foot. Arches/Arch Supporters Medial longitudinal arch Lateral longitudinal arch Transverse arch 3 major ligaments of the foot: o Long plantar, short plantar, and spring ligament. o They support the medial/lateral longitudinal arches o o Spring ligament also supports the head of the talus Tendons, bones, ligaments, and muscles all help to form the arches. TP and FL tendons criss-cross to help support the transverse arch. Joints of the Foot/Ankle Ankle (talocrural) joint can only do dorsiflexion and plantarflexion! Pronation = dorsiflexion, AB, eversion Supination = Plantarflexion, Inversion, AD o “have to get PAID for soup”…. Use your imagination Toe Movements Metatarsophalangeal (MTP) Joints -Flexion/extension -AB/AD 2nd digit cannot be AB/AD Interphalangeal (IP) Joints -Flexion/extension Subtalar Joint Composed of two joints that are anatomically separate but functionally work together. Actions: -Mainly inversion/eversion -All together do rotation of the foot (inversion/eversion/AB/AD combined) Transverse Tarsal Joint Also composed of two joints. This joint is where the greatest movement of the foot occurs. These joints all form the transverse arch. Also known as Choparts joints. Also known as Lisfranc’s joints. Actions: -where midfoot and forefoot flex/extend -inversion/eversion Actions: -Flexion/extension -Adaptation to uneven surfaces Lisfranc ligament Tarsometatarsal Joints From medial cuneiform base of 2nd metatarsal Crucial to stability of the tarsometatarsal joints. All pass under the tarsal tunnel (flexor retinaculum) TP FDL TA TN FHL Clinical Relevance Amputation o Usually amputate b/w the hindfoot and midfoot at the transverse tarsal joint Plantar Fasciitis o “Painful heel syndrome”… usually point tenderness directly under the calcaneus o Pain w/ great toe extension and dorsiflexion o Overuse injury (running) causing inflammation of fascia o Repeated tearing of plantar aponeurosis can lead to a calcaneal bone spur Foot Infections o Usually caused by a puncture wound o Have to be drained to relieve compartment syndrome o If need a fasciotomy Go in on medial side to avoid scaring on weight-bearing side Pes Planus (flat foot) o Stuck in pronation when walking o Flexible flatfeet = arch present when not bearing weight but flat when walking From loose or degenerating ligaments o Rigid flatfeet = flat when not bearing or bearing weight From bone deformity o Acquired flatfeet = from dysfunction of tibialis posterior Usually spring ligament failure o Lisfranc Injuries o o If injured it affects the entire tarsometatarsal area Dorsalis pedis o Can take pulse (right next to tendon of EHL) o Diminised pulse = possible peripheral a. dz o Deep Fibular n. Entrapment (Ski boot syndrome) o Results in pain in anterior compartment that radiates down to the space in b/w the 1st and 2nd digits. Tarsal Tunnel Syndrome o Space under the flexor retinaculum o Tibial n. can get entrapped there (like median n. and carpal tunnel), which causes tingling and numbness on the sole of the foot. o Gait Cycle Gait Cycle Phase Heel strike (initial contact) Main Action Lower foot to ground Muscles Gluteus maximus (extension/ER) Tibialis anterior (dorsiflexion/inversion) Loading response (foot flat) Accept body weight Quadriceps Gluteus medius and minimus (AB/IR) Midstance Stabilize pelvis Gluteus medius and minimus (AB/IR) Terminal stance (heel off) Accelerate mass Triceps surae (plantarflexion) Stabilize pelvis Gluteus medius and minimus (AB/IR) Grip floor to clear foot Flexor hallucis longus Preswing (toe off) Flexor digitorum longus Initial and mid-swing Terminal swing Accelerate thigh Iliopsoas/rectus femoris (flex thigh) Clear foot Tibialis anterior (dorsiflexion/inversion) Decelerate thigh Hamstrings Extend knee Quadriceps Position foot Tibialis anterior