Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
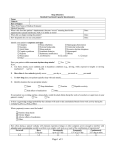
Group Major Illness Medical Information Questionnaire – Treating Medical Specialist Malignant Cancer To be completed by the claimant’s treating medical specialist. This questionnaire is designed to obtain information in relation to a claimant who has been diagnosed with malignant cancer. If there is a cost associated with the completion of the form, it is the responsibility of the claimant. Claimant’s details 1 a. Surname (Family Name) b. Given name/s c. Date of Birth / / History 2 a. How long have you known the claimant? months b. Are you the claimant’s usual treating specialist? Yes No c. Has the claimant been diagnosed with this condition, or any contributing symptoms previously? Yes No 3 years If ‘Yes’, when? / / Details of the claimant’s Major Illness The following questions are designed to assist Zurich in the assessment of the claimant’s insurance claim for Major Illness Benefits. It is important that you provide detailed answers to assist us in our assessment. a. Is there the presence of a malignant tumour, including leukaemia, lymphoma and other haemopoietic malignancies Yes No b. What is your diagnosis of the tumour? Histological examination reports in support of the diagnosis must be provided. c. Has the cancer been classified as carcinoma in situ? Yes No ZU20977 - V2 03/13 - SROE-008692-2014 d. If the claimant has been diagnosed as suffering from melanoma, please state the Clark level depth of invasion. e. If the claimant has been diagnosed as suffering from prostate cancer, what is the TNM Classification or other relevant classification score? f. Please describe the treatment regime the claimant has undergone, or will need to undergo in future, including details of surgeries and interventionist therapies. Malignant Cancer Form – Page 1 of 2 4 Declaration I hereby declare that the above statements are true and correct. Signature of Doctor / Specialist / Consultant Date ✗ / / Name Address Qualifications Telephone number Email Privacy Zurich is bound by the Privacy Act 1988 (Cth). In completing the forms or questions herein you will be providing us with personal and, perhaps, sensitive information. The collection and management of this information is governed by the Privacy Act 1988. For a more detailed explanation of Zurich’s Privacy Policy please visit our website at www.zurich.com.au or contact the Zurich Privacy Officer on 132 687 or email us at [email protected] Please send your completed form to: Zurich Australia Limited Group Risk Insurance Locked Bag 994 North Sydney NSW 2059 Save File Print Form Malignant Cancer Form – Page 2 of 2